
Abstract
Introduction:
Double-J (DJ) ureteral stents are used for multiple purposes in urology. Even though they temporize the subsequent treatment of lithiasis, they may cause different symptoms that impact quality of life (QoL).
Purpose:
In this randomized trial, we assessed whether the diameter of ureteral stents has an impact on catheter-associated symptoms, and their impact on QoL.
Methods:
A total of 194 consecutive patients undergoing DJ insertion between December 2018 and December 2022 were prospectively enrolled and divided into three categories: 4.7F (Group 1, n = 71), 6F (Group 2, n = 65), and 7F (Group 3, n = 58). Within 1 week after the DJ placement, patients completed the validated Spanish version of the Ureteral Stent Symptoms Questionnaire. Continuous variables were compared using analysis of variance and Student's t-tests. For categorical data, the chi-square test was used.
Results:
In the domain of “work” and “additional problems,” there were significant differences. In the “Work” domain, Group 1 presented the lower symptoms. In the domain “additional problems,” patients in Group 1 were prescribed fewer antibiotics owing to low urinary tract symptoms. In question U4 about urinary incontinence, patients in Groups 2 and 3 developed these symptoms more than patients in Group 1. In the “sexual activity” domain, specifically in question S3 (the patient has ever suffered any type of pain during sexual activity?), patients with 4.7F presented lower scores than patients with larger catheters.
Conclusion:
DJ-related symptoms affect QoL in most cases. Smaller catheters produced significantly less urinary incontinence, faster work reincorporation, fewer symptoms related to sexual activity, and fewer catheter-related symptoms than 7F catheters. In contrast, Group 3 presented fewer outpatient visits because of symptoms related to the DJ.
Introduction
Double-pigtail ureteral stents are used for multiple purposes in urology such as relief of urgent obstruction, pre-stenting for retrograde intrarenal operation or ureterorenoscopy (URS), some cases of malignant ureteral obstruction or prophylactic use in pyeloplasty. Even though they are useful for emergency urinary diversion and deferring the treatment of lithiasis in a second stage, they may cause different symptoms such as suprapubic or flank pain, vesicoureteral reflux, hematuria, bladder irritation, urgency, or incontinence, which impact quality of life (QoL). 1 –3
There are a variety of stents with diverse characteristics, such as different designs, lengths, material composition, coating, and dwell time. Stents could be siliconized, drug-eluting stents, stents with a softer distal portion and a harder proximal portion, or with no distal portion. These differences in design have been introduced in attempts to reduce stent-related symptoms, but the standard Double-J (DJ) stent is still the most used.
Some studies have compared multiple symptoms produced by different diameters and catheter compositions without finding concluding results on their impact on QoL. 2,4 Thus, this study aimed to compare catheter-associated symptoms produced by three different silicone DJ diameters and assess their impact on QoL.
Materials and Methods
A total of 412 consecutive patients undergoing ureteral stent insertion after URS or because of lithiasic obstruction between December 2018 and December 2022 were prospectively enrolled and after exclusion criteria, 194 patients were randomized into three categories: Group 1 4.7F: n = 71; Group 2 6F: n = 65; and Group 3 7F: n = 58 Universa Soft (Cook). The DJ catheters were placed under fluoroscopic vision placing the proximal pigtail in the renal pelvis, either as the only intervention or associated with URS.
We excluded patients with associated urinary infection, non-lithiasic disease (retroperitoneal fibrosis and recurrent narrowing), narrowing owing to tumors, pregnancy, bilateral ureteral stents, incomplete questionnaires, or long-term DJ (Fig. 1). The study was approved by the institutional review board and all participants gave their informed consent to participate (IRB No. 2016-002).
