
Abstract
Introduction:
A flexible cystoscope is an indispensable tool for urologists, facilitating a variety of procedures in both the operating room and at bedside. Single-use cystoscopes offer benefits including accessibility and decreased burden for reprocessing. The aims of this study were to compare time efficiency and performance of single-use and reusable cystoscopes.
Methods:
Ten new Ambu® aScope™ 4 Cysto single-use and two Olympus CYF-5 reusable cystoscopes were compared in simulated bedside cystoscopy and benchtop testing. Ten urologists performed simulated cystoscopy using both cystoscopes in a randomized order. Times for supply-gathering, setup, cystoscopy, cleanup, and cumulative time were recorded, followed by a Likert feedback survey. For benchtop assessment, physical, optical, and functional specifications were assessed and compared between cystoscopes.
Results:
The single-use cystoscope demonstrated shorter supply-gathering, setup, cleanup, and cumulative times (824 vs 1231 seconds; p < 0.05) but a comparable cystoscopy time to the reusable cystoscope (202 vs 212 seconds; p = 0.32). The single-use cystoscope had a higher image resolution, but a narrower field of view. Upward deflection was greater for the single-use cystoscope (214.50° vs 199.45°; p < 0.01) but required greater force (2.5 × ). The working channel diameter and irrigation rate were greater in the reusable cystoscope. While the single-use cystoscope lacked tumor enhancing optical features, it had higher Likert scale scores for Time Efficiency and Overall Satisfaction.
Conclusion:
The single-use cystoscope demonstrates comparable benchtop performance and superior time efficiency compared to reusable cystoscopes. However, the reusable cystoscope has superior optical versatility and flow rate. Knowledge of these differences allows for optimal cystoscope selection based on procedure indication.
Introduction
Cystoscopes have evolved since their inception in 1805 from unwieldy instruments lit by candlelight into sophisticated tools facilitating advanced procedures. 1 However, traditional endoscopes are limited by high purchase and maintenance costs and time-consuming processing and sterilization. 2,3 Furthermore, repeated sterilization can degrade image quality, and if done inadequately, may increase a patient's risk of infection due to cross-contamination. 4,5 These factors have prompted further innovation, resulting in the development of single-use disposable cystoscopes.
