
Abstract
Introduction:
Percutaneous nephrolithotomy (PCNL) is the recommended treatment for 2–4-cm renal stones. Minimally invasive PCNL (MPCNL) with ≤22F sheath was frequently used instead of standard PCNL. MPCNL uses pressurized irrigation to flush out stone fragments through a conventional nephrostomy sheath (cNS), which may result in higher intrarenal pressure (IRP) and longer operating time. The novel vacuum-assisted nephrostomy sheath (vaNS) was developed to mitigate higher IRP and to facilitate stone removal. It might improve the performance of MPCNL. This prospective and randomized trial compares these two sheaths.
Materials and Methods:
In total, 120 patients with 2–4-cm renal stones were accrued in six tertiary medical centers with equal numbers in 2021. In total, 120 patients underwent mPCNL, 60 using 18F cNS and 60 using 18F vaNS, in a prospective and randomized assignment. The primary outcome measurement is decrease in IRP. The secondary outcome is efficacy in stone retrieval.
Results:
The IRP was lower with vaNS than with cNS: mean IRP during lithotripsy was 12.0 ± 2.7 mm Hg with vaNS vs 20.4 ± 6.0 mm Hg with cNS, p = 0.000. IRP duration ≥30 mm Hg was shorter with vaNS than with cNS (6.7 ± 7.4 seconds vs 113.4 ± 222.7 seconds, p = 0.001). vaNS has shorter stone removal time (26.9 ± 14.3 minutes vs 35.7 ± 11.8 minutes, p = 0.000). Stone extraction rate was higher (166.4 ± 88.1 mm3/min vs 90.4 ± 31.7 mm3/min, p = 0.000). Stone grasper usage was less (1.4 ± 2.6 vs 11.9 ± 9.7, p = 0.000). vaNS maintained the safety profile. Blood loss, creatinine changes, perioperative complications, and hospital stays were the same in both groups, all p > 0.05.
Conclusion:
MPCNL for stones 2–4 cm using vaNS has shorter stone removal time, higher stone extraction rate, and less use of stone extractor. vaNS is superior to cNS at reducing IRP and is associated with improved stone free rates at 3 days but not at 30 days postoperatively. The trial was registered with Chinese Clinical Trial Registry (ClinicalTrials.gov, NCT ChiCTR2000039681).
Introduction
Percutaneous nephrolithotomy (PCNL) is the recommended treatment for renal stones >2 cm in size per American Association of Urology (AUA) and European Association of Urology (EAU) guidelines. 1,2 There is a trend toward using a smaller sheath to perform PCNL for its perceived lesser trauma to the kidney. Although minimally invasive PCNL (MPCNL) does have the advantages of less blood loss and shorter hospitalization, it also has the disadvantages of higher intrarenal pressure (IRP), longer operative time, higher postoperative complications, and lower stone-free rate (SFR). 3 –5 During the past few years, Professor Shaw Wan unveiled a vacuum-assisted nephrostomy sheath (vaNS), the ClearPetra (Well Lead Medical, China) (Fig. 1). 6,7
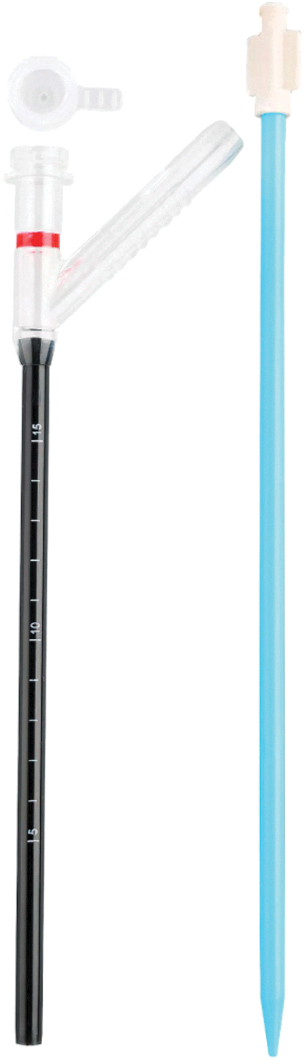
The vacuum-assisted nephrostomy sheath.
