
Abstract
Introduction:
Up to 80% of stent patients report urinary discomfort, negatively impacting their daily activities and quality of life. Conventional Double-J ureteral stents (DJSs) can cause adverse kidney and bladder-related symptoms. Complete intraureteral stents (CISs) may reduce bothersome bladder symptoms by reducing foreign material in the bladder. We sought to aggregate and analyze ureteral stent symptom questionnaire (USSQ) data from the available randomized controlled trials comparing CISs with conventional ureteral stents.
Methods:
In February 2023, a Preferred Reporting Items for Systematic Reviews and Meta-Analyses-compliant systematic review was performed to identify studies that evaluated the use of CISs and reported outcomes using the USSQ score. Two authors (D.E.H.-G. and G.S.) independently extracted and analyzed data using Review Manager 5.41. Heterogeneity was assessed using Higgins I2%, with values >50% considered heterogeneous and analyzed with a random effects model; otherwise, a fixed effects model was used. The results are presented as the mean difference (MD) with 95% confidence intervals (CIs). We set our significance level at p = 0.05.
Results:
Six randomized controlled clinical trials compared CISs with DJSs, but only five trials reported the USSQ score. Among these patients, 235 had CISs, whereas the remaining 259 had DJSs or loop-tail stents and served as controls for 494 patients. Urinary symptoms scores were lower in the CIS group (MD −5.19, 95% CI: [−5.89 to −4.50], p < 0.0001). Pain scores were also lower in the CIS group (MD −1.90 [−2.63 to −1.16] p < 0.00001). General health and work performance domains were similar between the groups. A 2.5% stent failure or migration rate requiring endoscopic intervention was reported in the CIS group compared with 0.3% in the DJS group (odds ratio 4.01 [0.96–16.76] p = 0.06).
Conclusions:
CISs significantly decrease urinary symptoms and pain associated with conventional indwelling ureteral stents. However, further trials are needed to determine the optimal patient selection for this type of stent.
Introduction
Urologists commonly utilize ureteral stents to facilitate renal drainage into the bladder in various clinical situations. However, >80% of patients with ureteral stents report symptoms such as bladder or flank pain that significantly impact their quality of life. 1 –3
Symptoms caused by ureteral stents have been theorized to be caused by local irritation from the bladder coil and reflux into the kidney during micturition. 4 These symptoms are typically managed medically with mixed results. 5 Various stent-related factors, such as size, materials, and designs, have been proposed to reduce symptoms. 6 The Ureteral Stent Symptom Questionnaire (USSQ) was introduced and validated by Joshi et al. in 2003 and has since been used in various studies to quantify morbidity from ureteral stents.
Vogt et al. proposed a variation in the classic Double-J ureteral stent (DJS) in which stents are divided, the distal portion of the stent is discarded, and a suture tail is attached to the distal end for later removal. 7 These complete intraureteral stents (CISs) theoretically reduce the amount of material in the bladder and reflux during micturition. We performed a systematic review and meta-analysis to analyze the available literature on CISs and their outcomes compared with conventional DJSs.
Materials and Methods
This systematic review is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting guideline statement. Pubmed®, EMBASE®, Scopus®, and Google Scholar® library databases were queried for full-text articles that addressed the use of CISs. Search terms included “Suture Stent,” “Complete* Intraureteral Stent,” “Single Coil Stent,” and “Stent Symptoms.” Additional articles were identified by reviewing similar and related articles and references from relevant reviews. Articles in English or Spanish without any restrictions on publication date were included. This study is registered with PROSPERO (
Two paired investigators (D.E.H.-G. and G.S.) independently screened 252 articles, focusing on studies reporting symptomatic outcomes related to CISs. Inclusion criteria included prospective nonrandomized studies or randomized controlled clinical trials (RCTs) comparing CISs with conventional DJSs. The studies evaluated ureteral stent-related symptoms and reported outcomes using the USSQ score or a similar scoring system.