Single-use cystoscopes offer unique advantages including their sterile nature out of the package, on-demand availability, maintenance-free operation, and compatibility with portable screens instead of large video towers. 6 –8 These features make them especially well-suited for time-sensitive procedures. However, given the novelty of single-use cystoscopes, few studies have evaluated their performance compared to reusable cystoscopes, especially with respect to time efficiency. 9,10 The purpose of this study was to compare single-use and reusable flexible cystoscopes with respect to physical and optical performance, time efficiency, and physician satisfaction.
Methods
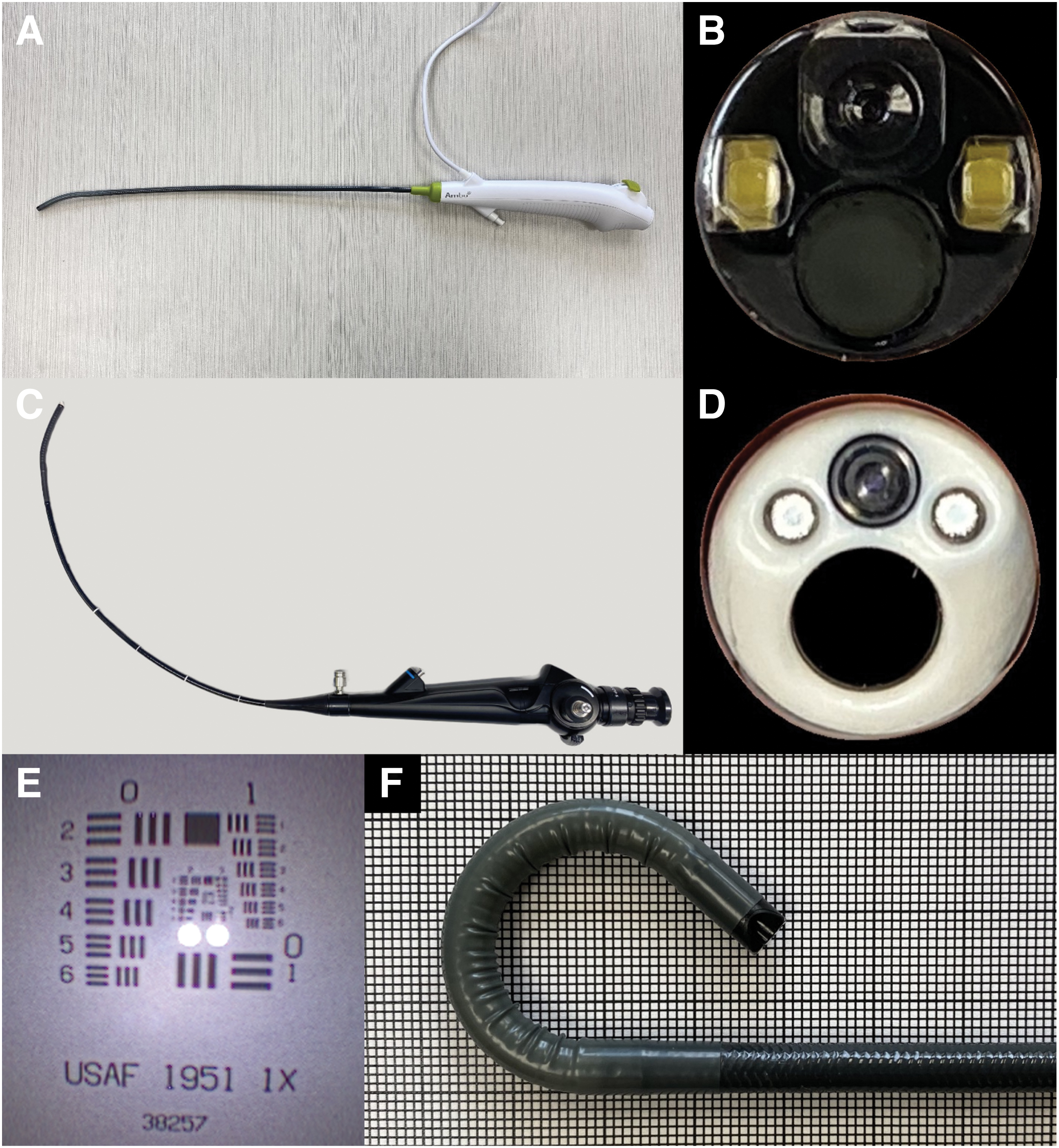
Ten new single-use aScope™ 4 Cysto (aS4C) cystoscopes (Ambu, Denmark) and two reusable current standard-of-care CYF-5 Cysto-Nephro Fiberscopes (Olympus, Center Valley, PA) were assessed for time efficiency, benchtop performance, and user satisfaction during a simulated bedside cystoscopy done after hours (Fig. 1). Ten urologists, including five attendings (two endourologists, two endourology fellows, and one general urologist) and five residents (two PGY-2, one PGY-3, and two PGY-4), participated in the study.
Time efficiency testing involved performing a simulated cystoscopy on a patient model. The model consisted of a female pelvis mannequin with a three-dimensional silicone bladder, which was 3D printed from a human bladder CT scan (Fig. 2). 11,12 The model was placed on an intensive care unit (ICU) bed to replicate a clinical environment. Participants were responsible for gathering all necessary supplies, setting up, and returning the equipment after each cystoscopy. In addition to the cystoscope, the necessary supplies for the reusable system included the video tower, light cord, and camera compared to only the portable monitor for the single-use system. These items were stored in the operating room located on a different floor than the ICU. General supplies for cystoscopy including irrigation tubing, normal saline, lubricant, drapes, and gloves were stored in the same room as the patient model. During cystoscopy, the participants were required to complete a target identification task by locating 22 equally distributed letters on the inner surface of the bladder. Letters were positioned throughout the bladder including the internal surface of the bladder neck, requiring full retroflexion of the endoscope to identify all letters. Each participant performed two trials in a randomized order, one with the single-use cystoscope and one with the reusable cystoscope. Following both trials, the participants completed an online survey using Qualtrics XM, consisting of a 10-point Likert scale (10 representing the highest satisfaction) to assess user feedback regarding six domains for each scope: Confidence in Sterility, Time Efficiency, Maneuverability, Image Quality, Cystoscopy Time and Overall Satisfaction.
