
Abstract
Introduction and objective:
Magnetic-assisted robotic surgery (MARS) has been developed to maximize patient benefits of minimally invasive surgery while enhancing surgeon control and visualization. MARS platform (Levita Magnetics) comprises two robotic arms that provide control to an external magnetic controller and an off-the-shelf laparoscopic camera. Our aim was to evaluate the safety and efficacy of the MARS platform in laparoscopic renal and adrenal procedure for the first time.
Methods:
This is a prospective, single-arm, open-label study (Clinical Trials Identifier: NCT05353777) including patients with renal or adrenal pathology analysis, submitted to laparoscopic procedure between April and June 2022. Patients were followed up to 30 days postoperatively. Preoperative, intraoperative, and postoperative data were recorded. Polynomial regression was used to determine the learning curve for docking time.
Results:
Fifteen cases were performed using the MARS platform (three partial nephrectomies, five total nephrectomies for benign pathology analysis, four radical nephrectomies, and three adrenalectomies) corresponding to 10 women and 5 men (mean age, 55 years [18–77]; average body mass index, 29 cm/m2 [22–39]). No cases required conversion to open procedure and all patients were discharged on the first or second postoperative day. No complications or re-admissions were reported within the first 30 days. All oncologic cases had negative margins. Learning curve was achieved by the fourth case, diminishing docking time from 5.22 (2.6–11.5) to 2.68 minutes (2.1–3.8) (p = 0.002). The learning curve was fitted to a cubic regression (R 2 = 0.714).
Conclusion:
This is the first clinical study demonstrating the safety and versatility of the MARS platform in urologic procedures. The robot was especially useful for tissue retraction, avoiding additional incisions and the need for a surgical assistant while increasing surgeon control and visualization. The learning curve was rapid, achieving a short docking time. MARS is a promising new technology that could be successfully evaluated in other surgeries.
Introduction
During the previous decades, minimally invasive surgery (MIS) has become the standard of care for a wide variety of urologic conditions. Compared with open procedure, video laparoscopic procedure (VLP) has demonstrated advantages in reducing postoperative pain, improving cosmesis, decreasing perioperative morbidity, and shortening hospital stays. 1 In addition, it has proven to have the same oncologic outcomes compared with open procedure. 2
For these reasons, open procedure has been almost completely replaced by MIS, leading to further development of new technologies associated with VLP. Nowadays, these advances are mainly focused on robot-assisted laparoscopic procedure. 3 –5
The Levita magnetic surgical system (LMSS; Levita Magnetics) was developed to increase the benefits of MIS while improving tissue exposure during laparoscopic procedures. The LMSS consists of a deployable magnetic tissue grasper that is introduced into the abdominal cavity and manipulated with an external magnet allowing for ideal exposure and avoiding the placement of a laparoscopic port. This system was approved by the Food and Drug Administration (FDA) in 2016 for patients with a body mass index (BMI) between 20 and 34 kg/m2 and has shown to be safe in the manipulation of several organs and tissues. 6
One of the limitations of the original LMSS was the need of an assistant for the movement and positioning of the external magnet to achieve dynamic retraction. 7 The magnetic-assisted robotic surgery (MARS) platform was developed to overcome this limitation and with the intention of increasing control and stability of the visualization. The MARS platform consists of two independent robotic arms fully controlled by the surgeon. One arm incorporates the LMSS, allowing the surgeon to mobilize the external magnet, whereas the second arm holds and manipulates an off-the-shelf conventional laparoscopic camera. The surgeon controls both arms with the same foot pedal. The MARS platform was developed to provide the benefits of LMSS allowing the surgeon to fully control all the instruments during the procedure while decreasing or even eliminating the need for an assistant.
Our objective was to describe, for the first time, the safety and efficacy of the MARS platform in laparoscopic renal and adrenal procedure.
Materials and Methods
Study design
A prospective, single-arm, open-label, ethics committee–approved study was performed at the San Borja Hospital Santiago, Chile (
Patient selection
Adult patients scheduled for laparoscopic renal or adrenal surgeries between April and June 2022 were recruited. Patients with metallic implants (pacemakers or electrotechnical implants) were excluded. All patients signed informed consent. Good clinical practices were strictly followed.
Preoperative (age, gender, comorbidities, BMI), intraoperative (length of operation, bleeding, ischemia time, number of trocars, robotic arms used), and postoperative (length of hospitalization, surgical complications according to Clavien–Dindo classification, ambulatory follow-ups, and pathology analysis in case of renal and suprarenal tumors) data were recorded. All patients were followed up to 30 days after operation.