The clinical trials had to report the specifications regarding the stent utilized (including its manufacturer, dimensions, and extent of modification), precise techniques employed for stent insertion, duration of stent indwelled, and the utilization of questionnaires for data collection. Studies that did not meet these criteria were excluded. In addition, nonoriginal studies, conference abstracts, and non-RCTs were excluded. Any disagreement about eligibility was resolved by discussion among the two investigators or finally determined by the senior author (W.A.M.) until a consensus was reached. We included studies reporting the impact of CISs vs DJSs on stent-related symptoms.
A total of six studies were identified using the criteria above. CISs were mainly achieved by two methods. First, a regular undersized loop-tail stent with a retrieval string was advanced until its distal end entered the ureteral orifice. The intraureteral placement was confirmed under imaging. The second method was to modify a conventional DJS to a suture stent by cutting the distal end of the stent and placing a suture to its distal tip.
The USSQ score has been previously validated as a tool for assessing various domains of ureteral stent-related symptoms, including urinary symptoms, pain, general health, work performance, and sexual function in different languages. 8 Only studies that consistently reported urinary symptoms, pain, general health, work performance, and sexual function scores were included to ensure adequate analysis. An expanded analysis employing standardized mean differences (SMDs) was employed to draw evidence from studies using alternative scores measuring similar parameters.
Two authors (D.E.H.-G. and G.S.) independently conducted the data extraction process following established methodologies for systematic reviews. To ensure accuracy and reliability, this process was performed in duplicate. The data analysis was carried out using Review Manager 5.41 software. To assess the presence of heterogeneity among the included studies, we employed the Higgins I2% statistic. 9 Studies with I2% values >50% were considered to exhibit significant heterogeneity and were further analyzed using a random effects model. 10
Conversely, a fixed effects model analyzed studies with I2% values ≤50%. When comparing the same outcome measure across studies, we present the analysis results as the mean difference (MD) accompanied by 95% confidence intervals (CIs). The MD provides information about the magnitude and direction of the difference between the intervention and control groups. Our significance level was set at p = 0.05, indicating statistical significance. We utilized an SMD to present the results in cases wherein different outcome measures were compared; this allowed us to quantify and compare the effects across various outcome measures in a standardized manner. 11
An MD or SMD <0 indicates that the intervention group achieved lower scores on the outcome measure tool, namely the international prostate symptom score (IPSS), the overactive bladder symptom score (OABSS), or the USSQ, in comparison with the control group. This finding favors the intervention group, in our case, the CIS group, suggesting that they experienced fewer symptoms or improved outcomes than the control group.
Conversely, an MD or SMD >0 indicates that the intervention group obtained higher scores on the outcome measure tool than the control group. In this scenario, the control group is favored as the lower symptoms group, indicating that they experienced fewer symptoms or better symptomatic outcomes than the intervention group. By examining the direction and magnitude of the MD or SMD, we can gain insights into the relative effectiveness of the intervention and its impact on symptom severity or outcomes compared with the control group.
Two reviewers (D.E.H.-G. and G.S.) conducted separate evaluations of the methodological quality and potential bias of each study included in the analysis. The Cochrane Risk of Bias tool was used. In case of any discrepancies or doubts concerning the quality assessment, both researchers discussed each study to arrive at a final consensus.
Results
Overall
A total of six studies were included in the analysis (Fig. 1). The six conducted studies demonstrated a low risk of bias using the Risk of Bias 2 (RoB 2) tool. Five studies reported outcomes with the USSQ score of 494 patients. Among these patients, 235 had CISs, whereas the remaining 259 had DJSs or loop-tail stents and served as controls. One study did not report outcomes in the USSQ score but instead used the IPSS and OABSS, expanding the total cohort size to 274 CIS patients and 300 controls, resulting in a combined cohort of 574 patients. The summarized findings from all the included studies are given in Table 1.

PRISMA study flow diagram. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Color images are available online.
Summary of Included Studies Inclusion and Exclusion Criteria, Timing, Procedure, Stent Type, and Symptoms Management
DJS = Double-J ureteral stent; NR = not reported; URSL = ureteroscopic lithotripsy.
