
Abstract
Purpose:
To analyze the utility and outcomes of available endourologic options to treat ureteral stricture after kidney transplantation (KT).
Methods:
A systematic review was carried out for all English language articles from 2000 to 2023 according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) standards using EMBASE, MEDLINE, SCOPUS, Google scholar, and Cochrane library. The search term combination for the string was follows: [(Ureteral stricture) OR (ureter stenosis) OR (ureteral stenosis) OR (Stricture ureter) OR (Narrowing ureter) OR (Ureter restriction) OR (ureteral restriction) OR (ureteral narrowing) OR (ureteral obstruction) OR (ureter obstruction) OR (obstructing ureter) OR (obstructive ureter) OR (narrow ureter) OR (ureteral narrow)] AND [(kidney transplant) OR (transplanted kidney) OR (transplant) OR (transplantation)] AND [(management) OR (Robotic) OR (laser) OR (stent) OR (dilatation) OR (dilation) OR (endoscopic) OR (endourological) OR (Urologic) OR (laparoscopic) OR (surgery) OR (treatment)]. Case reports, review articles, animal and laboratory studies were excluded. Risk of bias assessment was conducted using the RoB 2 and ROBINS-I tools.
Results:
A total of 1102 relevant articles published from 2000 to 2023 were found. After screening of titles and abstracts, a total of 19 articles were included in our systematic review. Ureteral stent/nephrostomy placement, balloon dilatation (ureteroplasty) with or without laser was used as initial approaches whereas follow-up and success rate were analyzed among other parameters.
Conclusions:
The management of ureteral strictures after KT is challenging and selecting the most appropriate treatment is crucial for successful outcomes. Our review suggests that, an endourologic management is a safe option with good long-term outcomes, especially in short and early strictures.
Introduction
Kidney transplantation (KT) is the treatment of choice for patients with end-stage chronic renal failure as it ensures a high survival rate and a better quality of life compared with peritoneal or hemodialysis, even in the elderly people. 1 However, KT operation is not free of complications and ureteral stenosis (US) is a relatively common urologic complication after the operation, which occurs in 2% and 10% of renal transplant recipients. 2 –4 US, which is defined as ureteral luminal narrowing or obstruction owing to the primary scarring or fibrosis of the ureter without external compression, can present in various forms ranging from asymptomatic dilation of the urinary system identified during follow-up to symptoms such as nausea, vomiting, decreased urine output as well as urinary tract infections and increased serum creatinine levels leading to subsequent graft loss. 3 –5 At present, urinary ultrasonography is the initial investigation used to confirm hydronephrosis/hydroureter. 3
US are most commonly located at the distal ureter or the neo ureterovesical (UV) junction 5 ; however, it may not always be easy to find a clear etiology. Some risk factors such as smoking, urinary tract infection, and type of UV anastomosis have been identified, whereas a clear relation with vascular factors was not demonstrated. 6,7 Moreover, donor age, multiple renal arteries, and delayed graft function were described as possible risk factors for late US after KT. 8 On the contrary, it has been shown that US does not negatively affect the graft survival or the overall survival of the patients once timely and appropriately treated. 9
Management options for US includes minimally invasive surgical approaches such as antegrade or retrograde Double-J stent placement, laser or balloon dilatation as well as open surgical reconstruction namely uretero-ureterostomy, uretero-pyelostomy, and re-do extravesical ureteroneocystostomy. Each treatment has its risks, and no true consensus exists as to the optimal treatment strategy to deal with this problem. The gold standard treatment has traditionally been open procedure. However, it is associated with high rates of complications like graft loss and even perioperative mortality rate. 5,10 –12 Furthermore, revision surgeries on transplanted kidneys and ureters are extremely challenging and potentially morbid procedures that require extensive experience and dedicated teamwork. Therefore, urologists tend to treat US using endourologic techniques as much as possible. However, there are dispersed knowledge on the endourologic management of US. This article aims to identify the endourologic procedures used to treat ureteral stricture in post-transplant kidneys, as well as to describe their success rates and complications.
