
Abstract
Introduction:
Ureteral stents are widely used throughout urologic surgery, most commonly following ureteroscope (URS) procedures. This systematic review aims to assess the current evidence concerning stent on string (SOS) placed after URS and compare it with stents without strings (SWOSs).
Methods:
A systematic review was conducted on several databases using the preferred reporting items for systematic review and meta-analysis (PRISMA) methodology for studies in English language, for patients of all age groups, who had an SOS after URS for stone disease.
Results:
Of 1210 records identified, a total of 22 studies (20 adult and 2 pediatric studies) were included, with a total of 8382 patients. Of these, 3427 (40.9%) had SOSs inserted and 434 (11%) were in the pediatric age group. Our results show that SOS provides several advantages, and compared with SWOS, they were in situ for less time, with no difference in complications such as urinary tract infection or urinary symptoms. Furthermore, significant cost savings, less pain on removal, and high rates of safe home removal were reported in SOS, with >90% patients reporting that they would be happy to remove their SOSs at home. However, a small risk of stent dislodgment must be considered when making decisions regarding SOS placement after URS.
Conclusion:
SOS provides an excellent option after URS, especially in those patients with no intraoperative complication, and their placement is done as a routine insertion based on surgeon preference. These stents reduce dwell time, pain, cost, risks, and suffering involved from prolonged stenting, and majority of patients are happy to remove it themselves at home. Although their use seems to be still restricted in the current endourology practices, they are likely to become the new gold standard for routine URS in future, with more shared decision making and patient-reported outcome measures coming into the mainstream.
Introduction
Ureteral stents are extremely valuable tools in the arsenal of urologic surgery and are of particular value in the context of ureteroscopy (URS) for urolithiasis. First described by Zimskind et al., 1 the design of the “Double-J” ureteral stent was first introduced by Finney. 2 Since then, a number of technological advances have led to the introduction of different designs and materials, aimed at establishing the optimal ureteral stent. 3 Ureteral stents are commonly placed after URS or percutaneous nephrolithotomy (PCNL) for urolithiasis, with stents placed after 63% of ureteral and 80% of renal stone URS procedures. 4
These stents are intended to prevent obstruction, ureteral stricture, and colic and renal failure. But often they are placed after uncomplicated URS because of clinical worry about post-URS edema or fragments blocking the ureter leading to unplanned hospital visits. 5 Although their benefit might be questioned, most stents may only be needed for first 24 to 72 hours. The majority of these stents, however, are placed without strings, we refer to them in this review as stents without strings (SWOSs).
Despite their benefits, there remain significant side effects from ureteral stents, which can include pain, urinary symptoms, urinary tract infection (UTI), and a negative impact on patients' quality of life (QoL). 5 A Cochrane review carried out by Ordonez and colleagues 5 found that there may be a reduction in ureteral stricture and readmission in those patients stented after URS, but that this was low certainty of evidence. There was no clear consensus regarding placement of ureteral stent, and it is often subject to individual clinicians' preference and the specifics of that particular case.
A ureteral “stent on string” (SOS) provides an alternative to standard removal of stents through cystoscopy, as the stent can be simply removed by pulling on the string. First described by Siegel et al., 6 ureteral stents can come packaged with a string attached, their insertion requires little procedural modification to that of SWOS. There is, however, a scarcity of literature regarding SOSs. Concurrently, rates of urolithiasis are increasing in both the adult and pediatric populations, 7,8 leading to an increased burden on health care systems globally.
As a consequence, rates of URS and, therefore, ureteral stenting have also increased. Ureteral stents not only cause significant side effects, but their removal also typically requires a clinic appointment, a clinician, the patient to take time off work, and it requires equipment such as a flexible cystoscope. This systematic review aims to assess the current evidence concerning SOSs placed after URS in the adult and pediatric population to answer our hypothesis, “Is stent on a string (SOS) the new gold standard for post-ureteroscopy ureteric drainage in adult and paediatric patients?”