MARS platform
The MARS platform consists of two independent robotic arms (Fig. 1). The robotic magnetic arm (RMA) carries the magnet used to control the LMSS and the robotic camera arm (RCA) holds the off-the-shelf endoscopic camera, both controlled by the same foot pedal. Each robotic arm is mounted on a wheeled cart and includes a graphical user interface for system setup and management. The Levita robotic platform MARS is designed to allow the surgeon to use the LMSS and directly navigate the camera diminishing, decreasing, or even eliminating the need for an assistant. The LMSS (Fig. 2) consists of a laparoscopic single-use magnetic hand piece with a deployable magnetic atraumatic grasper attached to its distal end. The magnetic grasper is introduced through a 10 mm trocar into the surgical cavity, opened and attached to the desired tissue. Once the tissue is firmly grasped, the handle is squeezed to release the magnetic grasper. The surgeon can modify the position of the grasper by using the foot pedal that controls the RMA.

Levita's MARS platform. The system consists of two independent arms: the RMA that holds the MC of the surgical magnetic system (left) and the RCA that holds the available endoscopic camera (right). Both arms are controlled by the same foot pedal that contains forward/backward, right/left, up/down buttons and a button on the side to switch between robotic arms. Each robotic arm is mounted on a wheeled cart. Both robotic arms RMA and RCA have 7 degrees of freedom and a reach of 820 mm, allowing the robots' end-effector (laparoscopic camera and MC) to be placed in the abdomen area with adequate flexibility for the positioning. The foot controller is designed to be actuated with either foot without needing to visually look at it. This way, the visual attention remains focused in the procedure. MARS = magnetic-assisted robotic surgery; MC = magnetic controller; RCA = robotic camera arm; RMA = robotic magnetic arm. Color image can be found online.

LMSS:
MARS calibration, setup time, and docking
The system needs a pre-setup of <5 minutes before the task, these include setting up configurations specific to the procedure (carts position and scope length), move the robots to the dressing position, dress the robotic arms with sterile drapes, and place the sterile scope holder in the RCA.
When the surgeon is ready to begin and requests the robots, the docking time starts to run. First, both carts are positioned next to the patient in the positions chosen by the surgeon. The wheeled carts have handles that enable four wheels that need to be unlocked to position the cart. After moving the carts into place, a “start” button is pressed to allow the surgeon to have full control over the robots (foot control+hand-guiding). Next, the surgeon needs to connect the scope to the RCA (through the scope holder) and then, using robot hand-guiding, place the tip of the scope within the incision port opened for the camera and press a button to “teach” the pivot point for the device. This is a must-do step to allow the robotic control to correctly move the scope within the abdomen, minimizing the force on the incision. When the pivot point is taught, the docking time finishes.
The robot can be used throughout multiple hours and multiple cases without reducing its performance. Once a procedure is finished, the robots are taken away from the patient table, the scope holder and sterile drapes are removed, and then the robotic arms are moved into storage position, waiting for another procedure to begin.
Surgical technique
Patients were placed in the right or left lateral decubitus positions depending on the operative site (Table 1).
Preoperative Characteristics of Patients and Type of Procedure Performed
BMI = body mass index; NA = not applicable; VLP = video laparoscopy.
The first port was placed with an open technique, and the rest were introduced under direct visualization. The distribution of the trocars was modified from the usual distribution for a nephrectomy to allow better movement of the robotic arms. The trocars were inserted as given in Figure 3. In the case of right-sided surgeries, an additional 5 mm port was used to introduce a hepatic retractor when necessary.

Distribution of the trocars with the MARS platform for left nephrectomy or adrenalectomy. Color image can be found online.
The MARS platform was positioned on the same side of the surgical table as the surgeon, and the RMA on the opposite side (Fig. 4). Before docking the MARS platform, the camera must be assembled to the RCA. After this, the robotic arm is approached and inserted through the camera port.

Distribution of MARS platform in the operating room during left renal surgery. Color image can be found online.
The magnetic grasper was used to retract Gerota's fascia, colon, lateral retraction of the kidney and during dissection of the renal hilum. It was also used for retraction of the tumor during its excision.
Results
Patients
Fifteen patients were recruited, 10 women and 5 men, with a median age of 55 (18–77) years, and an average BMI of 29 (22–39) kg/m2. Table 1 provides patient characteristics, preoperative diagnosis, and surgical procedure.
Proceedings
Ten surgeries for benign pathology analysis and five for malignant pathology analysis, with an average tumor size of 4 (1.5–9) cm were included: three partial nephrectomies with a median ischemia time of 29 (26–32) minutes, five total nephrectomies for benign pathology analysis with a median operative time of 196 (177–295) minutes, four radical nephrectomies with a median operative time of 159 (90–244) minutes, and three adrenalectomies with a median operative time of 123 (120–130) minutes.
The learning curve for docking was achieved by the fourth case, diminishing docking time from 5.22 (2.6–11.5) to 2.68 (2.1–3.8) minutes (p = 0.002). The learning curve was fitted to a cubic regression and obtained an R 2 = 0.714 (Fig. 5).