Materials and Methods
Inclusion criteria
All English language articles reporting ≥10 patients of all age groups including pediatric studies.
Studies reporting data of initial presentation and primary treatment for ureteral strictures after transplant.
Exclusion criteria
Case reports, review articles, animal and laboratory studies.
Non-English language studies.
Articles with <10 patients.
Studies reporting on solely open surgical management of US.
Studies reporting treatment of chronic, recurrent, or refractory US.
Studies with insufficient data (i.e., ureteral stricture outcome of treatment was not specified).
Search strategy and study selection
A systematic review was conducted according to Cochrane guidelines and Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist. The databases searched included EMBASE, MEDLINE, SCOPUS, Google Scholar, and Cochrane library. Search was carried out for all English language-relevant abstracts and publications concerning endourologic treatment for ureteral stricture in patients with kidney transplants, from the year 2000 and onward (January 2000 to June 2023).
The precise search term combination for the string was follows: [(Ureteral stricture) OR (ureter stenosis) OR (ureteral stenosis) OR (Stricture ureter) OR (Narrowing ureter) OR (Ureter restriction) OR (ureteral restriction) OR (ureteral narrowing) OR (ureteral obstruction) OR (ureter obstruction) OR (obstructing ureter) OR (obstructive ureter) OR (narrow ureter) OR (ureteral narrow)] AND [(kidney transplant) OR (transplanted kidney) OR (transplant) OR (transplantation)] AND [(management) OR (Robotic) OR (laser) OR (stent) OR (dilatation) OR (dilation) OR (endoscopic) OR (endourological) OR (Urologic) OR (laparoscopic) OR (surgery) OR (treatment)].
The studies found by the search were screened manually according to the title and the abstract content independently and manually by L.C. and A.P. (Amelia Pietropaolo). Followed by the review of the full texts of these eligible studies by the same authors independently, discrepancies were resolved with mutual agreement of the authors (A.T. and M.I.D.).
Data extraction and analysis
Two authors (L.C. and A.P. [Amelia Pietropaolo]) performed the data extraction. Data on journal, authors, publication date, type of study, number of patients, mean age, stricture location, mean time from KT to presentation of US, mean time to management, stricture length, gender, type of management, success rate, total number of transplants, type of donor (living or deceased), definition of success, and conclusions were extracted. Complications were classified according to the Clavien–Dindo system. Data were collected and analyzed on Microsoft Excel 2019 (Microsoft Corp., Redmond, WA). Owing to the heterogeneity of the studies and the absence of any randomized trials or standardized outcomes, the authors decided that a formal meta-analysis was not possible. Risk of bias assessment was conducted by L.C. using the RoB 2 tool in randomized studied and ROBINS-I tool in nonrandomized studies given in Table 1.
Risk of Bias Assessment Using ROBINS-I Tool
 Low risk;
Low risk;  moderate risk;
moderate risk;  high risk
high riskOur search strategy and PRISMA diagram are given in Figure 1.