Methodology
Patient/population, intervention, comparison and outcomes statement
The PICO statement for this systematic review is as follows: in patients subjected to previous URS procedures for urolithiasis, how did patients with SOSs (intervention) compare with those with SWOSs (comparator).
Evidence acquisition: criteria for considering studies for this review
Inclusion criteria
All articles written in the English language
Patients of all age groups who had an SOS after URS
Studies with a minimum of 20 patients
Exclusion criteria
Review articles
Older studies using the same data as a more recent study
Studies with <20 patients
Studies examining treatment for non-nephrolithiasis/urolithiasis conditions or stent for non-URS procedures
A systematic review of the literature was carried out according to the Cochrane review and preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines, including all adult and pediatric studies assessing ureteral stents with extraction strings, after URS. The databases searched were MEDLINE, Google Scholar, CINAHL, EMBASE, The Cochrane Central Register of Controlled trials, and individual urology journals. To ensure all relevant studies were identified, we also manually searched bibliographies of identified studies as well as that of previous systematic reviews. 9 –11 All studies up until July 2023 were included.
Search protocols were tailored to each of the databases, with search terms including “ureteroscopy,” “flexible ureteroscopy,” “URS,” “FURS,” “RIRS,” “renal,” “calculi,” “stone(s),” “urolithiasis,” “laser,” “ureteral,” “ureteric,” “stent(s),” “thread,” “extraction string,” and “string.” To identify pediatric studies, we included the terms “paediatric,” “child,” and “children.”
Boolean operators “AND” and “OR” were used to refine the results. Two reviewers (N.L.H. and C.H.) independently screened the studies to identify relevant studies for inclusion. Any discrepancies or queries were reviewed by the senior reviewer B.K.S. Inclusion criteria were all original studies assessing ureteral stents with extraction strings placed after URS and written in the English language, where the SOSs were removed by pulling on an external string.
Outcomes of interest included author, year of publication, country of study, journal, study type, sample size, mean age, gender of patients, dwell time of stents, stent dislodgments, readmissions or emergency department (ED) visits, UTI rate, urinary symptoms, QoL assessment, cost, pain score on removal of stent, and rate of patient self-removal.
