
Abstract
Background:
Cone beam computed tomography (CBCT) enables intraoperative cross-sectional and three-dimensional imaging of the urinary tract. CBCT in a hybrid operating room can be used for intraoperative detection of residual stones and potential additional stone extraction at the end of percutaneous nephrolithotomy (PCNL). This study describes our initial experience with intraoperative CBCT during PCNL and analyzes its role in potentially improving its outcomes.
Methods:
We conducted a single-center retrospective cohort study at a tertiary referral hospital between 2018 and 2021. The study aimed to evaluate the outcome of patients who underwent intraoperative noncontrast CBCT scan during PCNL. The CBCT scan was performed when the urologist determined the kidney to be endoscopically stone-free. In case any residual fragments were imaged, an additional effort was made to extract them. Patients were divided into three groups based on treatment outcome: stone-free upon CBCT, not stone-free with additional stone extraction after CBCT, and not stone-free without additional stone extraction. Procedure and patient characteristics were recorded to identify factors associated with additional stone extraction during CBCT-assisted PCNL.
Results:
A total of 102 procedures were included in this study. Intraoperative CBCT scans showed residual calcifications in 58 (57%) cases. In 39 cases, which is 38% of the total population and 61% of the cases with residual calcifications, one or more residual fragments imaged on the intraoperative CBCT-scan were extracted additionally within the same procedure. A higher Guy's Stone Score was associated with a higher likelihood of additionally extracting stones as a result of the CBCT.
Conclusions:
CBCT-assisted PCNL in a hybrid operating room can lead to additional stone extraction in the same procedure in 37% of all cases and in over 60% of the cases in which residual fragments are imaged. The value of CBCT-assisted PCNL appears to increase in the case of more complex stone surgery cases.
Introduction
Percutaneous nephrolithotomy (PCNL) is the recommended surgical procedure for the treatment of large or complex kidney stones. 1 Its primary objective is the complete removal of all stone material since any residual fragments left behind increase the risk of stone disease recurrence, additional stone-related complications, and the need for re-interventions. 2,3 Reported stone-free rates after PCNL range from 56% to 100%, with a decreasing stone-free read in case of a higher stone load or higher complexity of a stone case. 4,5 However, these rates generally rely on ultrasound or Kidney-Ureter-Bladder X-ray for assessment of a stone-free status, which has limited sensitivity in detecting smaller residual fragments as compared to low-dose CT. 6 Moreover, the studies mentioned generally consider patients with residual fragments smaller than 4 mm as stone-free. 4 These findings indicate that a substantial number of patients retain residual fragments following PCNL, potentially leading to further stone-related morbidity.
Intraoperative assessment of a stone-free status can lead to a false assumption of stone clearance in approximately one out of five cases. 7 Hence, there is a need to explore and develop methods that can enhance the accuracy of intraoperative assessment modalities, which, in turn, could contribute to higher stone-free rates.
The standard method for assessment of the stone-free status involves obtaining fluoroscopy images and inspection by means of nephroscopy. A novel imaging modality for intraoperatively imaging the urinary tract is cone beam computed tomography (CBCT).
CBCT can be used in a hybrid operating room to provide high-resolution cross-sectional images of the urinary tract. 8 Recently, CBCT has been introduced in urology and has been used for assessment of a stone-free status or for gaining CBCT-guided percutaneous access to the kidney. 9,10 A recent study from our center demonstrated the feasibility of using the CBCT-scanner for detection of residual stones in PCNL. 11 Several benefits have been suggested for the utilization of CBCT during PCNL. A potential advantage is the possibility of extracting additional stones intraoperatively after performing the CBCT scan, potentially leading to increased stone-free rates. This, in turn, may lead to a decrease in the intensity of follow-up procedures and a reduction in radiation exposure due to a decreased requirement for additional imaging. With enhanced stone-free rates, the decreased need for reintervention could decrease additional stone-related morbidity. Since a stone-free status can be assessed intraoperatively, this can allow for an increase in the use of a totally tubeless exit strategy, thereby reducing postoperative pain and discomfort, along with shortening hospital stay.