The primary objective of this novel device is to reduce the IRP during MPCNL. The secondary objective is to improve the efficacy of extracting stone fragments (pers. commun., Shaw P. Wan, 2013). The vaNS has a 45° oblique side branch that can be attached to a vacuum equipment. It allows continuous and active aspiration of irrigation fluid. A 14 mm longitudinal pressure vent in the form of a slit (Fig. 2) located on this side branch enables the operator to adjust the vacuum pressure.
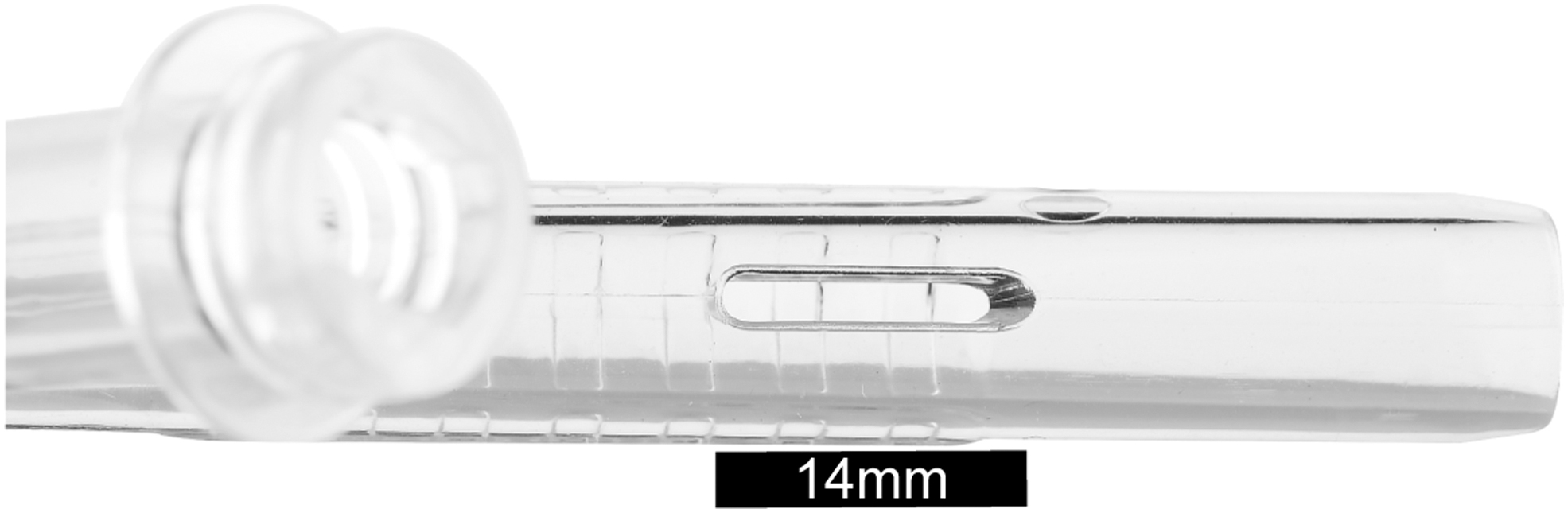
A 14-mm longitudinal pressure vent.
The methodology of withdrawing the endoscope to proximal to the takeoff of the side branch opens an unimpeded channel for active aspiration of stone fragments. vaNS may mitigate some of the deficiencies of the conventional nephrostomy sheath (cNS) in the treatment of 2–4-cm renal stones. To prove this hypothesis, we embarked on this multicenter prospective and randomized trial (Fig. 3).