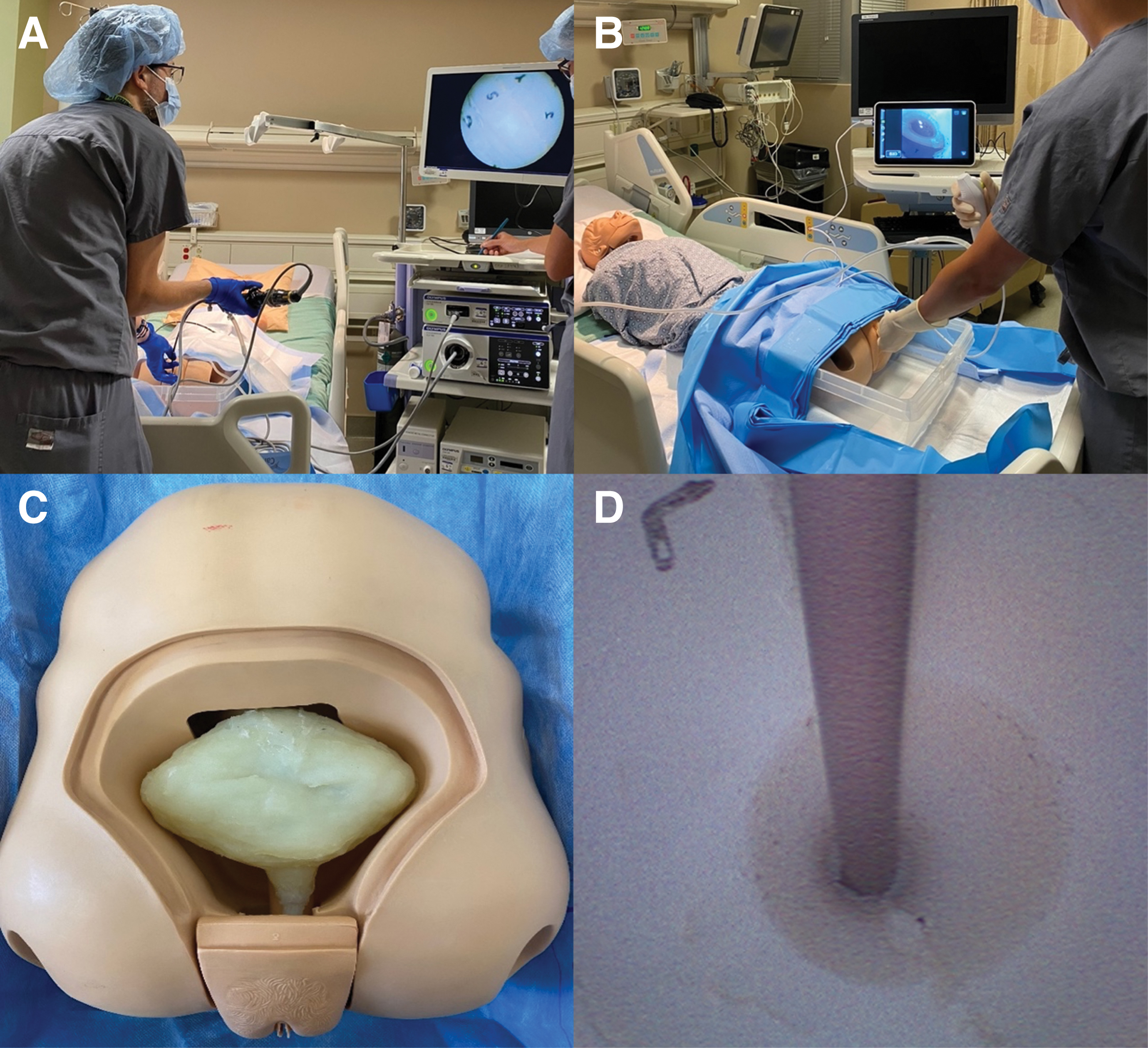
Cystoscopy with target identification task performed in an ICU room with
Four separate time intervals were measured: supply-gathering, setup, cystoscopy, and cleanup time. Supply-gathering time referred to the duration between leaving the starting position and entering the patient's room with all necessary equipment. Setup time was defined as the time from entering the patient's room to inserting the cystoscope into the urethral meatus. Cystoscopy time was the duration from cystoscope insertion to completion of target identification. Cleanup time was the period from completing target identification to returning all equipment to the storage room.