Urinary symptoms
The urinary symptoms section of the USSQ score was analyzed by including a total of 494 patients from 5 studies. In patients with CISs, the analysis revealed a statistically significant MD of −5.19 points (95% CI: [−5.89 to −4.50], p < 0.0001). An expanded analysis incorporating the IPSS/OABSS cohort and SMD was performed to provide a more comprehensive evaluation, which included an additional 80 patients. The overall SMD was found to be −1.03 (95% CI: [−1.20 to −0.85], p < 0.00001) when utilizing I-PSS scores, and −0.95 (95% CI: [−1.13 to −0.77], p < 0.0001) when using OABSS values. These findings are shown in Figure 2.
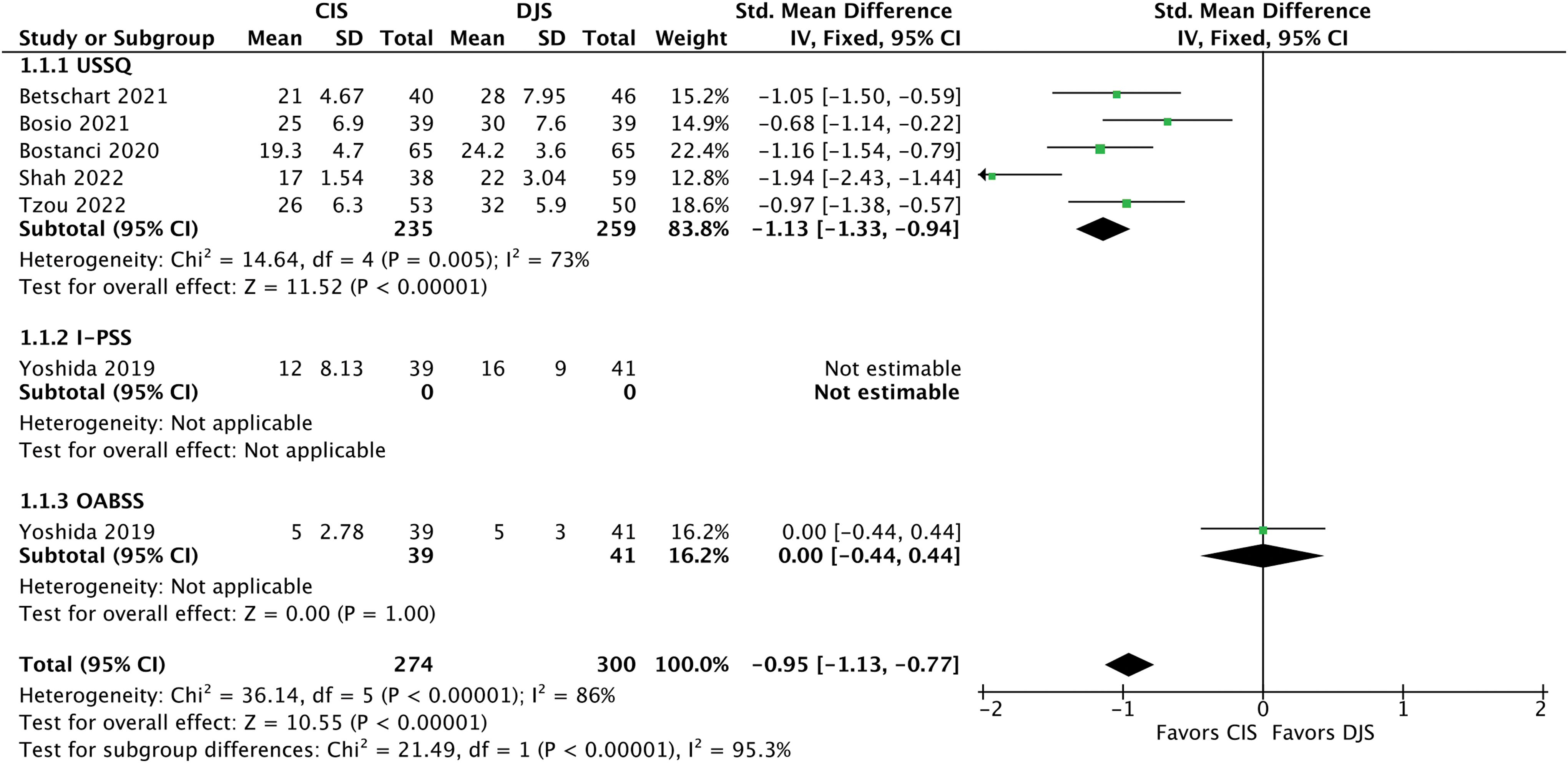
Forest plot summarizing SMD of urinary symptoms. CI = confidence interval; CIS = complete intraureteral stent; DJS = Double-J ureteral stent; I-PSS = international prostate symptom score; OABSS = overactive bladder symptom score; SD = standard deviation; SMD = standardized mean difference; Std = standardized; USSQ = urinary stent symptom questionnaire. Color images are available online.