With the increasing availability of hybrid operating rooms globally, more urologists now have the opportunity to utilize CBCT intraoperatively. Since CBCT-assisted PCNL is still a relatively new technique with a thin evidence base, patient selection criteria for this purpose have not been defined. Through a retrospective analysis of surgical outcomes along with patient and stone characteristics, we aim to identify predictors associated with additional extraction of stone fragment after a CBCT scan during PCNL.
This could improve the selection criteria for identifying the patients who could benefit the most from PCNL procedures performed in a hybrid operating room.
Materials and Methods
This study is a single-center retrospective cohort study involving patients who underwent CBCT-assisted PCNL between 2018 and 2021. These are the first cases using the CBCT scanner for intraoperatively detecting residual fragments since the installment of our urological hybrid operating room. The CBCT scanner installed in our center is an ArtisQ Ceiling DynaCT (Siemens Healthineers, Erlangen, Germany).
The scanning protocols used had an image acquisition duration of 6 seconds, with a total of 397 frames, a radiation dose of 0.08 to 0.36 μGy per frame, and a slice thickness of 2 mm. The median added surgery duration for performing the CBCT scan was 8 minutes in our feasibility study, and, in the case of imaged residual fragments, an additional median duration of 11 minutes for the effort to attempt to extract these fragments. 11 The mentioned scanning protocols result in an estimated effective dose of 1.96 to 7.76 mSv. 12
All PCNL were performed by a single surgeon (S.R.) with over 10 years of experience. All patients underwent preoperative low-dose noncontrast computed tomography (NCCT) or renal ultrasonography. Patients underwent either PCNL-monotherapy or endoscopically combined intrarenal surgery (ECIRS), in which PCNL is combined with retrograde ureterorenoscopy.
Tract sizes used were ultramini PCNL (OD 13F), mini-PCNL (OD 17.5F), or full-size PCNL (OD 24F). Stones were treated using a combination of pneumatic and ultrasonic fragmentation and laser lithotripsy.
Subjects were included if they were 18 years of age or older and if they underwent a PCNL procedure during which a CBCT-scan was made for potentially extracting any imaged residual fragments at the moment when an endoscopically stone-free status was reached and was stated as such in the surgery report. At the moment of performing the CBCT-scan, the metal nephroscopy sheath was retracted and only a guidewire was left in place. If any residual fragments were visualized on the CBCT-scan, the nephroscopy sheath was reintroduced and an effort was made to retrieve the imaged fragments. In some cases, a retrograde ureterorenoscope was used to attempt to locate residual fragments which could not be located by means of nephroscopy.
The study protocol was reviewed by the local medical ethics review board, which granted a waiver for a comprehensive assessment of this retrospective study.
Patients were divided into three subgroups depending on their operative outcomes; stone-free upon intraoperative CBCT, not-stone free with additional stone extraction, and not-stone free without additional stone extraction.
Several predictors for these abovementioned operative outcomes were evaluated for correlation with their specific outcome. In this way, the patient characteristics that result in a higher chance of a beneficial effect of the CBCT scan were selected. The predictors used were age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA)-class, PCNL Side, Positioning, PCNL Type (PCNL-monotherapy or ECIRS), PCNL tract size (ultramini, mini, or full size PCNL), Stone type (single or multiple stones), mean hounsfield units value of the stone, and the two stone case complexity scores S.T.O.N.E. 13 and Guy's Stone Score. 14 With these predictors, univariate analysis was performed. Mann–Whitney U test was used for ordinal variables, whereas chi-square test was used for categorical variables. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) for Windows (version 23.0). A p-value below 0.05 was considered statistically significant. Statistically significant values are displayed in bold script in the tables.
All patients underwent a regular follow-up NCCT with 2 mm slice thickness 4 weeks after the procedure as is standard care in our center. Follow-up NCCT outcomes were compared to the intraoperative CBCT outcomes. Stone-free data was categorized into Grade A (no stones on CT-scan, absolute stone-free), Grade B (≤2 mm fragments, relative stone-free), Grade C (2.1–4 mm fragments, relative stone-free), or not stone-free.