In vitro optical resolution testing was performed using a 1951 U.S. Air Force test pattern grid (Edmund Optics, Barrington, NJ) at 15 mm under controlled lighting conditions. 13 This reports resolution in line pairs/mm (lp/mm), reflecting the number of lines that can be distinguished per mm, with a higher lp/mm indicating better resolution. Field of view (FOV) testing was also conducted with both single-use and reusable cystoscopes using a protractor and reported in degrees (°) as previously described by Marchini et al. 14 Resolution and FOV testing were completed using both viewing options for the reusable cystoscope: the built-in eyepiece and video tower monitor. Both tests were conducted outside the bladder model in a controlled laboratory setting. Any user-adjustable optical settings were noted for each cystoscope.
Maximum upward and downward deflection testing were completed with an empty working channel in both cystoscopes. Force required for maximum deflection, 180° upward, and 90° downward with an empty channel was measured using an ES10 force gauge (Mark-10, Copiague, NY). 15 The irrigation rate was determined by suspending normal saline at a height of 2 m and measuring the time to empty 500 mL through an empty channel. 16 Physical testing involved measuring specifications including cystoscope mass (without light cord), working channel length, proximal and distal cystoscope outer diameter, and working channel diameter.
Statistical analysis using the Mann–Whitney U test was performed for upward and downward deflection, force required for deflection, FOV, irrigation rate, cystoscope mass, working channel length, and proximal and distal cystoscope outer diameter comparing the single-use and reusable cystoscopes. A paired Wilcoxon signed-rank test was performed for time efficiency and Likert scale satisfaction survey comparing both cystoscopes. All statistical analyses were performed using SPSS version 24 (IBM, Armonk, NY). The significance threshold was set at p < 0.05.
Results
The single-use cystoscope required less time for supply-gathering (187 vs 266 seconds), setup (211 vs 300 seconds), cleanup (183 vs 296 seconds), and cumulative time (824 vs 1231 seconds) compared to the reusable cystoscope (p < 0.05 for all) (Fig. 3). The time required for cystoscopy was similar between the single-use and reusable cystoscope (202 vs 212 seconds; p = 0.32). There was no difference in times between residents and attendings for any stage (p > 0.05).