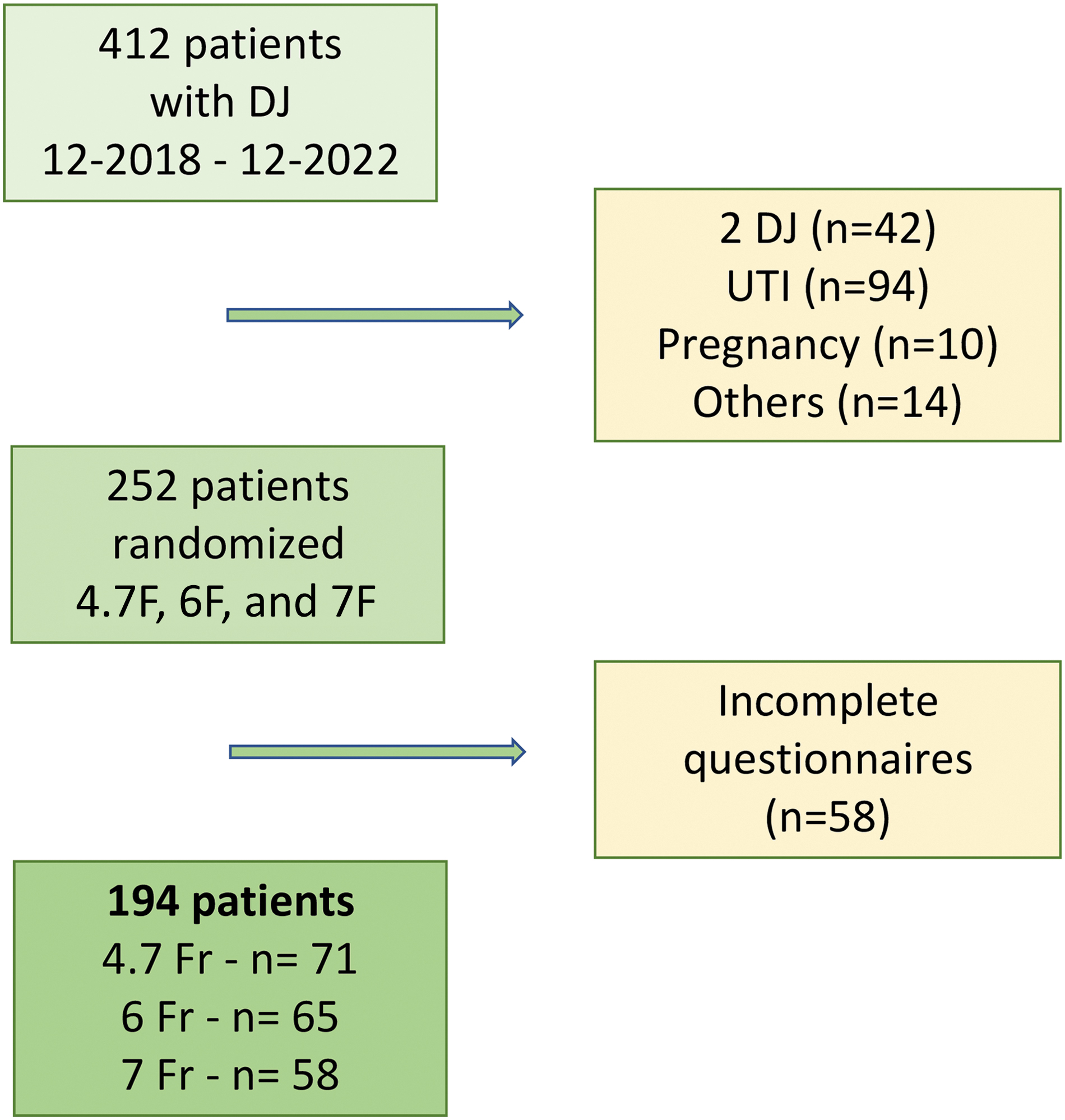
Flowchart of patient's inclusion. DJ = Double-J catheter; UTI = urinary tract infection.
Within 1 week after the DJ placement, patients completed the validated Spanish version of the Ureteral Stent Symptoms Questionnaire (USSQ). 5 This questionnaire consists of 43 questions divided into six domains: 11 about urinary symptoms, 9 about pain, 6 about the general state of health, 7 about work activity, 5 about the sexual sphere, and 5 about additional problems, the last of which is general experience.
Antibiotics were not administered unless patients had a urinary tract infection confirmed by urine culture or pyelonephritis diagnosed by images. Patients were advised to take 150 mg/d of diclofenac in case of pain after discharge. Alpha-blockers and anticholinergics were not systematically administered at discharge.
Statistics
Continuous variables were compared using analysis of variance and Student's t-tests. For categorical data, the chi-square test was used. Analysis was performed using Stata version 14 (College Station, TX, USA). Variables with normal behavior were described as mean and standard deviation (SD), and p < 0.05 was considered significant.