Pain
A total of six different studies provided data on pain scores. Among these studies, four reported visual analog scale (VAS) scores for pain and USSQ scores; one solely provided VAS scores, and another exclusively presented USSQ data. Analysis of the VAS scores, which included data from 234 patients with CISs and 254 patients with DJSs, revealed a statistically significant MD of −1.90 points ([−2.63 to −1.16], p < 0.00001). Similarly, analysis of the USSQ pain scores involving 131 patients with CISs and 155 patients with DJSs revealed a statistically significant MD of −4.08 points (95% CI: [−5.43 to −2.72], p < 0.0001).
By pooling the data from both pain scores, we conducted a comprehensive analysis and obtained a statistically significant SMD of −0.86 points (95% CI: [−1.18 to −0.55], p < 0.00001). These findings, summarized in Figure 3, demonstrate a significant reduction in pain experienced by patients with CISs compared with those with DJSs.
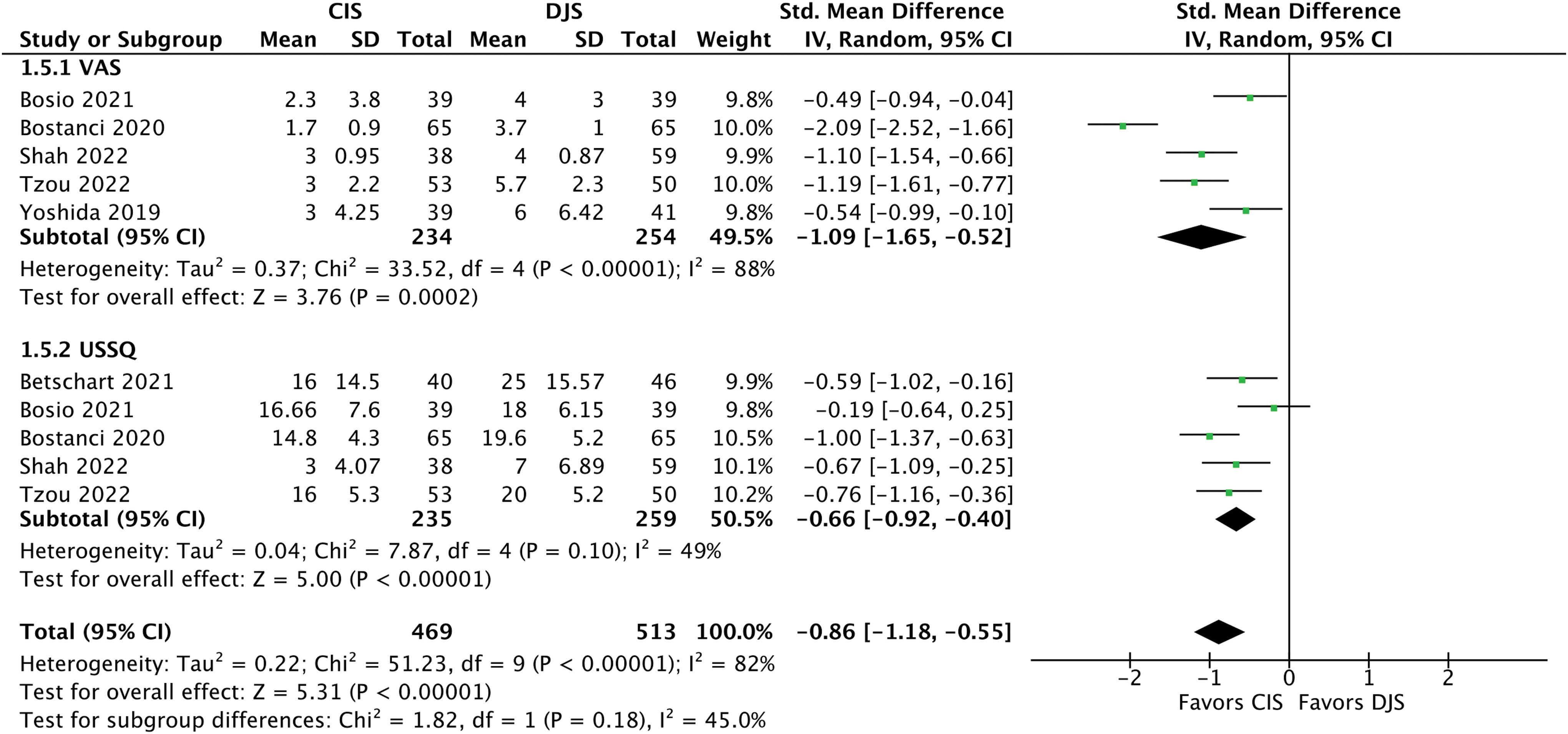
Forest plot summarizing SMD of pain symptoms. VAS = visual analog scale. Color images are available online.
Work performance
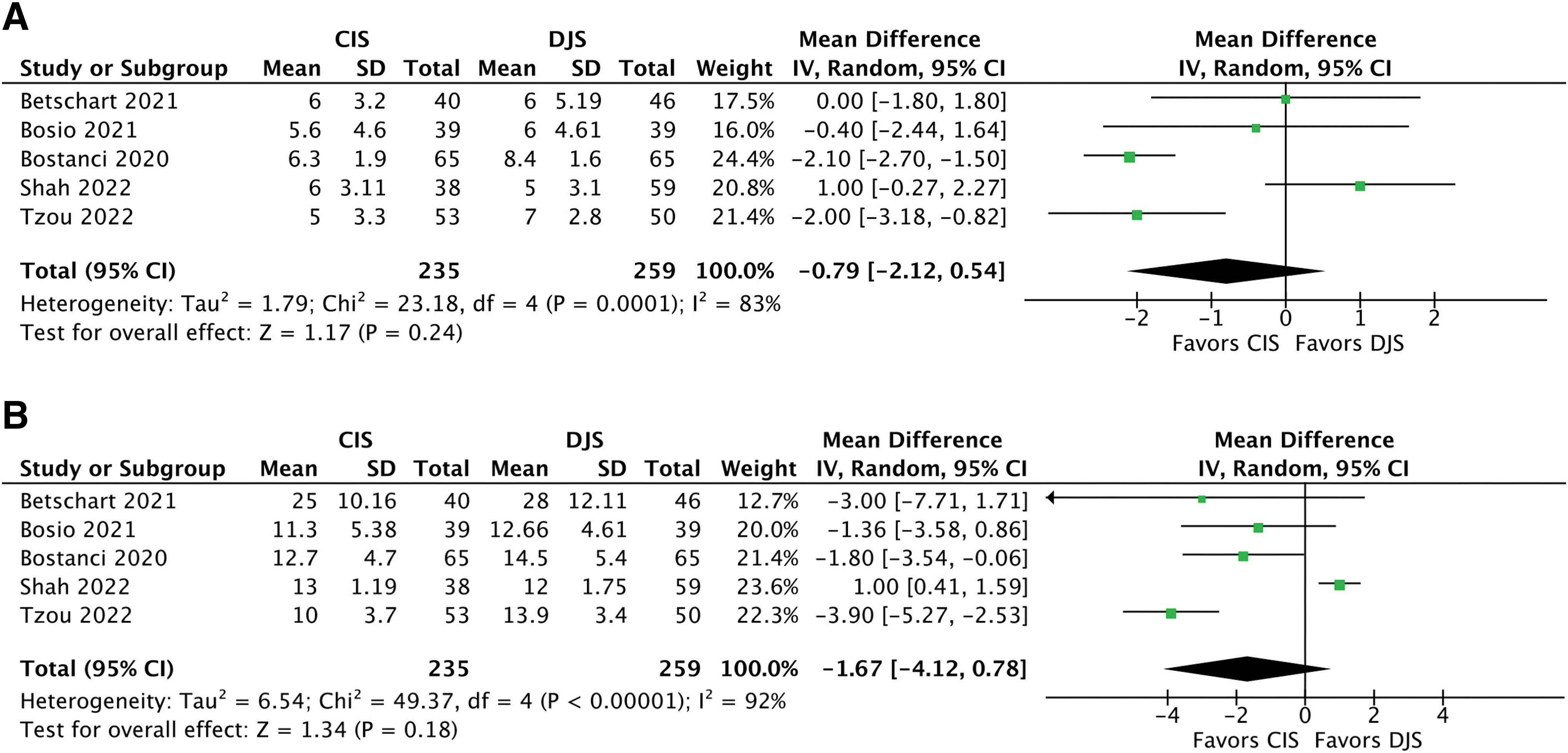