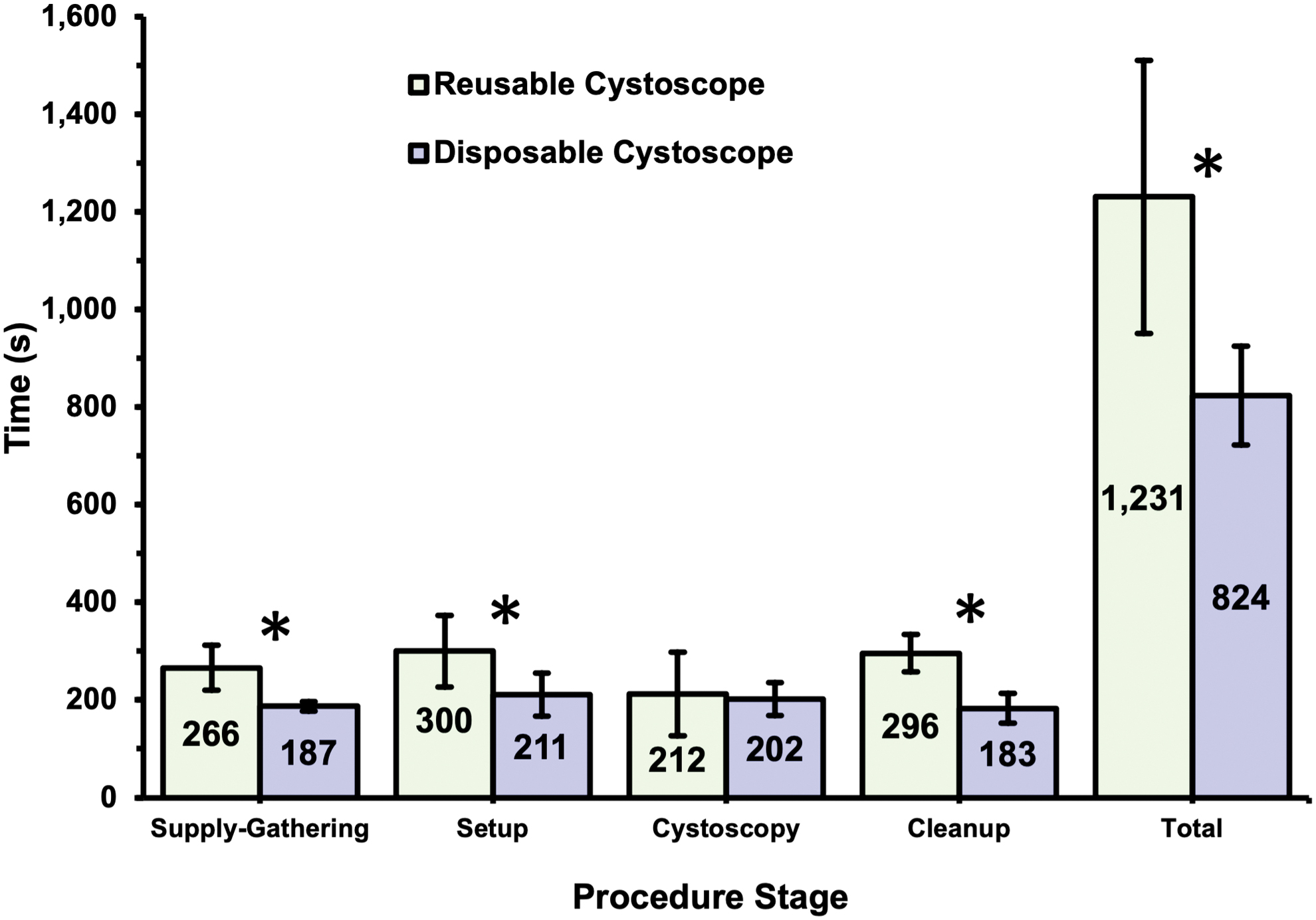
Median time for supply-gathering, setup, cystoscopy, cleanup, and cumulative time. Error bars represent interquartile ranges. *p < 0.05. Color images are available online.
The single-use cystoscope had a superior median resolution of 6.35 lp/mm compared to both viewing options for the reusable cystoscope (p < 0.01). The reusable cystoscope tower monitor had a resolution of 2.0 lp/mm and was lower than its built-in eyepiece resolution of 3.56 lp/mm (p < 0.01). The reusable cystoscope had a wider FOV of 107.8° for the tower monitor and 104.0° for the built-in eyepiece than the 66.54° for the single-use cystoscope (p < 0.01). User-adjustable optical settings such as focus, white balance, and narrow band imaging were available for the reusable but not for the single-use cystoscope.