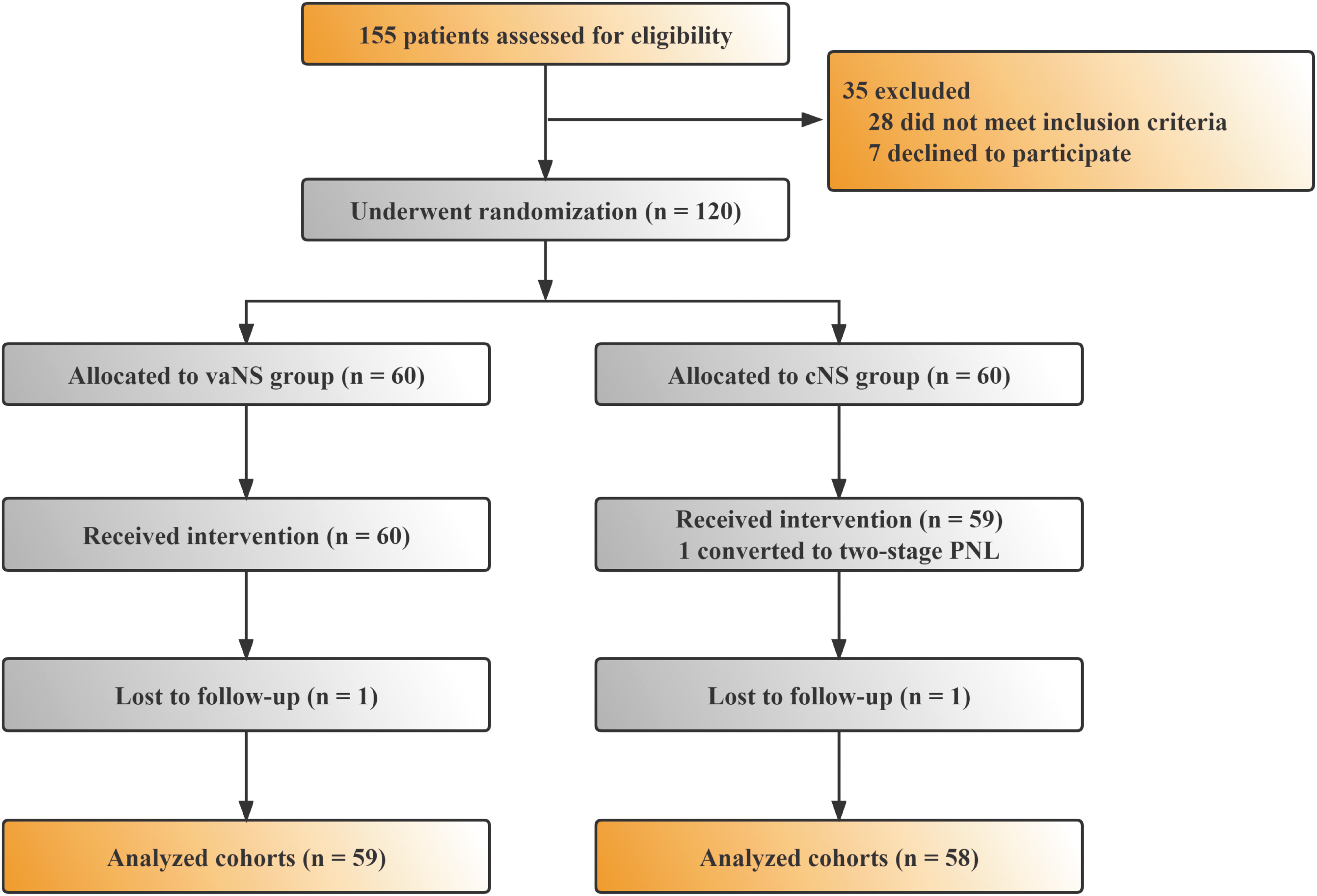
Trial flow chart.
Since the primary objective of vaNS is to lower the IRP during MPCNL, we chose the difference in the mean peak IRP between the two different nephrostomy sheaths as the primary outcome measurement. The secondary outcome measurement is the efficacy in extracting stones. We are cognizant that the most important aspect in evaluating a new device or procedure for any stone surgery is SFR. However, PCNL procedures have become standard armaments in the urologic surgery repertoire. Most experienced surgeons performing these procedures can achieve high SFR with low complications. If one uses SFR or complication rate as the primary outcome, it will require a large sample size, probably >1000 patients, to show any statistical differences. This would be outside the scope of this study.
Materials and Methods
This is a multicenter, parallel, open-label, and randomized and controlled trial (RCT). In total, 120 patients were recruited from 6 tertiary medical centers from February 2021 to October 2021. All participating centers have similar expertise in performing PCNL and generally do >500 PCNLs per year. Ethics committee approval was obtained at each participating institution and a written informed consent was received from each patient.
The primary outcome was reduction of mean peak IRP. Secondary outcomes included occurrence time of IRP ≥30 mm Hg, efficacy in stone extraction, blood loss, change in creatinine, operative time, perioperative complications, and hospital stay.