Results
A total of 102 PCNL procedures, in a total of 100 individual patients, in which a CBCT-scan was performed intraoperatively to potentially detect and extract any residual fragments, were included in this study. Of the 100 included patients, 50% were male, and 50% were female, with a mean age of 55 years. The median BMI was 27.1 kg/m2. In 28 cases, ECIRS was performed, whereas in 74 cases, PCNL monotherapy was performed. Sixty-three cases involved stones on the left side, whereas 39 patients were operated on the right side.
CBCT outcomes
In 64 out of 102 cases (63%), one or more residual fragments were displayed on the intraoperative CBCT scan, whereas 38 (37%) showed no residual fragments.
In 39 (38%) of 102 cases, which is 61% of the cases with residual fragments, additional stone material could successfully be extracted after performing the CBCT scan. Figure 1 shows an example of an intraoperative CBCT scan, in which a residual fragment was imaged at the end of the procedure. The guidewire left in place induces a degree of scatter artifacts but allows for swiftly regaining access to the kidney.
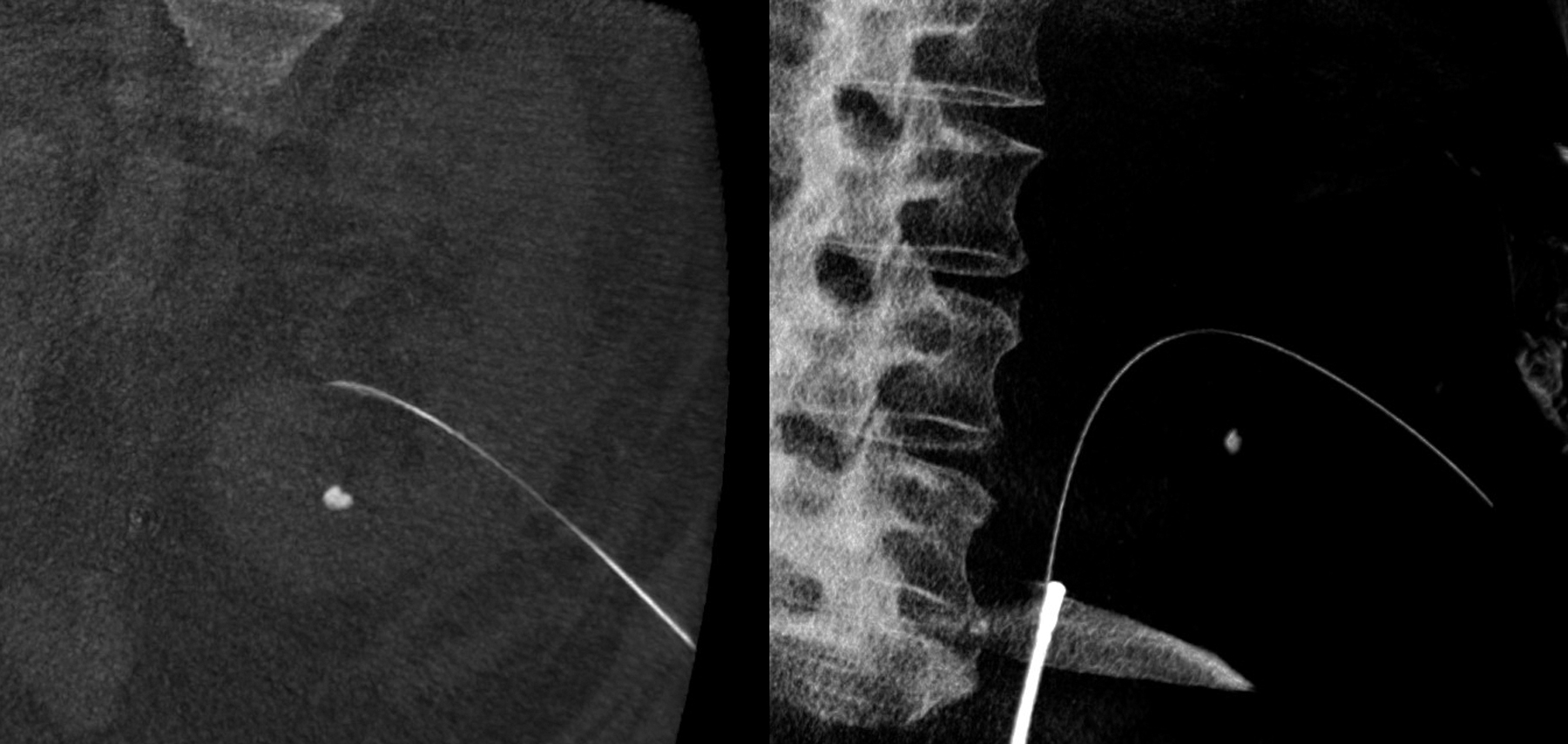
An example of an intraoperative CBCT scan. On the left, a coronal CBCT image is shown, with the guidewire left in place to enable prompt reaccess of the kidney. A residual fragment is imaged on this CBCT image. On the right, the 3D-reconstruction of this same scan is shown with a guidewire, retrograde ureterorenoscope, and residual fragment in place. CBCT, Cone beam computed tomography.