The single-use cystoscope produced a median maximal upward deflection of 214.5° and a downward deflection of 181.5° (Table 1). In comparison, the reusable cystoscope produced a median maximal upward deflection of 199.45° and a downward deflection of 110.25° (p < 0.01). The single-use cystoscope required greater force for maximal upward deflection (21 vs 8 N) but less force for maximal downward deflection (5.9 vs 6.3 N; p < 0.05 for all). At 180° downward and 90° upward deflection, the single-use cystoscope required greater force (p < 0.05). Irrigation rate with an empty working channel was higher for the reusable cystoscope at 495.9 mL/min compared to 389.61 mL/min for the single-use cystoscope (p < 0.01). The mass of the single-use cystoscope was less than the reusable cystoscope (Table 1). For working length, the single-use cystoscope was longer at 38.98 cm compared to 37.45 cm for the reusable cystoscope. The proximal outer diameter for the single-use cystoscope was smaller at 5.2 mm than the reusable cystoscope at 5.46 mm, but the insertion tube outer diameter was comparable between the two cystoscopes (5.56 vs 5.55 mm; p = 0.73). The reusable cystoscope had a wider working channel diameter of 2.5 mm compared to 2.24 mm for the single-use cystoscope (p < 0.01).
Physical, Optical, and Functional Performance of the Single-Use aScope 4 Cysto and Reusable CYF-5 Cysto-Nephro Fiberscope
Bold indicates significant p-value.
FOV = field of view; IQR = interquartile range; lp/mm = line pair/millimeter; n = number of patients; N = newton.
Survey data for 10 participants was recorded. The single-use cystoscopes were rated higher on Time-Efficiency and Overall Satisfaction (p < 0.05) (Table 2). Ratings for Confidence in Sterility, Maneuverability, Image Quality, and Cystoscopy Time were good for both cystoscopes with no significant differences (p > 0.05).
Likert Scale Participant Feedback
Bold indicates parameters representing statistical significance.
Discussion
The single-use flexible cystoscope performed well in both benchtop assessment and a simulated bedside cystoscopy. Use of the disposable cystoscope took 67% of the cumulative time compared to the reusable cystoscope. This may be due to lighter equipment requirements, which consists of only a portable monitor and the cystoscope itself as opposed to the reusable cystoscope which requires a bulky video tower, light cord, and camera. One of the major differences in time was due to transport of the heavy video tower for the reusable cystoscope. Furthermore, accounting for processing and sterilization may generate even greater time savings for the single-use cystoscope. Reducing perioperative procedure times for the single-use cystoscope may offer benefits in time-sensitive clinical scenarios.
Both single-use and reusable cystoscopes demonstrated comparable times for cystoscopic target-identification intended to simulate bladder screening. This suggests that the two devices have comparable functionality for the purpose of a limited bladder examination. However, the single-use cystoscope was noted to lack lesion-enhancing features present in the reusable cystoscope, such as narrow band imaging. This deficit may affect the single-use cystoscope's ability to detect bladder lesions. In a study comparing a different single-use (Isiris) and reusable flexible cystoscope, Seyam et al. reported no significant difference in bladder cancer detection rates. 17 However, the study did not specify whether the reusable cystoscope utilized tumor-enhancing optical features, which may affect lesion-detecting ability.
In addition to reducing perioperative times, the single-use cystoscope may offer other significant advantages in the acute inpatient setting, particularly for difficult catheterizations due to stricture disease or false passages. At many sites, including ours, there are restrictions on using large independent cystoscopy towers outside the operating room. As a result, cystoscopy with wire placement is performed through the eyepiece of the cystoscope, limiting direct vision of the pathology to only the operating surgeon. Lack of direct vision for inpatient assistants, who are often not urology attendings or residents, poses significant challenges to successful wire placement. This often prolongs procedure time and increases patient distress. However, the portable monitor of the single-use cystoscope provides the same visualization to the assistant managing the wire, often enabling a more efficient procedure.