USSQ—work performance was analyzed in five studies, which provided a total patient population of 494 stent users. Meta-analysis of these data revealed a nonsignificant difference in work performance scores, MD −0.79 points ([−2.12 to 0.54], p = 0.24). These findings are displayed in Figure 4A.
Forest plot summarizing
General health
USSQ—general health was analyzed in five studies, which provided a total patient population of 494 stent users. Pooled analysis of these data revealed a nonsignificant difference in general health scores, MD −1.67 points ([−4.12 to 0.78], p = 0.18). These findings are displayed in Figure 4B.
Sexual performance
USSQ—sexual performance was described in four studies, providing a population of 182 patients with CISs and 209 patients with DJSs. Pooled analysis revealed a statistically significant MD of −0.56 points ([−0.92 to −0.21] p = 0.002). These findings are displayed in Figure 5.

Forest plot summarizing sexual performance. Color images are available online.
Stent dysfunction
Stent dysfunction, defined as stent failure, migration, or displacement requiring reintervention, was reported in six trials, with events of interest occurring in only four trials. The pooled incidence of stent dysfunction was 2.5% in the CIS group and 0.3% in the DJS group. Pooled analysis revealed a nonsignificant odds ratio (OR) of 4.01 ([0.96–16.76] p = 0.16). These findings are displayed in Figure 6.

Forest plot summarizing stent dysfunction. Color images are available online.
Sensitivity Analysis
We conducted a subgroup analysis to account for potential confounding factors arising from variations in the types of stents used in the control groups. This analysis involved splitting the studies into groups based on the specific stent used in the control group. The aim was to assess the impact of different stent types on various domains. The results of the subgroup analysis revealed significantly decreased urinary symptom scores, and pain, favoring CIS when compared with both the DJS and loop-tail stent groups. These findings align with the original investigation, providing consistency and robustness to our results.
No significant differences were observed in terms of work performance and general health, consistent with the study's original findings. These findings are summarized in the Supplementary Data S1.
Discussion
This meta-analysis compared the performance of CISs to DJSs using USSQ and similar scores, finding that CISs significantly benefit pain and urinary symptoms. Although the dysfunction rates were not significantly higher in the CIS group, with an OR of 4.01, this variable could become statistically significant if a larger population was studied.