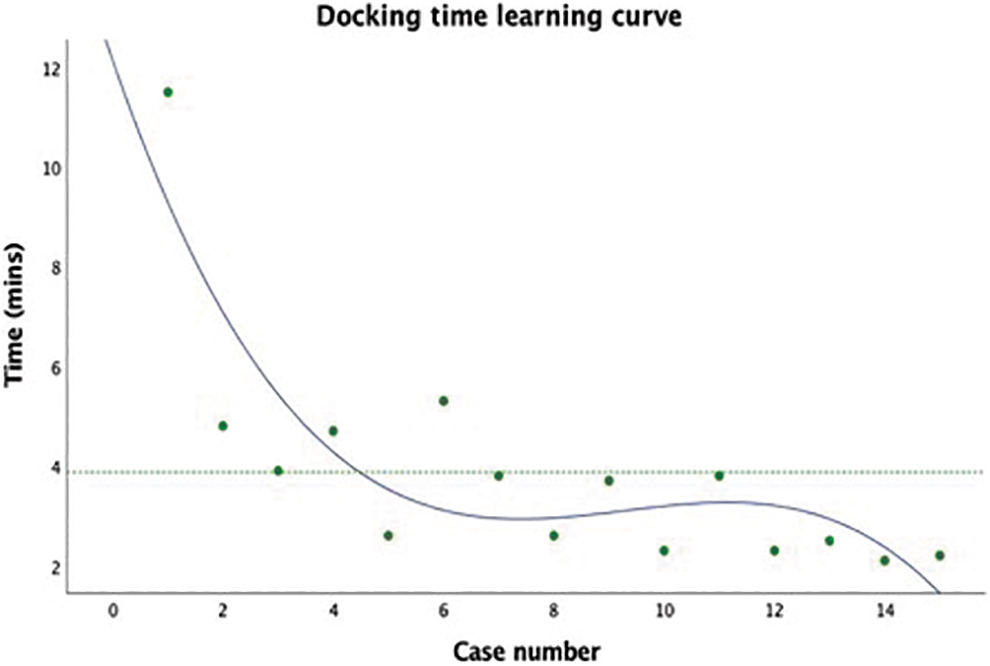
Learning curve of docking time in minutes among consecutive surgeries using the MARS platform. The learning curve was fitted to a quadratic curve regression (R 2 = 0.714). Dashed line represents the mean operative time of docking (referential). Color image can be found online.
The median blood loss for partial nephrectomies was 150 (50–500) mL, for radical nephrectomy 75 (20–100) mL, total nephrectomy 20 (10–300) mL, and adrenalectomy 5 (5–50) mL.
Compared with traditional techniques, all proceedings were performed with one fewer incision and were conducted by the surgeon without an assistant. During the operation, no cases required conversion to open procedure.
After the operation, patients were discharged on the first or second postoperative day, and no complications or re-admissions were reported within the first 30 days.
From the five cancer cases, the histopathological analysis described that all were clear cells renal carcinomas, including one case with sarcomatoid differentiation (pT1a), and two involving the renal vein (pT3a). All cases had negative margins. For cases with benign pathology analysis, three corresponded to angiomyolipoma, four to chronic pyelonephritis with glomerular atrophy, and three to cortical adrenal adenomas. Table 2 summarizes the surgical outcomes.
Surgical and Postoperative Outcomes
ADT = adrenalectomy; CCR = clear cells renal carcinoma; PN = partial nephrectomy; RN = radical nephrectomy; SD = standard deviation; TN = total nephrectomy.
Discussion
This is the first report of the use of the MARS platform in the urologic field.
During the past 30 years, open urologic procedure has been broadly replaced by MIS, which has been improved by ongoing advances in VLP and the introduction of robot-assistedprocedure. 3,5 Although the MARS platform is a new product, the use of magnets in medicine dates to the mid-1880s when the British successfully described ocular foreign body removal using magnets. 7 Nowadays, their use has spread to almost all areas of medicine. The LMSS was first developed in 2016. 7 Since then, it has been used in a wide range procedure, being most used in bariatric. Welsh et al. compared the surgical outcomes of 100 patients that underwent bariatric procedure with LMSS with 196 control cases, 8 reporting that patients operated with LMSS had significantly less pain in the immediate postoperative period and a shorter hospital stay compared with the control group.
In urology, the first publication of LMSS use was in three cases of robot-assisted radical prostatectomies performed without the need of a fourth robot arm, thanks to the exposure provided by LMSS. 9 Meanwhile, the first use of LMSS for renal procedure was published in 2020, 7 consisting of a series of 10 cases that confirmed the safety and versatility of LMSS by performing 5 robotic partial nephrectomies, 2 robotic radical nephrectomies, 1 robotic pyeloplasty, and 2 VLP radical nephrectomies. The main benefit of LMSS was the exposure of the renal hilum during dissection of the uretero-pelvic junction in single-port robotic surgeries, reproducing multiport techniques. However, one of the main disadvantages observed in that experience was the restriction of movement of the external magnet, given it required an assistant for its manipulation.