Our sample size was calculated based on these premises. We used the “Tests for Two Means in a Multicenter Randomized Design” in the PASS 15 software to calculate the sample size. 8,9 The reported peak IRP was 55.1 mm Hg for the conventional nephrostomy sheath (cNS) group, and 28.1 mm Hg was the hypothesized peak IRP in the vaNS group. A sample size of 17 per center could achieve a 90% power to detect a difference of 27.000 between the two means, with a standard deviation of 18.000 for the corresponding variables. The intraclass correlation coefficient (ρ) of 0.100 was used to test the significance level of 0.050 from a mixed effects model, which was suitable without the treatment-by-center interaction.
Using a 95% confidence interval and an α error of 5%, the minimum sample size for each center was estimated to be 17 patients. With a 1:1 ratio for group comparison and estimated 10% loss, 19 patients were required to provide a 90% power for this study. We increased the sample size to 20 to provide a margin for error, thus, 120 patients for the 6 participating centers. Inclusion criteria were patients 18 years of age or older with renal stones 2–4 cm in size, no evidence of urinary tract obstruction, normal renal function, no previous open renal surgery, and informed consent.
Exclusion criteria were American society of Anesthesiologists (ASA) III or higher on preoperative assessment; uncorrected coagulopathy; renal or anatomical anomalies that precluded MPCNL; uncontrolled comorbidities such as diabetes, hypertension, or urinary tract infection; and refusal to participate in the study. In total, 155 consecutive patients with 2–4-cm stones were evaluated. In total, 120 patients were eligible and entered the randomization with 60 patients per group. One patient from each of the cNS and vaNS groups was lost on follow-up and were excluded. One patient from the cNS was excluded for conversion to a two-stage PCNL because of an intraoperative cardiopulmonary event.
Ultimately, 117 patients completed the study, and their data were analyzed. A computer-generated randomization table with 120 binary numbers in 1:1 ratio was used. A central coordinator revealed the random assignment to each surgeon just before commencing the procedure. All centers approved a pre-established and uniform operating methodology. All patients underwent standardized preoperative preparation. These included noncontrasted and/or contrasted CT studies. PCNL was performed under either general or epidural anesthesia. The surgery started in lithotomy position with retrograde insertion of an already calibrated 6F open-ended ureteral catheter to just above the ureteropelvic junction and confirmed with contrast fluoroscopy.
The patient was next turned into prone position. Catheter position was reconfirmed. The inserted ureteral catheter with its extension tubing was connected to a pressure transducer, leveled with the affected kidney, and primed. It was then connected to a continuous pressure-monitoring machine (IntelliVue, Philips). The baseline pressure was set to 0 and the pressure-monitoring range was set at 0–200 mm Hg. It should be emphasized that we were not measuring the innate IRP. Rather, this was a pressure comparison study. IRP was continuously monitored and recorded. A caliceal puncture was achieved using combined fluoroscopic and ultrasonic images. A 0.035″ guidewire was inserted into the punctured calix and, if possible, manipulated down into the ureter.
One-step or multistep fascial dilation was performed to 20F. An 18F cNS or vaNS was inserted over the obturator. A 12F mininephroscope with 6F working channel, 22.5 cm in length (Wolf, Germany), was introduced through the sheath to observe the stones. The irrigation was delivered using a mechanical pump with a setting of 260 mL/min. flow rate and a maximum irrigation pressure of 275 mm Hg in all the procedures. This setting was based on our experience and reports. 10,11 The high flow rate was selected to ensure clear vision and effective flushing of stone fragments. The upper limit for irrigation pressure was set for safety consideration.
Lithotripsy was performed using holmium laser lithotripters with 550-μm fibers. The laser power was set at 40 Watts (20 Hz × 2.0 J). For the cNS group, stone fragments were removed using either pressurized irrigation or a stone extractor. For the vaNS group, the stone fragments were removed with suction. Use of the stone extractor was permitted. The vacuum pressure was set at 200 mm Hg. Our in vitro experiment showed that this vacuum pressure and 50% coverage of the vent on the oblique side port of the vaNS resulted in equal volumes of ingress and egress of the irrigation fluid.