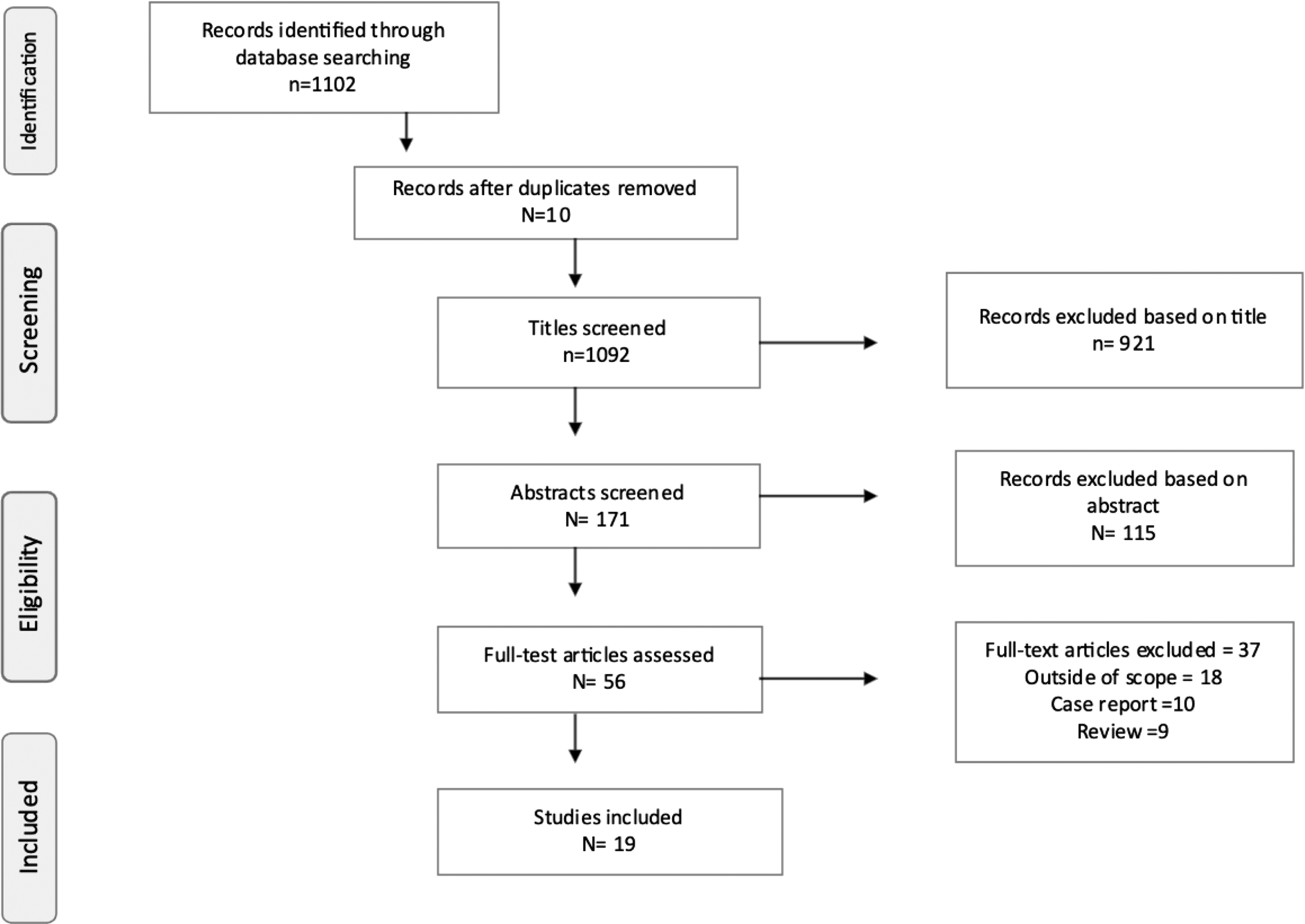
PRISMA flowchart of the included studies. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Results
A total of 1102 relevant articles published from 2000 to 2023 (23 years) were found. After titles and abstracts were screened for eligibility, a total of 19 articles met the inclusion criteria and were included in our final review which are summarized in Table 2. 2,4,5,11 –26 A total of 512 patients who underwent endourologic treatment of US were found. There were nine studies that investigated stent insertion, seven studies regarding balloon dilatation with or without laser incision, and three evaluated combined options. Of the latter, they compared two different groups, one treated with minimally invasive technique and the other with open procedure. Patients' demographics are given in Table 2. There was a total of 273 men with a mean age of the patient cohort at 41.6 years. Stricture was mostly located at the distal ureter close to the UV anastomosis (200 US, 71.4%) and the mean length of the US was 1.94 cm (range: 3.5–9.6 cm). The time to presentation of the US varied between 4 weeks and 48 months (mean time: 19.83 months). Different techniques to resolve hydronephrosis or to treat the US highlighted in the studies are given hereunder.