The idea of being able to free the camera-carrying assistant surgeon has been previously attempted. There are two existing robotic camera holders: one is the assembled robotic arm type holders (SCARA), which consist of three motorized joints in combination to a passive ball joint, and the parallelogram type camera holders, which have three motorized joints, 3 but the one that accounts for the biggest clinical experience is the automated endoscopic optimal positioning system (AESOP®; Computer Motion), a SCARA-type support, which is voice controlled that showed promising results in urologic, gynecologic, and abdominal surgeries. 4 However, AESOP was discontinued in 2003.
With the development of the MARS platform, the original limitations of the LMSS were overcome. We were able to prove several of its advantages in urologic procedures. One is that it allows surgeons to operate without the need for a surgical assistant to handle the camera, enhancing control and improving visualization, as it provides a stable image. This also allows to optimize clinical workflow, liberating a surgeon for parallel cases or additional clinical duties. In addition, the use of the magnet in the MARS platform eliminates the requirement for an extra port, reducing postoperative pain and leading to improved cosmetic results. This groundbreaking technology has proven its safety and versatility in laparoscopic renal and adrenal surgeries, with no cases necessitating conversion to open procedure.
The rapid learning curve achieved after the fourth case further emphasizes the efficiency of the MARS platform. The system is easy to use, and the short docking makes it highly efficient without delaying the usual surgical times.
Since our hospital is a teaching center, the assistant surgeon who holds the camera is usually a resident or less experienced surgeon. With the RCA, common problems such as loss of focus or surgical horizon, erroneous movements, and even camera staining that adds additional time to the case were avoided. Finally, the LMSS was found to be subjectively helpful in all cases and allowed to expose different structures without generating tissue damage. Its safety has been previously proven in gallbladder, liver retraction, Gerota's fascia, perirenal fat, tumor tissue, and colon. 6 Furthermore, MARS platform did not show any limitations when used in patients with BMI up to 39 kg/m2.
None of the 15 surgeries had complications and all the follow-ups performed showed no abnormalities. It is important to emphasize that despite releasing the first assistant from the cases, contact was always maintained in case assistance was required.
Although MARS has clear benefits, there are some areas that need to be considered for optimal clinical use. In patients shorter than 155 cm, the disposition of the trocars is more challenging. Since there is less working space, the trocars must be brought closer together and the RCA may interfere with the urologist's vision. 10 These disadvantages were overcome with the learning curve; however, reducing the size of the platform, with emphasis on the RCA, could be beneficial.
As a promising new technology, further studies are necessary to explore its applicability in other surgical fields. Moreover, the MARS system aims to be highly cost-effective by potentially being more affordable than current robotic platforms and optimizing the utilization of operating room and human resources. 9,10 Although the exact cost of the system's components still has not been defined (it has not yet been released to the market), the combination of clinical benefit, benefit for the patient and its potential cost-saving attributes, will make it valuable in modern medical practices.
Conclusions
In this case series we proved, for the first time, the safety and versatility of the MARS platform for renal and adrenal laparoscopic surgeries. The MARS platform was especially useful in tissue retraction, allowing the primary surgeon to avoid additional incisions and the need for a surgical assistant. There were no complications during the procedure, and until at the 30-day follow-ups, which confirmed the safety of the device. Furthermore, there was a short learning curve for docking time and potential to improve surgical workflow.
The results of this pioneer study are encouraging. Future studies should be considered to assess its applicability in other surgical areas and to confirm the benefits of this new platform.
Footnotes
Acknowledgments
The authors thank all those who contributed to this clinical trial, without whose help and commitment the study could not have been completed. Special thanks to all the personnel of the Urological and Surgical Departments in Hospital Clínico San Borja Arriarán and the Servicio de Salud Metropolitano Centro. Special thanks to Javiera Obreque for monitoring the data and Vivian Soto as the main research coordinator.
Authors' Contributions
F.L.: conceptualization; methodology; validation, formal analysis, investigation, resources, writing—original draft, writing—review and editing, visualization, supervision, project administration. I.F.: conceptualization; methodology; validation, formal analysis. C.R.: conceptualization; methodology; formal analysis. C.M.: conceptualization; methodology; validation, formal analysis, investigation, resources, writing—original draft, writing—review and editing, visualization, supervision, project administration. T.G.: resources, writing—original draft, writing—review and editing, visualization. C.S.: writing—review and editing. J.F.O.: conceptualization; methodology; validation, formal analysis, investigation, resources, writing—original draft, writing—review and editing, visualization, supervision, project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.