With complete covering of the pressure vent, the egress increased over the ingress accordingly. The withdrawal of the endoscope to proximal to the takeoff of the side port allowed the removal of the larger stone fragments. A 6F Double-J stent and a nephrostomy tube were placed at the end of procedure. To measure the volume of the extracted stone, the fragments were placed into a graduated container that was calibrated to 0.1 mL and filled with water. The amount of water displaced denoted the stone volume.
The stone removal time was set from the beginning of the holmium laser lithotripsy to the ending of extraction of all visible stone fragments. The stone extraction rate refers to the volume of stones removed per minute, which is calculated by dividing the total number of stones extracted by the stone removal time.
Removed stones were sent for analysis. Initial SFR was assessed by limited CT on the third postoperative day. Secondary procedure would be planned for patient with significant or symptomatic residual stones. Final SFR was assessed 1 month later. Patients with no residual stone on the 3-day CT was not re-evaluated. Patients with limited residual stones, kidney, ureter, and bladder radiograph and/or ultrasonography were performed and compared with the previous CT. Repeated CT scans were done only if clinically indicated.
SFR is assessed based on the new grading system: Grade A: absolute stone free (no stones on CT scan), Grade B: relative stone free (≤2 mm fragments), and Grade C: relative stone free (2.1–4 mm fragments). Perioperative complications were assessed using the modified Clavien–Dindo grading system.
Statistical analysis
Continuous variables were compared using either a two-sided t-test or a Wilcoxon rank sum test. Categorical variables were compared with either the chi-squared test or Fisher's exact test. A p-value <0.05 was considered statistically significant. SPSS 23.0 software was used for this analysis.
Result
In total, 155 patients were eligible to enter the study; 28 did not meet inclusion criteria; and 7 were excluded for nonconsent.
Demographic data of the cohorts are given in Table 1. There were no significant differences in gender, age, body mass index, comorbidities, or urine culture results.
Patients' Demographics
BMI = body mass index; cNS = conventional nephrostomy sheath; SD = standard deviation; vaNS = vacuum-assisted nephrostomy sheath.
Stone characteristics are given in Table 2. There were no significant differences in stone locations, stone sizes, CT HU, S.T.O.N.E. scores, or stone compositions between these two groups.
Stone Characteristics
Detailed efficacy data are summarized in Table 3. Most punctures were performed in the central region. The stone removal time was significantly shorter in the vaNS group. The stone extraction rate was significantly greater, and the use of stone grasper was significantly less in the vaNS. The baseline IRP was the same in both groups. There were significantly lower mean IRPs for the vaNS group during lithotripsy. There were also significant shorter durations where the IRPs were >30 mm Hg for the vaNS group. Other pressure parameters also favored the vaNS group. The lowest recorded IRPs were −7.9 ± 17.1 mm Hg vs 9.3 ± 6.5 mm Hg, and the highest recorded IRPs were 32.5 ± 7.9 mm Hg vs 61.6 ± 33.5 mm Hg, for vaNS and cNS, respectively.
Operative Data
Grade A (no stones on CT scan), absolute stone free, Grade B (≤2 mm fragments) relative stone free, and Grade C (2.1–4 mm) fragments relative stone free.
IRP = intrarenal pressure; SFR = stone-free rate.
There were no significant differences in the volumes of the removed stones.
SFR data were classified into three grades as depicted in Table 3. The 3-day Grade A SFR favored the vaNS (72.9% vs 53.3%). The 30-day Grade A SFR was similar in both groups, 86.4% vs 74.1%. There were no SFR differences in Grades B and C. On day 3, the mean diameter of the residual stones in the cNS group was 2.1 mm; it was 1.3 mm in the vaNS group.
On day 30, the mean diameter of residual stones in the cNS group was 1.1 mm; it was reduced to 0.4 mm in the vaNS group. There were three patients in the cNS group with residual stones >6 mm that required secondary procedure. Two underwent retrograde ureteroscopy and one elected extracorporeal shockwave lithotripsy. No patient in the vaNS group needed further intervention.
Safety data are depicted in Table 4. There were no differences in blood loss, creatinine changes, perioperative complications, and hospital stays; all p > 0.05. One patient in each group received a hemostatic agent for moderate blood loss, but no transfusion was required. One patient in the cNS group required selective arterial embolization to achieve hemostasis.
Safety Data
Grade I: fever = T > 38.3°C, Grade I: hemorrhage = use hemostatic drugs, Grade IIIb: hemorrhage = vascular interventional embolization.