Results
Demographic data and patients' characteristics are shown in Table 1. The mean age was 49.1 (SD 15.4). There was a predominance of male gender 123/194 (63.4%), and the median body mass index was 26.9 (SD 5.3). There was no case of DJ migration. There was no statistically significant difference in height, age, or body mass index between the groups. All patients presented some type of discomfort among the different evaluated domains. In the domains “work” and “additional problems,” a significant difference was evidenced (Table 2). In the domain “Work,” Group 1 presented the lower score (13.75 SD 5.01, p = 0.014). On the other hand, in the “additional problems” domain, the result was lower in Groups 3 and 1 compared to Group 2 (p = 0.033). In contrast, there was no statistical difference between groups in global urinary symptoms, pain, general health, and sexual activity domains.
Demographic Characteristics By Group
BMI = body mass index; DJ = Double-J; SD = standard deviation.
General Domains
Statistically significant.
When analyzing individual questions, in the domain “work,” Group 1 presented a lower score in questions W2 (number of days bed rest) and W3 (number of days reduced more than half daily activity) than the other groups. Group 1 had 1.46 (SD 1.84) days vs 2.26 (SD 2.49) in Group 2 and 1.96 (SD 2.30) in Group 3; and 2.63 (SD 4.52) in Group 1, 4.23 (SD 3.64) in Group 2, and 3.11 (SD 2.97) in Group 3, respectively for W2 and W3 (Table 3), which translates into faster recovery and resumption of daily life in the group of patients with a 4.7F catheter.
Questions
Statistically significant.
Furthermore, in the domain “additional problems,” patients in Group 1 presented a lower prescription of medicine because of low urinary tract symptoms: 1.11 in Group 1 (SD 0.45); 1.33 in Group 2 (SD 0.68), and 1.2 in Group 3 1.2 (SD 0.47) for A2 (p < 0.001) (Table 3). However, in questions A3 and A4 about visits to the emergency room or the need to consult professional help because of symptoms related to the catheter, the patients with larger diameter catheters (Groups 2 and 3) were the ones who went least often compared to Group 1 (Table 3). The majority of patients consulted because of urination disorders, such as dysuria, frequency, and lumbar discomfort when urinating.
Notably, in question U4 about urinary incontinence warned or unaware, patients in Groups 2 and 3 developed these symptoms more than patients in Group 1, p < 0.001 with 1.1 in Group 1 (SD 0.35), 1.32 in Group 2 (SD 0.67), and 1.21 in Group 3 (SD 0.64) (Table 3). In the subgroup analysis according to gender, in question U4, women in Group 1 presented fewer symptoms related to the catheter (Supplementary Table S1).
In question P1, “Have you suffered pain associated with the catheter?”, there was also a significant difference in favor of Group 1 patients (p < 0.001), detailing that presented fewer symptoms related to the catheter in question P1.
In question G4 which asks whether the patient has felt calm, Groups 1 and 2 presented a lower score than Group 3: 2.16 in Group 1 (SD 1.47), 2.17 in Group 2 (SD 1.07), and 2.42 in Group 3 (SD 1.39, p < 0.03), thus Groups 3 presented the lower sensations of calm and tranquility than Groups 2 and 3.
Regarding sexual activity, 54% of responders had no sexual intercourse since the placement of the catheter, and 80% of them were for reasons related to it. In addition, in question S3, which emphasizes whether the patient has ever suffered any type of pain during sexual activity, Group 1 has not had or has had milder symptoms about catheters with a larger diameter; 1.29 in Group 1 (SD 0.55), 1.44 in Group 2 (SD 0.61), and 1.83 in Group 3 (SD 0.87) (p = 0.049).
Discussion
In this study, we found that the DJ diameter had an impact on QoL. This impact was evidenced in the work and additional problem domains of the USSQ. Particularly, Group 1 presented the lower score in the work domain, and Group 3 the lower in the additional problem domain.