Comparison
In Table 1, a detailed overview of the procedure outcomes and baseline characteristics is listed comparing the group with and without residual fragments on the intraoperative CBCT scan. In Table 2, the group with imaged residual fragments is further divided into a group with (n = 39) and without (n = 25) additional extraction after CBCT. Statistical analyses were performed to indicate factors associated with an increased likelihood of additional stone extraction in case a patient is not yet stone-free at the moment when the CBCT scan is performed. Additional stone extraction in the case of residual fragments upon CBCT was significantly higher (p = 0.015) in the case of a Guy's Stone Score of 3 or 4 (59%) as compared to a Guy's Stone Score of 1 or 2 (28%).
Procedure Outcomes and Baseline Characteristics, Compared Between Stone-Free and Not Stone-Free Study Subjects
Mann–Whitney U test.
Chi-square test.
ASA = American Society of Anesthesiologists; BMI = body mass index; CBCT = cone beam computed tomography; ECIRS = endoscopically combined intrarenal surgery; HU = hounsfield units; PCNL = percutaneous nephrolithotomy.
Comparison Between the Groups With (n = 39) and Without (n = 25) Additional Extraction After Cone Beam Computed Tomography
Mann–Whitney U test.
Chi-square test.
Statistically significant p-values (< 0.05) are highlighted in bold script.
In Table 3, the study population is displayed divided into a group with additional stone extraction (n = 39) versus the group without additional stone extraction (n = 63), along with a statistical analysis testing for significant differences. The group with additional stone extraction had a significantly higher proportion of a Guy's Stone Score of 3 to 4 (p = 0.04).
Comparison Between Cases with Additional Stone Extraction Versus Cases Without Additional Stone Extraction
Mann–Whitney U test.
Chi-square test.
Statistically significant p-values (< 0.05) are highlighted in bold script.
Follow-up outcomes
Upon follow-up NCCT 52 out of 102 cases (51%) were fully stone-free (Grade A), as compared to 38 (37%) upon intraoperative CBCT. Of the remaining 50 cases, 14 (14%) were grade B stone-free, 16 (16%) were grade C stone-free, and 20 (20%) were not stone-free.
In the cases in which additional extraction occurred (n = 39), 18 (46%) resulted in a grade A stone-free status upon follow-up NCCT, 6 were grade B stone-free, 7 were grade C stone-free, and 8 (21%) showed large residual fragments.
No patients that were rendered stone-free intraoperatively showed residual fragments >4 mm in diameter upon follow-up CT. Three patients that were rendered fully stone-free upon CBCT showed residual fragments ≤2 mm upon follow-up NCCT (grade B), and three patients showed residual fragments ≤4 mm upon follow-up NCCT (grade C).
Discussion
In this study, we showed that CBCT scan can lead to additional stone extraction in many cases. In 37% of all included cases, additional stone extraction occurred after performing the CBCT scan. The overall stone-free rate upon follow-up CT increased as compared to the intraoperative CT stone-free rates. To which extent this can be attributed to the additional stone extraction remains unclear.