Owing to the heterogeneous nature of the reported data, a narrative review was carried out and a formal meta-analysis was not performed.
Results
Demographics
Of 1210 records identified, a total of 22 studies (20 adult and 2 pediatric studies) were included (Fig. 1). Baseline characteristics of the studies are given in Table 1. Other outcomes of interest, including complications, are given in Table 2.
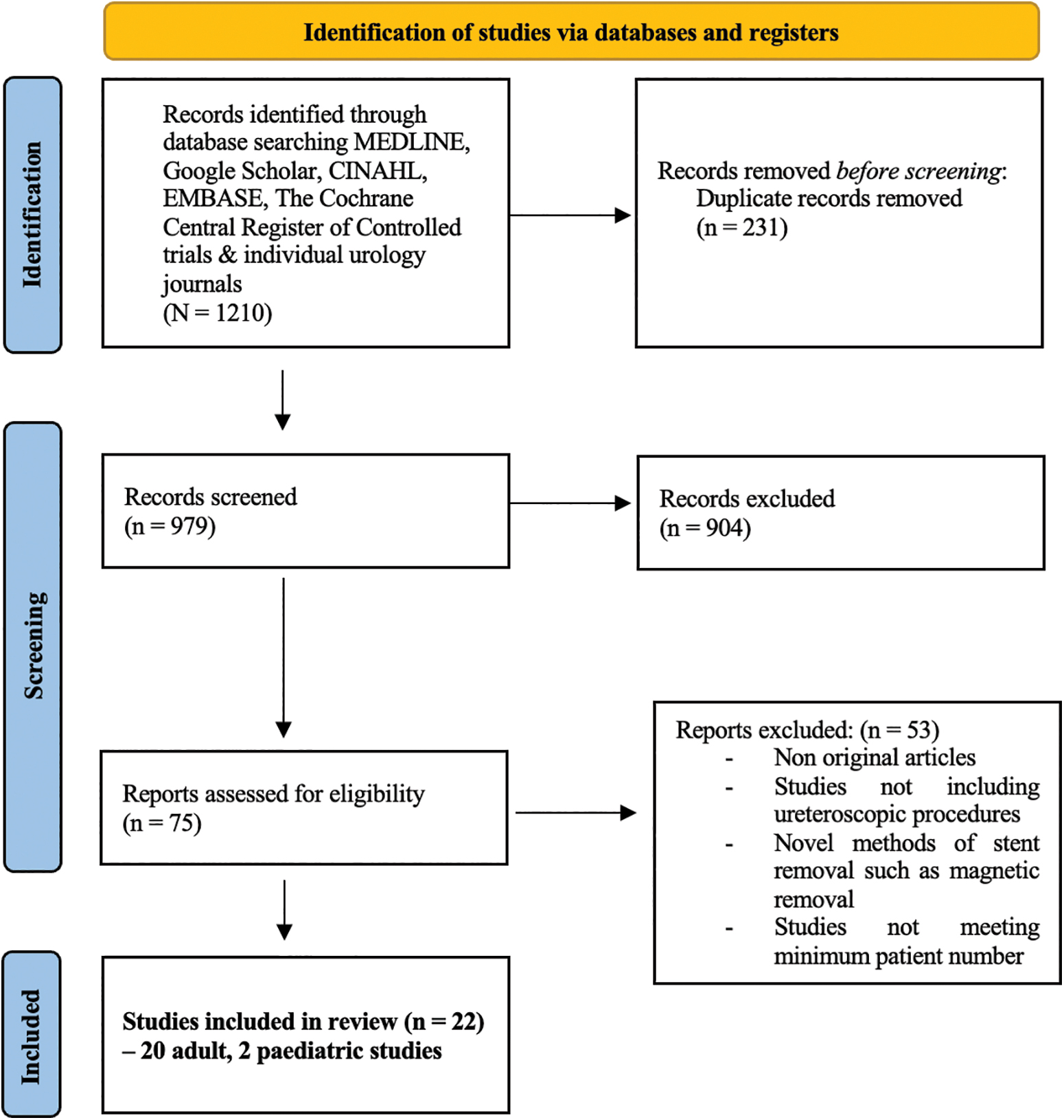
PRISMA flowchart of the included studies. PRISMA = preferred reporting items for systematic review and meta-analysis. Color images are available online.
Demographics of the Included Studies
NR = not recorded; RCT = randomized control trial; SD = standard deviation; SOS = stent on string; SWOSs = stents without strings.
Results of Outcomes of Interest in Included Studies
ED = emergency department; N.B. = Note; QoL = quality of life; URS = ureteroscopy; USSQ = Ureteric Stent Symptom Questionnaire; UTI = urinary tract infection; VAS = visual analogue scale.
A total of 8382 patients were recruited across the studies included, with a total of 3427 (40.9%) SOSs inserted. Of the total patients, 434 (11%) were in pediatric age group. There was a male–female ratio of 1.23:1 in adult patients and 1.44:1 in pediatric patients. In adults, there was an average age of 48.17 years (range: 21–77), in keeping with studies assessing the epidemiology of urolithiasis. 12 In pediatric patients, average age was 4.5 years (range: 4–20). Five of the studies were randomized control trials (RCTs). The remainder of the studies were predominantly retrospective cohort studies or case series. 13
Stent dwell time
Twelve studies reported on stent dwell time. 13 –24 In the 10 studies comparing SOS dwell time with SWOS dwell time, there was a reduced dwell time in the SOS groups for all studies, with 7 of these finding this reduction to be statistically significant. 13,15 –17,19,20,24 The average dwell time in adults was 6.6 days for SOS vs 12.36 days for SWOS, resulting in a dwell time 1.87 times longer in the SWOS groups. In the pediatric studies, only one study compared SOS with SWOS, 25 and the mean stent duration of SOS was 10.1 ± 4.9 days vs 34.0 ± 13.2 days for SWOS (p < 0.01).