Discussion
High IRP should be a concern in any endoscopic intrarenal surgery. High IRP is often not recognized unless peri- or postoperative complications have occurred. Sequelae of high IRP include pyelovenous reflux, perirenal extravasation, intrarenal bleeding, and renal tubular fibrosis.
There were several publications between 2016 and 2022 touting the benefits of vacuum-assisted PCNL. Two meta-analyses by Li et al. and Zhu et al. compared vaNS and cNS in MPCNL. 12,13 Both concluded that vaNS could result in better SFR, fewer auxiliary procedures, shorter operation time, and less postoperative infection.
Lai and colleagues reported the result of using vaNS vs cNS in patients with pyonephrosis secondary to obstructive calculous in a single-center RCT. 14 vaNS patients had higher initial SFR, shorter operative time, and fewer postoperative complications.
Xu et al. in another single-center RCT reported using 18F vaNS vs cNS in the treatment of staghorn stones. 15 They showed that the vaNS group had a significantly lower peak and mean IRP throughout the procedure. The vaNS group also had a shorter lithotripsy time, lesser use of the stone extractor, and a higher SFR.
Our data demonstrated that vaNS is superior to cNS in terms of maintaining lower IRP during lithotripsy and higher efficacy in extracting stones. Studies have demonstrated that pyelovenous backflow occurs when the IRP is >30 mm Hg. 16,17 In an infected environment, influx of bacteria and endotoxins into the bloodstream may occur and result in systemic inflammatory response syndrome and sepsis. 18 The IRPs with vaNS, except for mean peak IRP, were generally well below this threshold. Furthermore, the risks for pyelovenous backflow are proportional to the peak and the cumulative time that the IRP is ≥30 mm Hg.
The mean peak pressure was 32.5 mm Hg and the cumulative time of IRP ≥30 mm Hg was only 6.7 ± 7.4 seconds for the vaNS group. Our cNS group did show a trend toward higher incidence of postoperative fever. However, since both groups had low complication rate, we could not demonstrate any statistical significance.
Recently there are more interests shown for vacuum-assisted lithotripsy. Sur and colleagues reported using a fluoroscopic guided steerable ureteroscopic renal evacuation sheath (the CVAC™ system) to aspirate the residual stones after laser lithotripsy. They compared this system with basket extracting of stone fragments. 19 They demonstrated superior stone clearance; at 30 days, aspiration technique achieved a 100% SFR, whereas basketing achieved only 75%. However, because of the limited sample size, this difference did not reach statistical significance.
Our final SFR did not show any differences between the groups according to the grades. Nevertheless, vacuum-assisted lithotripsy is more effective in removing stone fragments as witnessed by the higher immediate SFR. Many patients will be able to pass small residual stone fragments postoperatively, especially if they are not in the lower calices. With the improved lithotripsy technique, bigger residual stones are rarer nowadays; thus, a large sample size would be needed to demonstrate any significant SFR at 30-day follow-up.
Our longer hospitalization time is because of our low cost of hospitalization, our national health insurance policy of reimbursing only inpatient expenses, and the long distance patients must travel. Most patients would not agree to be discharged until they were well recovered, and all the external tubes removed.
The limitation of this study was the relatively small number of participants. A larger sample size might be able to demonstrate differences in SFR and postoperative complications.
Conclusion
vaNS can maintain lower IRP, shorter operating time, and higher efficacy in stone extraction during MPCNL than cNS without sacrificing SFR and safety profiles. Therefore, vaNS should be favorably considered when performing MPCNL for 2–4-cm renal stones.
Footnotes
Authors' Contributions
S.L., X.D., J.L., X.Z., R.L., Y.Z., and G.X. conceived and designed the study. S.L., X.Z., Y.C., H.W., Z.C., Y.Z., and H.Z. performed the data collection. S.L., X.D., J.L., X.Z., R.L., Y.Z., Z.C., and G.X. analyzed the data and reviewed and revised the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the Key Clinical Specialty Project of Guangdong Province (2022), Characteristic Technology Project of Guangzhou Municipal Health Commission (No. 2023C-TS50), Key Laboratory of Guangdong Higher Education Institutes (2021KSYS009), and Guangzhou Key Laboratory of Biological Targeting Diagnosis and Therapy (No. 202201020379).