In a recently published prospective randomized trial, Holmes et al. reported comparable total procedure and operating room times between a single-use aS4C and a reusable Olympus CYF-VH flexible cystoscope for diagnostic or bladder cancer surveillance purposes. 10 Effective completion of the procedure, image quality, lighting, and maneuverability was also comparable between both cystoscopes. While there was no difference in total procedure and operating room times, the study was set solely in the operating room, which entails a different supply, setup, and cleanup process than the bedside cystoscopy simulated in our benchtop model.
The single-use cystoscope demonstrated higher optical resolution than both the built-in eyepiece and video tower monitor for the reusable cystoscope. Notably, the eyepiece of the reusable cystoscope had higher resolution than its monitor. However, as described above, utilizing the eyepiece adds an extra layer of complexity to the procedure when performing cystoscopy with additional interventions such as wire placement in the acute setting. Similarly, Whelan et al. reported that the single-use aS4C cystoscope showed higher resolution than a reusable standard definition Olympus CYF-V2 cystoscope. 9 When compared to a reusable high-definition Olympus model CYF-VH cystoscope, the single-use cystoscope resolution was marginally higher at 50 mm, comparable at 10 and 30 mm, and lower at 3 and 5 mm. 9
Optical testing revealed that the FOV of the aS4C cystoscope did not meet product specifications (53° less). 6 Similarly, the FOV of the reusable cystoscope was also less than product specifications (12° less), although to a lesser extent. 18 The reusable cystoscope FOV was significantly greater compared to the single-use cystoscope, but its impact on cystoscopy is unclear as there were no significant differences observed during simulated cystoscopy times.
Flexion of the aS4C cystoscope exceeded product specifications in both upward (5° more) and downward deflection (62° more). 6 Similarly, Whelan et al. found that the aS4C cystoscope also exceeded downward deflection specification but marginally did not meet upward deflection (5° less). 9 Our study demonstrated that the single-use cystoscope had significantly greater upward and downward deflection with an empty working channel compared to the reusable cystoscope. Adding instruments to the single-use cystoscope has been reported to decrease downward deflection and flow rates, but not upward deflection. 9 The lighter weight of the single-use cystoscope may offer an advantage, but it was associated with higher forces required for deflection, which could be problematic for surgeons with arthritis or during lengthy procedures. Optical quality remained unchanged after repeated testing, whereas 2 of the 10 single-use cystoscopes demonstrated mechanical wear manifesting as reduced deflection angles and increased deflection force.
One of the greatest appeals of single-use cystoscopes is the perceived reduction in infection risk due to their sterile packaging. While cystoscopy procedures may not be entirely sterile, using single-use cystoscopes eliminates the potential risks associated with inadequate instrument sterilization and cross-contamination. In a recent randomized prospective study, no patients in either the single-use or reusable cystoscope group developed a urinary tract infection. 10 Addressing this gap in knowledge is crucial to further understand the impact of single-use cystoscopes on infection rates.
Regarding environmental impact, Boucheron et al. reported that using reusable cystoscopes resulted in significantly greater waste production and water. Exclusive use of the Ambu single-use cystoscope would result in approximately one ton less waste and almost 95,000 L of water saved per year. 19 Single-use cystoscopes also reportedly have a smaller carbon footprint than reusable cystoscopes, although the carbon footprint was similar when comparing reusable and single-use ureteroscopes. 20,21 The greater environmental impact of reusable cystoscopes may be due to its sterilization methods, harms of reprocessing solutions, and use of packaging and storage materials. On the other hand, discarding single-use cystoscopes could result in a large volume of plastic and electrical devices that require proper disposal. Larger-scale and global studies are needed to assess environmental harms and benefits of both cystoscope types.