Overview of the Included Studies (All Studies Are Retrospective)
DJS = Double-J stent; Dx = diagnosis; KT = kidney transplantation; NUS = nephroureteral stent; PNAS = percutaneous nephrostomy with antegrade; PTA = percutaneous transluminal angioplasty; UPJ = ureteropelvic junction; US = ureteral stricture; UVJ = ureterovesical junction.
Ureteral stent or nephrostomy placement
A total of 13 studies identified ureteral stent/nephrostomy placement as the initial approach in US. Of these, five remarked cystoscopic stent insertion while five reported on percutaneous nephrotomy (PCN), four on anterograde stent insertion whereas two did not specify the approach. Of the articles describing stent insertion, six did not proceed to further operative procedures after stenting. On the contrary, the remaining used the ureteral stent as the initial solution and then performed more definitive treatments such as balloon dilatation (7), laser incision (1), or open procedure (ureterostomy, re-do reimplantation) (2).
Balloon dilatation and laser incision or urethroplasty
Balloon dilatation was defined as a good definitive procedure for the treatment of US in some studies. Of these, 1 described balloon dilatation in retrograde (cystoscopy) approach, 11 via antegrade (PCN) approach, and 2 did not specify. Included studies (8) mostly defined the location of US as distal ureter (221, 74%), whereas proximal ureter was most commonly affected in 7 studies (32, 15%), and in 3 studies, mid ureter was labeled as the most frequent location for US (11, 9%). Of note, 4 studies indicated stricture at multiple ureteral locations (13, 11%). In 176/335 (52.5%) patients, the treatment was successful with a resolution of the stenosis and hydronephrosis, consequently. Mean follow-up after treatment of US was 50.1 months and 12 articles reported failure in 150 (47.2%) patients and recurrence of stricture.
Discussion
Nowadays, minimally invasive approach is recommended as the initial treatment modality for ureteral complications after KT, although the preferred treatment options vary among different centers. 5,18 In this study, we tried to highlight the outcomes and nuances in minimally invasive approaches to treat US after KT.
Stent placement
In terms of the retrograde approach, various success rates have been reported from 88% in 97 patients to overall success of 53.8% in 52 patients with retrograde ureteral stenting and 85.2% with retrograde stent exchange procedures. 27,28 In another study from 2006, the authors demonstrated 85% success rate in treating 20 ureteral stenosis with retrograde stent placement. 2 Furthermore, a study from Turkey showed a 75% success with periodic retrograde ureteral stent and balloon dilatation using a retrograde approach. 17
Regarding antegrade ureteral stenting, Bhagat et al. reported a success rate of 57% in 44 patients. 29 Their study confirmed an association between time to obstruction and success rate, with 69% success observed in early obstructions and 33% in late obstructions. Similarly, different authors indicated success rates of 85% and 77.3%, respectively, using percutaneous nephrostomies alone and combined with antegrade stent placement. 15,16 Pappas and colleagues studied 15 ureteral strictures, among which 7 were classified as early and 8 as late. Percutaneous nephrostomies were inserted, and antegrade stent placement was successful in 11 of 13 cases. 16
Researchers from Italy analyzed the outcome of nephrostomy combined with Double-J stent placement, differentiating between antegrade and retrograde approaches. Both approaches demonstrated favorable outcomes with a success rate of 72% in the retrograde approach compared with 50% in the antegrade or combined approach. 5
However, as not highlighted in all studies included, differences in stent type, material, or manufacturer were not analyzed nor taken into consideration in this article.
Balloon dilatation
Several studies have demonstrated balloon dilatation as a good definitive procedure for the treatment of ureteral stenosis. In a study that included 21 patients, results revealed a 62% success rate stating antegrade balloon dilatation is a safe and simple procedure that should be considered as the first-line treatment. 14 In addition, Juaneda et al. looked into 56 patients of whom 51 had US in the distal ureter, and 5 in the proximal ureter with a mean stricture length of 1.5 cm. In all, 45 were treated with PCN and balloon dilatation and 20 of them were successful. 12 Similarly, another study treated 13 patients with periodic retrograde ureteral stent and balloon dilatation achieving a success rate of 75%. 17 Two separate groups studied the outcome of anterograde balloon dilatation and came up with a 47% and 40% success rate, respectively. 11,25
Furthermore, Territo et al. showed a 61% success rate in the treatment of 44 patients with balloon dilatation and or laser incision. 18 In this study, an overall success rate of 52.5% with balloon dilatation only was observed.