Stent dislodgments
Of the studies on adults included, 15 reported on stent dislodgment. 13,14,16 –24,26 –28 Across the studies, the range of stent dislodgment in the SOS groups was between 0% and 15%. The only study reporting dislodgment in the SWOS group was Ghani and colleagues in 2023. 24 In a large retrospective study including 4437 patients, they reported a dislodgment rate of 0.05% in SWOS patients and 0.49% in SOS patients. Interestingly, the RCT by Shah and colleagues 22 shortened the string to between 4 and 5 cm from the tip of the urethra, which may explain the low rates of stent dislodgment (2%).
In their RCT from 2013, Barnes and colleagues 13 reported the highest rates of stent dislodgment at 15%. Of note, none of these patients required reinsertion of their stent. In their discussion, they state that this increase from the 4.7% seen in their retrospective study may be because of the prospective nature of this RCT, leading to a more reporting of dislodgments or the higher percentage of women seen in this study than in the previous study, which they suggest are more prone to stent dislodgment because of female hygiene habits. In the pediatric studies included, 25,29 rates of dislodgment ranged from 0.8% to 7%. In Le et al.'s study, 25 the rate of dislodgment in the SOS and SWOS groups was the same at 7%. This was not found to be statistically significant.
Readmission/ED visits
Twelve studies on adults reported on readmission rates or ED attendance. For SOS patients, this ranged from 0% to 25%. For SWOS patients, it ranged from 0% to 15.8%. 13,16 –19,21 –24,28,30,31 The only study that reported a statistically significant difference between SOS and SWOS was Ghani et al. 24 They reported that ED attendances were significantly higher in SOS patients (12.5% vs 7.9%, p < 0.001) with a stent in situ for up to 4 days than those in patients with an SOS in situ for ≥5 days.
The studies reporting higher rates were by Doersch and colleagues and Hu et al. In Doersch et al.'s study, 30 they reported rates of 17% in the SOS group and 15.8% in the SWOS group, finding no statistically significant difference between the groups. In Hu et al.'s study, 21 where they compared a standard SOS with a novel technique where the length of the string had been shortened (novel group) according to a formula dictated by the length of the patient's urethra, they reported rates of 25% in the standard SOS group and 8.3% in the novel group. They do not suggest why this discrepancy occurred, although there was a higher rate of stent dislodgment and UTI in the standard SOS group. The two included pediatric studies did not report readmission/ED visit rates.
Urinary tract infections
UTI rates were reported in 13 of the studies on adults. 13 –22,24,30,32 For SOS patients, the rates ranged from 0% to 9.1%. In the SWOS patients, the rates ranged from 0% to 13.3%. Fröhlich and colleagues 15 set out to assess whether SOS had a higher rate of UTI than SWOS. They found, in a study totaling 342 patients, the total UTI rate was 6.4%, with no significant difference between the two groups (7.9% [SOS] vs 5.6% [SWOS], p = 0.49). Freifeld and colleagues, 32 however, found a statistically significant increase in UTI in SOS patients than in SWOS patients (6.7% vs 3%, p = 0.057).
Of note, they found that there was a higher UTI rate when SOS was left in situ for longer (20% for >8 days, 3.9% for <8 days, p = 0.001). Lynch and colleagues 19 found higher rates of positive mid-stream urine in SWOS patients than in SOS patients (13.3% vs 1.6%, p = 0.02). Rates of UTI in pediatric patients with SOS ranged from 1.23% to 7%. In the study comparing SOS with SWOS, rates of UTI were 7% in the SOS group and 9% in the SWOS group (p = 1.0). 25
Urinary symptoms and QoL assessment
Five studies on adults reported urinary symptoms. 13,14,16,22,33 Barnes et al., 13 Kim et al., 14 and Shah and colleagues 22 found no significant difference in Ureteric Stent Symptom Questionnaire (USSQ) scores between SOS and SWOS groups. Liu et al. 16 found no significant difference in lower urinary tract symptoms (LUTS) between the two groups. Five studies on adults also reported QoL assessment. Barnes and colleagues, Kim et al., and Shah and colleagues all found no difference in QoL scores from the USSQ.