In case residual fragments were imaged, one or more of these were located and extracted in 61% of cases. This is a relatively high percentage, but this still leaves 39% of cases in which residual fragments were imaged which could not be retrieved. A substantial number of these cases involve those with Randall's plaques or parenchymal stones. In other cases, the procedure had to be ended due to impaired vision, a long procedure duration or anesthesiologic issues. In the remaining cases, intraluminal stones were not extracted even though they were imaged and attempted to be located after performing the CBCT scan. This implies that even though CBCT allows for imaging of potential residual fragments, not all these fragments can effectively be located and extracted.
Only Guy's Stone Score was found as a statistically significant predictor of occurrence of additional extraction after CBCT. For two other predictors regarding stone complexity, S.T.O.N.E. score and stone type, a trend toward significance was observed. Based on these findings, it can be concluded that a greater stone load or increased complexity of a stone case may be associated with a higher likelihood of detecting and extracting residual fragments using CBCT-assisted PCNL. Categorizing stone cases in the urolithiasis research field poses a persistent challenge due to the unique nature of each case. As a result, identifying suitable predictors for additional stone extraction becomes challenging.
In some cases, the follow-up CT-scan showed small residual fragments that were not visualized on the intraoperative CBCT scan. In all these cases, this involved small residual calcifications of 2 mm in diameter or below, located in the operating field. These residual fragments could have been missed due to the scatter imaging artifacts caused by the metal guidewire that is left in place during performance of the CBCT scan to facilitate regaining access to the kidney.
In a recent investigation conducted by Patel et al., which involved 52 prospective CBCT cases, residual fragments were observed in 26 of these cases (50%). 15 Among these 26 cases, further extraction of fragments was performed in 23 instances (88%). These findings partially correspond with the findings of our study, in which residual fragments were present in 64 cases (63%), with additional extraction being carried out in 39 of these cases (61%). The higher degree of additional extraction in their study could be explained by variations in the study populations or differences in procedures for when to perform a CBCT.
Two studies have focused on predicting the stone-free status following PCNL and have investigated factors influencing the disparity between clinical stone clearance and stone clearance on CT imaging, with a discordant evaluation of a stone-free status in 20% and 23%, respectively. 7,16 Especially for these cases, CBCT can be of added value by imaging stone fragments that would otherwise be left in place. Additionally, intraoperative confirmation of a stone-free status by means of CBCT imaging may instill greater confidence in the urologist when considering the implementation of a totally tubeless exit strategy, obviating the necessity for JJ-stent or ureteric catheter placement.
Several limitations can be listed for this study. First, the retrospective nature of this study lowers the level of evidence. The effect of additional extraction cannot be fully assessed with this study due to the interval of 4 weeks between the procedure and the follow-up CT-scan, allowing for spontaneous passage of residual fragments during that time. An alternative would be to perform an intraoperative control CBCT-scan after the extraction of stones, but due to the additional radiation exposure this entails, we chose to refrain from this. The size of the extracted residual fragments was not recorded. Therefore, it is not possible to measure the effect of the additional extraction from this study.
Conclusions
CBCT-assisted PCNL in a hybrid operating room can lead to additional stone extraction in the same procedure in 37% of all cases and in over 60% of the cases in which residual fragments are imaged. The value of the CBCT-scanner seems to increase when the complexity of stone cases or the stone-load increases. CBCT-assisted PCNL seems to be of higher value in cases with a large stone-load in which reaching a fully stone-free status seems achievable in a single procedure. A randomized controlled trial is currently ongoing to determine whether CBCT-assisted PCNL results in a higher stone free rate and ultimately in benefit for patients.
Footnotes
Authors' Contributions
R.A.K.: conceptualization, methodology, investigation, writing; R.M.: investigation; M.T.J.B.: resources, writing; E.A.: resources, writing; I.J.d.J.: supervision, writing; S.R.: supervision, writing, resources, project administration.
Author Disclosure Statement
No competing financial interests exist for this study.
Funding Information
This work was supported internally by the Department of Urology, University Medical Center Groningen, the Netherlands.