Some studies investigated the combination of laser and balloon dilatation. For instance, a study from the United States investigated 12 ureteral strictures, of which 8 were treated with balloon and laser together, and 4 solely with balloon. The success rate was 75% for balloon and laser and 50% for balloon alone. Overall, the authors found a 75% success rate in strictures ≤10 mm and 50% in >10 mm. 22
In another study, two different groups were compared. One group was treated solely with nephroureteral stent (NUS), whereas the other group underwent NUS combined with balloon dilatation (named percutaneous transluminal angioplasty [PTA]). The overall technical success rate was 82%, and after a 6-month follow-up, a success rate of 58% was observed with no significant advantage found in adding PTA to NUS. 24 Others demonstrated no difference between the efficacy of PNAS (balloon dilatation or Amplatz sequential dilatation) and open procedure, comparing 2 groups with 22 patients each. 16
Open procedure vs minimally invasive techniques
Some studies have demonstrated that endourologic techniques are less effective compared with open repair. For example, one study showed a 50% success with percutaneous management in contrast to 71.4% with surgical intervention. Similarly, Arpali et al. conducted a study comparing a minimally invasive approach to open procedure. In their study, there were two different groups, 29 patients in the minimally invasive approach and 16 in the open procedure groups. 19 Overall, US locations were as follows, 10 proximal, 6 mid-third, 21 distal, and 8 multiple locations. The minimal invasive group showed a success rate of only 24.2% expressing that open surgical management should be considered the gold standard approach. 19 In addition, Santos Pérez de la Blanca et al. concluded that endourologic techniques are less effective, whereas surgical repair offers satisfactory results. 25
In a Portuguese single-center study, researchers considered different approaches while treating 15 patients with balloon dilatation, 8 with UV reimplantation, 6 with single catheterization, and 3 with ureterostomy. Although minimally invasive treatment was satisfactory, ureterostomy showed 100% success compared with 47% of balloon and 75% of UV reimplantation. Likewise, researchers from Spain showed their results in a study including 56 US, 11 treated with open procedure and 45 with balloon dilatation. Open procedure had a 100% success compared with the 45% for balloon dilatation. 12
Nevertheless, it is important to note that along with its well-known technical difficulty, the literature indicates that open procedure is associated with higher mortality rates, morbidity rates, and graft loss. One large review conducted by Kashi et al., which compared open procedure to stent placement, revealed 100% graft survival in percutaneous management compared with 87% with open procedure. 30
However, open procedures were not the focus of this study and, therefore, reports dedicated solely to open repair were intentionally excluded as per the scope of the review.
Combination
Several studies have demonstrated that minimally invasive management is not always successful, particularly in cases of late and long ureteral strictures, suggesting a correlation between the length of the stenosis, time of presentation, and the success of endoscopic treatment. Hence, a classification might be helpful to determine whether a patient would benefit from an endourologic approach or open procedure. For instance, in the study conducted by Simsek and colleagues, ureteral obstruction was classified into three subtypes: type 1 as isolated stenosis, type 2 as partial and dense fibrosis along the ureter affecting <50% of the length, and type 3 as a complete stricture. 16 Furthermore, He et al. proposed a clinical classification system based on grades according to the severity and nature (Table 3). 13 Grade 1 US were treated with ureteral stent reinsertions for 6 weeks, grade 2 using balloon dilatation/ureterostomy, and grade 3 with open procedure, ensuing a 100% success rate. 13
Grade Classification According to He et al. 12
DD = deceased donor; LD = living donor.