Inoue et al. 18 used the WHO-5 questionnaire to quantify QoL between SOS and SWOS patients, they found no significant difference between the groups. In the pediatric study by Le and colleagues, 25 pain/bladder spasms/hematuria were seen in two SOS patients (14%) and two SWOS patients (9%), this was not statistically significant.
Cost
Three studies on adults reported on cost savings. 16,19,20 All studies reported cost savings with SOS when compared with studies with SWOS. Liu and colleagues 16 found that cystoscopic removal of ureteral stents costs 507.9 CNY (£55) per case vs 86.7 CNY (£9.44) for SOS. Lynch et al. 19 identified a saving of €390 (£333) per case, which was extrapolated to €23,790 (£20,335) over 7 months. Bates et al. 20 calculated a cost saving of £67,000 in their study, extrapolated to £130,000 per year in one department. Of the two pediatric studies identified, one assessed the cost implications of SOS. Le and colleagues 25 calculated a cost of $400.48 (£310.76) per case using SOS and $2290.86 (£1777.63) per case using SWOS.
Pain score on removal measured by visual analogue scale
Ten studies on adults reported on pain score on removal of stent. 13,14,18,20 –22,28,31,33,34 The average score for SOS was 2.53, and that for SWOS was 4.61. In their RCT, Kim and colleagues 14 reported visual analogue scale (VAS) pain scores of 2.94 for SOS and 4.23 for SWOS (p = 0.005). There was a particularly marked difference in males, when compared with females (p = 0.006). Inoue et al., Bates and colleagues, and Shah et al. 18,20,22 also all reported reduced pain scores on removal in the SOS group, with Bates et al. reporting data that supported the findings from Kim and colleagues that males saw a more marked difference in pain in the SOS group than in the SWOS group.
Patient satisfaction and ability to remove own stent at home
In the six studies on adults assessing the rates of home removal of SOS, 13,26,28,30,31,34 rates ranged from 70% to 100%. In the web-based questionnaire from Loh-Doyle and colleagues, 12% of respondents reported removing their own stents at home, 34 however, there was no indication as to what proportion had been instructed to do this. In Bockholt et al.'s study, 26 all patients except one removed their stent at home. Barnes et al. 13 similarly reported only one male patient who requested removal by clinician because of anxiety. Doersch and colleagues 30 reported two patients were unable to remove their own stents (2%), they do not specify why. Dhar and colleagues reported 100% effective home removal of stents.
High proportions of patients stated that they would be happy to have an SOS again. York and English 31 reported rates of 75%, Loh-Doyle et al. 34 reported rates of 88.2%, and Kim et al. 14 reported rates of 100%.
Discussion
After uncomplicated URS, where complete stone removal is achieved, routine ureteral stenting is not necessary. 35 –38 Ureteral stenting should be reserved for those patients who are at higher risk of complications such as bleeding, sepsis, obstruction, or after ureteral trauma. 35,39 Despite this, ureteral stents are placed after a large proportion of URS procedures, 4 with most urologists choosing to leave stents for 1 to 2 weeks. 35 Published data show that only 19% to 23% of urologists place SOSs after URS, 26,27,34 this might be even lower in the real world.