In this study, smaller DJ produced less impact on the work domain, and in individual questions “number of days bed rest all day long” (W2) and “number of days reduced more than half daily activity” (W3) faster in patients with a 4.7F catheter than the others with DJ. Similarly, Nestler et al. randomized patients to receive 4.7F, 6F, and 7F stents after URS. 6 They found that patients with 4.7F or 6F stents presented significant advantages in the work domain compared to those with 7F. However, they did not present the result of individual questions of each domain. Conversely, Wu et al. performed a systematic review comparing symptoms between 4.7F, 5F, and 6F DJ after URS with intracorporeal lithotripsy. 7 There was no significant difference in USSQ scores regarding work performance, general health, additional problems, and complications such as fever. This could be owing to heterogeneity among included studies.
In the additional problems domain, Group 2 presented a higher score compared to Groups 1 and 3. However, there was no significant difference between Groups 1 and 3. Regarding individual questions, “visit to the emergency room because of discomfort” (A3) was less for Group 3 than Groups 1 and 2, “admission or procedure because of discomfort” (A4) was worse for Group 1 than Groups 2 and 3, and “use of antibiotics” (A2) was worse for Group 2 compared to Group 1. These results show that there could be unmeasured or hidden factors that influence the result. Other studies found no difference in the additional problem domain between DJ sizes. 4,6 Therefore, these results should be taken with caution.
Regarding individual questions, patients in Group 2 and Group 3 presented more “urinary incontinence” (U4) and “presence or absence of pain” (P1) compared to those in Group 1. In addition, smaller catheters presented better “feeling silent or comfortable” (G4) than Group 3. Wu et al. 7 found that the smaller stents had better outcomes in urinary symptoms and body pain domains evaluated by the USSQ, but they did not analyze individual questions.
DJ stents are essential instruments used daily. The disadvantage of these stents is that most patients experience at least some form of discomfort according to different questionnaires. 3,8,9 In our study, 100% of the patients presented some type of discomfort. This could be owing to this study using the USSQ, a very detailed and specific questionnaire.
Some studies have shown that catheter-related symptoms depend on the correct length. A longer stent causes an overlong intravesical segment, increasing irritative symptoms. 10,11 In our country, there is no easy availability of different catheter lengths; thus, the same length was used in all patients as we use in current daily practice. However, there was no statistical difference when comparing groups by height.
Another small study randomly assigned 45 patients to receive a 4.7F or a 6F DJ after URS. There was no significant difference in the pain score and irritative symptoms between the two groups. 12
Finally, in our study, more than 50% of patients had no sexual activity since DJ placement, which is in line with previous reports. Nestler et al. 6 could not evaluate sexual activity because most patients stopped sexual activity, and Bosio et al. found that 40.4% of patients stopped having sexual activity, most of them because of stent-related problems and or pain during sexual intercourse. 7,9 In addition, in our study, the patients of Group 1 presented fewer symptoms during sexual activity.
This study presents several limitations. We did not collect information on alpha-blockers and anticholinergics, which have been suggested to reduce stent-related problems. 13 This work took 4 years to recruit patients since it included the 2 years of the COVID-19 pandemic era, which delayed interventions and increased the number of stents placed in patients with urinary infections. These also affected the patient's desire to participate in the study and probably impacted questionnaire completeness, which led to the exclusion of many patients.
Another limitation is that, despite randomization, after exclusion, the three groups presented a different number of participants. Also, the role of untreated stones on symptoms was not analyzed. Studies have shown that the shape, material, and length of DJ might affect stent-related discomfort. 14 –20 We used the same length and type of DJ in all the patients. However, there was no statistically significant difference in the height between patient groups.
Conclusion
Ureteral catheter-related symptoms affect QoL in patients either placed post-URS or for obstruction relief. Smaller catheters produced significantly less urge urinary incontinence, faster work reincorporation, fewer symptoms related to sexual activity, and fewer catheter-related symptoms than 7F catheters, but patients with 7F catheters attended emergency centers less often.
Footnotes
Acknowledgment
The abstract was previously published in Abstracts of the 40th World Congress of Endourology: WCE 2023.
Authors' Contributions
S.B.: Data curation and writing—original draft. N.B.: Data curation and conceptualization. L.R. and E.M.P.: Data curation. P.N.C.: Data curation, investigation, methodology, conceptualization, and supervision. L.B.: Data curation, formal analysis, investigation, methodology, writing—original draft, and writing—review and editing. All authors approved the final article in its existing form.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.