Stent-related symptoms are thought to be caused by local mucosal irritation from the bladder coil and reflux because of poor ureteral coaptation and the possible retrograde flow up ureteral stents. 4 Alternative stent designs have attempted to remedy these factors by decreasing the stent diameter, using softer materials or alternative designs for the bladder coil. However, results have not shown significant advantages. 16,18,19 Thus, treatment of stent-related morbidity has been chiefly through pharmacologic interventions to manage specific patient complaints. 5
Yoshida et al. published the first randomized controlled trial with CISs in 2019, utilizing undersized stents to eliminate the intravesical component. This trial employed various scores to measure the morbidity of stents and found patients who received CISs to have significantly decreased urinary symptoms and pain scores. 15 Yoshida and colleagues was followed by Betschart et al., who achieved similar results by cutting DJSs to approximately half their length and attaching a long suture tail to the distal end, ensuring a complete intraureteral placement.
This trial, similarly, found decreased pain and urinary symptom scores. 12 In addition, Betshcart proposed that the actual length of the stent could be tailored to the length required by each patient. Follow-up studies by Tzou et al. and Shah and colleagues had consistent findings, which are compatible with the aggregate results of this meta-analysis. 13,14
Although dysfunction rates were not statistically significantly different, this is likely a type 2 error related to a relatively low population size compared with the relative event rate. Since a possible fourfold increase in dysfunction rate has been observed, further studies should aim to identify the ideal patient population for CISs. For instance, an obstruction may pose significant challenges in specific people, like patients with solitary kidneys. As an additional factor, CISs only provide ureteral patency in the stented segments, as the suture provides no protective effect.
Thus, patients with obstruction near the ureterovesical junction would be at risk for stent failure with CISs. In cases wherein obstruction may be variable, such as patients passing stones, care must be considered as stones migrating beyond the distal tip of the stent may lead to reobstruction. Whether differences exist in stent performance based on intraureteral length remains to be seen. Interstudy consistency of findings, however, suggests that intraureteral benefits are achieved regardless of length. Thus, one could consider leaving long segments of stents if they do not extend into the bladder.
Additional issues with CISs were identified by Betshcart and colleagues, including in patients wherein stents are used to dilate the ureter before procedures. 12 However, future studies could employ longer stents with shorter suture tails that provide more distal dilation to circumvent this possible limitation.
The most significant limitation of this study is its lack of homogeneity. We include a variety of clinical scenarios with variations in stent design, methodology, and indication for stenting. For example, Tzou et al. left long suture tails that exited the urethra to facilitate manual removal without any adjuvant procedure, unlike any of the other trials. Several studies, such as Yoshida and colleagues, only included patients undergoing endourologic urolithiasis procedures, whereas others had more varied populations. Other potential confounders include nonstandardized pain management regimens in the included studies.
For example, Yoshida et al. and Bostanci and colleagues used oral analgesics to manage stent-related symptoms and, in contrast, Betshcart et al. in addition to oral analgesics used tamsulosin, an alpha blocker, to alleviate symptoms. However, results were consistent across studies, and heterogeneity for pain and urinary symptoms was low, increasing the certainty and confidence of these findings.
Conclusion
Meta-analysis of the literature suggests that CISs may decrease pain and urinary symptoms compared with DJSs. However, further studies are needed to determine the optimal patient selection who would benefit the most from this stent design.
Footnotes
Authors' Contributions
D.E.H.-G. contributed to conceptualization (equal), data curation (equal), formal analysis (equal), investigation (equal), methodology (equal), visualization (lead), and writing—original draft (equal). G.S. was involved in conceptualization (equal), data curation (equal), formal analysis (equal), investigation (equal), methodology (equal), and writing—original draft (equal).
S.K. carried out conceptualization (equal), data curation (equal), formal analysis (equal), investigation (equal), methodology (equal), visualization (supporting), and writing—review and editing (equal). R.E.L. took charge of conceptualization (equal), writing—review and editing (equal), and validation (equal). W.A.M. was in charge of conceptualization (equal), writing—review and editing (equal), and validation (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.