Stents can commonly stay in situ for longer than the planned 1 to 2 weeks because of waiting times or patient or surgeon factors, which can place patients at risk of UTI, stent encrustation, prolongation of pain, urinary symptoms, 13,40 and rarely “missed” stents. The presence of the coiled “J” of the stent within the trigone bladder leads to significant lower urinary tract symptoms, hematuria, and has a significant effect on patients' QoL. 40
Benefits of SOSs
This review has shown that SOSs have a significantly shorter dwell time than SWOS. 13 –17,19,20,22 This benefit of shorter dwell time should not be underestimated given the significant symptoms that can occur secondary to prolonged ureteral stent placement, which causes patient suffering, loss of work, ED visits, and infectious complications. None of the studies commented on stent encrustation rates, however, we know that encrustation is generally linked to a longer dwell time, which could be avoided with shorter dwell times seen in SOSs. 41 Furthermore, a significant concern with ureteral stent placement is that of the “missed or forgotten stent.” 42
This is clearly more likely to occur in SWOS and can cause significant morbidity to patients, often leading to significant pain, UTI, and necessitating difficult and often lengthy procedures to remove them. Owing to string on the outside, SOS reminds the patients that the stent is still in place, effectively preventing this from occurring. Of course, avoiding stent insertion at all is optimal, however, as we have seen, stent insertion is often performed after URS, and apart from avoiding it altogether, the next best step is to reduce the stent dwell time.
Of the studies included, in general, rates of UTI were similar in the SOS and SWOS groups. Freifeld and colleagues showed that the rates were 20% in those patients wherein SOS was in place for >8 days. In those patients wherein SOSs were in place for <8 days, rates of UTI were comparable with those of the SWOS group. There was no significant difference in UTI in the pediatric studies.
Regarding ED attendances and readmissions, Ghani and colleagues 24 found, in their retrospective study including 4437 patients, that ED attendances were significantly higher in SOS patients (12.5% vs 7.9%, p < 0.001). On subgroup analysis however, they found that this was particularly significant in those patients with a dwell time of 0 to 4 days, compared with those patients with an SOS in situ for ≥5 days.
In the other studies included, there was no significant difference between the groups. One study, by Hu et al., reported rates of 25% in the standard SOS group, but this was not compared with an SWOS group. Data regarding readmission/ED attendance were not collected in the pediatric studies identified. There was no overall difference seen in terms of urinary symptoms or QoL scores.
SWOSs are typically removed through cystoscopy, usually under local anesthesia in the outpatient setting. Cystoscopy involves a clinician, clinic space, and cystoscopic equipment, as well as requiring the patient to attend the appointment. Furthermore, cystoscopy has risks, including UTI, hematuria, and LUTS, which can all impact patients' QoL. 18,43 SOSs allow removal of ureteral stents without the need for cystoscopy, which our review has shown leads to a reduction in pain for patients, which is particularly significant for those patients who have multiple treatments for urolithiasis.
VAS pain scores were significantly lower in the SOS groups than in SWOS groups. 13,14,18,20,22,33,34 For these patients, reducing the pain involved in removing the stent may go some way to alleviating the discomfort associated with a ureteral stent, for the current and any future episodes.
The removal of SOS is either done by patients themselves at home or by the surgeon or nurse in the outpatient setup. If done at home, patients are advised to ensure a complete removal including the pigtail curl at both ends. If unsure of its removal, there might be an arrangement for them to send the picture of the removed stent to the clinical team. As inadvertent stent expulsion can occasionally happen, it is secured to the penis in men and mons pubis or thigh in women usually with a transparent self-adhesive surgical tape. Although the risk is low, patients are also warned that if the stent is accidently dislodged or expelled, they should seek help, to check and ensure the drainage of the kidney, and that a new stent is not needed again.
With regard to pediatric patients, stent removal typically involves a general anesthetic and rigid cystoscopy, which involves risk to the patient as well as needing significant resources. SOSs were first described by Siegel et al. and designed first and foremost for the pediatric patient. In a recent review by Juliebø-Jones and colleagues, 10 they outlined the current plethora of options for ureteral stent removal, including SOSs and magnetic devices. SOSs in pediatric patients offer UTI and LUTS rates similar to SWOSs as well as offering significant cost savings when compared with SWOSs.
By using SOS, rather than SWOS, Bates and colleagues calculated a potential saving of £130,000 a year in one department alone. Le et al. calculated that a single SOS removal in a pediatric patient was $400.48 vs $2290.86 for SWOS. Costs to the patient should also be taken into account, with Staubli et al. 44 finding that 78% of costs from stent insertions in their Swiss study were related to work incapacity.