In addition, other researchers observed a lower success rate after balloon dilatation in late stenosis, which supports the fact that endourologic techniques are more effective in early strictures. 26 Gaya et al. highlighted that anastomosis strictures after radical cystectomy pose a challenge, as endoscopic treatment may not always be feasible owing to low success rates, stricture length, and radiologic morphology. 31 These characteristics should, therefore, be considered when selecting the optimal candidate for endoscopic treatment. Moreover, Gil-Sousa et al. studied 33 ureteral strictures with 10.6 ± 23.0 months mean time from KT to presentation and a mean ureteral stricture length of 2.5 ± 1.9 cm. They treated 15 patients with balloon dilatation, 8 with UV reimplantation, 6 with single ureteral catheterization, and 3 with ureterostomy. Balloon dilatation was successful in 47%, UV reimplantation in 75%, single catheterization in 17%, and ureterostomy in 100%. The authors then concluded that ureteral stricture management should be individualized based on clinical characteristics and the patient's history. 20
Nonetheless, in a relatively recent study, 19 patients who developed ureteral stenosis post-transplant were divided into early (n = 9) and late (n = 10) stricture and the success rates were 100% for early and 90% for late US. 32 Most patients were treated with a nephro-ureterostomy catheter, balloon dilatation, Double-J stent, and nephrostomy. Slight differences were observed in long-term outcomes during follow-up, but similar recurrence rates were noted, indicating that the time of obstruction may not significantly affect the success rate. 10,32 Finally, researchers from Italy revealed their experience on 22 ureteral strictures where they treated their patients with nephrostomies+Double-J stent, comparing the antegrade and retrograde approach showed a 72% success of retrograde and 50% antegrade/combined approach. 5
In our review, the included studies exclusively utilized either the antegrade or retrograde treatment approach for US, and interestingly, we did not observe a significant difference in success rates between the two approaches.
Limitations of the study
Several limitations should be considered for this study. First, detailed individual-level patient data were not available from all studies. Second, there was variability among the studies in terms of grading, surgical technique, location, length of the stricture, time to diagnosis, donor age, antegrade or retrograde approach, type, sex, and surgeon experience. These factors could have influenced the treatment success rates and should be considered when deciding the best treatment option. In addition, some studies included other urologic complications such as urinary leaks, which could have affected the failure rate. Furthermore, it is important to note that data regarding the utilization of antegrade or retrograde approaches as well as robotic approaches are limited. Likewise, the absence of intragroup comparisons among stent types, materials, and sizes may introduce bias into the interpretation of outcomes, underscoring the need for such comparisons in future research.
Overall, the literature supports the use of minimally invasive endourologic techniques as the first-line treatment for ureteral strictures after kidney transplant. However, the success rates vary depending on the specific technique, timing of intervention, and characteristics of the ureteral stricture. Therefore, a classification system for US may be useful to choose the most optimal treatment approach. Further research is needed to cultivate treatment algorithms and improve long-term outcomes in this specific patient population. Finally, the screening process involved only two individuals, which may have introduced the possibility of overlaps or overlooks, potentially leading to the omission of relevant studies or data.
Conclusion
There are a variety of endourologic modalities to treat US after KT. Our review highlighted the efficacy of various endourologic modalities, such as antegrade and retrograde ureteral stenting, balloon dilatation, or combination of these techniques with endourologic modalities such as laser. Although each technique has shown different outcomes, the success rate varies depending on several factors such as the timing of intervention, length and location of the stricture, timing of diagnosis and intervention. Therefore, minimally invasive endourologic techniques can be regarded as safe options with good long-term results. Nevertheless, further prospectively designed research including all necessary parameters is essential to refine treatment algorithms, establish standardized protocols, and address the specific challenges posed by late and long ureteral strictures.
Footnotes
Authors' Contributions
Study concept and design: A.T.
Acquisition of data: L.C., A.M. (Amelia Pietropaolo).
Analysis and interpretation of data: L.C., A.M. (Amelia Pietropaolo), M.I.D., A.T.
Critical revision of the article for important intellectual content: All authors.
Supervision: A.T.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.