The NeoFlex and Coloplast Isiris stent-grasper are two other single-use flexible cystoscopes commercially available. Recent benchtop testing of both cystoscopes demonstrate comparable deflection and optical performance compared to the aS4C cystoscope. 9,22,23 The Isiris, designed for stent removal with a built-in grasper, showed successful outcomes for office-based procedures, except for encrusted and migrated stents. 24 In a benchtop study comparing the NeoFlex to an Olympus CYF-VH reusable flexible cystoscope, the NeoFlex showed greater deflection and lower irrigation rates, similar to our findings with the aS4C cystoscope. 23 However, it demonstrated inferior resolution compared to the high-definition Olympus CYF-VH cystoscope. Notably, the aS4C cystoscope and CYF-VH had comparable resolution. 9
Finally, although cost efficiency was not included as part of our study, it is an important consideration for institutions when selecting an endoscope. Any study attempting to understand cost will, of necessity, require many assumptions. Small changes in these assumptions when compounded can substantially influence cost-effectiveness. Microcosting analyses have reported that reusable cystoscopes are more cost-effective in high-volume endourologic centers, including for procedures such as stent removal. 25,26 Another cost study concluded that disposable cystoscopes are most cost-effective in low-volume centers or in very high-volume centers. 27 The differences in the conclusions of these various cost studies can be attributed to the different cost allocations, including those required for the reprocessing of reusable scopes, repair and maintenance of reusable scopes, personnel and staff responsible for scopes, and the total number of reusable scopes available relative to the procedure volume.
Some limitations of our study include its benchtop design which cannot accurately replicate all aspects of the working environment encountered during clinical cystoscopy. Nonetheless, the single-use aS4C performed comparably to the reusable Olympus CYF-5 Cysto-Nephro Fiberscope in benchtop testing and a simulated bedside cystoscopy. Another limitation is our comparison of a single-use digital cystoscope and a reusable fiberoptic cystoscope, which produced inferior resolution. However, we did not use a reusable digital cystoscope for comparison as a fiberoptic cystoscope is the standard-of-care at our institution and many other sites. Although resolution of a digital cystoscope would be greater than that of a fiberoptic cystoscope, the study by Whelan et al. demonstrated that the aS4C had superior resolution to a standard definition Olympus CYF-V2 digital cystoscope. 9 Another limitation of our study is that it did not employ actual bladder tumors, which may best be evaluated using a prospective randomized clinical trial. Despite these limitations, to our knowledge, this is the first study to assess time efficiency between single-use and reusable cystoscopes in a controlled bedside scenario. Additionally, the study evaluates several previously untested optical and functional parameters such as FOV and force required for deflection.
Given the similar functionality and faster set-up times, disposable cystoscopes represent a promising option for use in the emergency room or when performing after hour procedures. The utility of disposable cystoscopes in the operating room and the clinic will depend on multiple factors not assessed in our study, including staffing availability, case volumes, and institutional policies.
Conclusion
The Ambu® aS4C single-use flexible cystoscope demonstrates comparable benchtop performance with limited user-adjustable optical settings but superior time efficiency compared to a reusable flexible cystoscope. The time efficiency of single-use cystoscopes is important in time-sensitive procedures, such as emergent or bedside cystoscopies. On the other hand, the optical versatility and durability of reusable cystoscopes make them well suited for complex cases, including those in a clinic or operating room settings that are well staffed. Further clinical, economic, and environmental studies should be investigated.
Footnotes
Acknowledgments
Ambu provided the single-use aS4C cystoscopes and the Ambu aView 2 Advance HD monitor system, and Olympus provided a CYF-5 flexible cysto-nephro fiberscope for the benchtop assessment of this study.
Authors' Contributions
R.C.: conceptualization, methodology, formal analysis, investigation, writing—original draft, writing—review and editing, and project administration. C.B.: conceptualization, methodology, investigation, writing—original draft, writing—review and editing, and project administration. A.F.: writing—original draft and writing—review and editing. K.S.: writing—original draft and writing—review and editing. D.R.P., J.C.H., and E.B.: investigation. A.S.A. and J.B.: investigation, resources, writing—original draft, and writing—review and editing. D.D.B.: conceptualization, investigation, resources, writing—original draft, writing—review and editing, and supervision. R.C. and C.B. are recognized as cofirst authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.