Removal of SOSs by patients was effective between 70% and 97% of cases in the studies included. 13,26,28,30,31 Doersch and colleagues most recently reported that 89 of 94 (94.7%) patients with SOSs were able to remove it themselves. 30 In an era of spiraling health care costs and concerns over climate change and greenhouse gas emissions, reducing the need for patients to travel to hospital for a cystoscopic removal of their ureteral stents could lead to reduced time off work as well as reduced emissions related to this travel.
Barnes et al. reported that patients avoided a 285 km (177 mile) round trip by removing their stents at home, saving significant fuel and time costs for patients. Furthermore, the majority of patients report being happy to have an SOS again, indicating high rates of patient satisfaction.
Drawbacks of SOSs
The most significant risk associated with SOSs is that of early/accidental dislodgment. In a meta-analysis from 2019, 11 where data from Barnes and colleagues and Kim et al. were studied, they calculated that although dislodgment was more common in the SOS groups compared with SWOS groups, this was not statistically significant. In a recent study by Ghani et al., stent dislodgment rates were 0.49% in SOS patients and 0.05% in SWOS patients (p = 0.013).
Overall, in the studies included in this review, rates of dislodgment ranged between 2% and 15% in the SOS groups, compared with between 0% and 0.05% in SWOS groups. A risk of dislodgment should, therefore, be taken into account when deciding on stent placement after URS, especially in those patients with concerns over ureteral injury or risk of stricture exists. Another potential drawback has been highlighted by Ghani and colleagues, 24 who reported that rates of ED attendances are significantly higher when SOSs are in situ for shorter periods (0–4 days). They recommend a dwell time of at least 5 days. This should be taken into account when planning stent removal.
Future directions
Ureteral stents are an integral part of the armamentarium, with a number of avenues under exploration to find the perfect stent. Recent studies have looked at reducing the amount of stent material, by using complete intraureteral stents, removing the distal pigtail “J” of the stent. Four of these studies required cystoscopic removal 45 –48 and two, included in this study, had externalized stents that could be pulled out by hand. 22,23 These studies showed significant reductions in stent-related symptoms with no significant increase in complications. 49
There are other novel methods for stent removal that obviate the need for cystoscopy including magnetic removal of stent with metal attachment, a “snare” where a lasso type device removes the stent. 42 Another avenue that is being explored in animal models is that of the biodegradable ureteral stent. Promising trials in a rabbit model have shown complete degradation in 4 weeks. 50 Although SOSs seem to be a good option, perhaps the guidelines can do more for guidance regarding the best practice and indications for their use. 38 Similarly, although the use of SOS is mostly in the context of URS, it will also have a growing role in minimally invasive PCNL. 51
Limitations
There are limitations to this review. Although stents are used worldwide for majority of endourology procedures, there are relatively few studies on the use of SOSs. Furthermore, we have limited our studies to only those that included patients undergoing URS. Furthermore, only five RCTs were included and only three of these compared SOS patients with SWOS patients.
We also only identified two pediatric studies for inclusion, making it difficult to draw any significant conclusions with regard SOSs after URS in pediatric patients. Although we move forward to tailored endourologic treatment, we do, however, need more data from RCTs, especially taking into account patient-reported outcome measures and patient preference, which is much more likely to favor SOSs. 52,53
Conclusion
SOSs provide an excellent option after URS, especially in those patients with no intraoperative complication, and their placement is done as a routine insertion based on surgeon preference. These stents reduce dwell time, pain, cost, risks, and suffering involved from prolonged stenting, and majority of patients are happy to remove it themselves at home. Although their use seems to be still restricted in the current endourology practices, they are likely to become the new gold standard in future with more shared decision making and patient-reported outcome measures coming into the mainstream.
Footnotes
Authors' Contributions
N.L.H. contributed to data collection and writing.
C.H. was involved in data collection and editing.
B.K.S. was in charge of editing and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.