
Abstract
Introduction and Objective:
Since its Food and Drug Administration (FDA) approval in 2018, Intuitive Surgical DaVinci single port (SP) robotic platform has been an effectively used technology for multiple urologic procedures. The purpose of this study is to share our early intraoperative and perioperative outcomes and potential benefits for performing a lower anterior access (LAA) incision for SP robot-assisted partial nephrectomy (SP-RAPN). The LAA incision enables performing a trans- or retroperitoneal (RP) approach through the same incision and eases the transition to a RP approach.
Methods:
This study is a prospective review of 78 SP-RAPN cases between March 2021 and January 2023 by an experienced robotic surgeon. A single 2–3 cm oblique incision parallel to the external oblique muscle, one-third of the distance between the iliac crest and umbilicus, was used to insert the multichannel port to perform the RAPN. We extracted intra- and perioperative data of these patients to share the outcomes of this approach.
Results:
SP-RAPN was effectively completed in 78 patients (38 females and 40 males) without conversion to open or laparoscopic techniques. The mean age was 61.2 ± 12.1 years. The mean tumor size was 3.0 ± 1.2 cm, 43 were right-sided masses, and 35 were left sided. The R.E.N.A.L Nephrometry score ranged from (4–11) with an average of 7.0 ± 1.9. Average operating room time was 90.5 ± 24.6 minutes, estimated blood loss was 88.3 ± 134 mL, and length of stay of 1.07 ± 0.7 days. Of the 78 cases, 40 required clamping of the renal artery with average warm ischemia time of 19.4 ± 6.7 minutes in patients who underwent clamping. No complications in all of 78 patients.
Conclusions:
This study demonstrates the feasibility and reproducibility of SP-RAPN using a LAA incision. This incision provides a standardized approach for surgeons to transition to the RP approach using the SP platform.
Introduction
Minimally invasive surgery has been a key focus for urologists seeking innovative approaches to urologic surgeries. Over the past two decades, urologists have made significant advancements in minimally invasive surgery, starting with laparoscopic partial nephrectomy, introduced by Winfield and colleagues in 1993. 1 The introduction of the DaVinci Robot further expanded the possibilities of robot-assisted partial nephrectomy (RAPN) described by Gettman and associates. 2 However, the laparo-endoscopic single-site (LESS) nephrectomy discussed by Fan and coworkers in 2012 had limitations due to instrument crowding and restricted motion, leading to inferior outcomes compared to multi-incision robotic nephrectomy and limiting its widespread adoption. 3 –5
In 2018, the Food and Drug Administration (FDA) approval of the DaVinci single port (SP) Robot brought about a new advancement in minimally invasive kidney surgery. The SP robot addressed many of the challenges associated with LESS by introducing an articulating camera and multielbow instruments. These advancements have made SP robots more widely adopted among urologists.
The SP platform has both advantages and disadvantages. In previous studies, compared with multiport robotic surgery, SP robotic surgery has shown a reduction in the length of hospital stay, pain complaints, opiate use, and estimated blood loss (EBL). 6 –9 However, subcostal incision for retroperitoneal (RP) nephrectomy has been shown to be associated with an increased risk of incisional hernias with subcostal muscle laxity seen on follow-up visits, with an incidence of radiologic-evidence hernia of 8%, as reported by Chow and colleagues. 10
Initial studies examining SP-RAPN have been performed with a transperitoneal (TP) approach with a periumbilical incision and a RP approach using a subcostal incision, like a prior laparoscopic single incision. 5 Harrison and associates reported that SP-RAPN was associated with reduced length of stay (LOS) and opioid use in patients undergoing SP-RAPN vs multiport (MP) RAPN. 11
Initial studies examining SP-RAPN utilized a surgical approach that mimicked the MP approach. At our institution, we hoped to take advantage of the SP robot's unique ability to operate in small spaces. We introduced a new approach that is now referred to by the Single Port Advanced Research Consortium as the lower anterior access (LAA) incision. This incision has been previously referred to as Single Port Ahmed Modification (SPAM), supine anterior retroperitoneal access (SARA), and lower anterior retroperitoneal access (LARA). LAA utilizes a lateral lower abdominal incision. Combined with the ability of the SP robot to globally reposition itself in small spaces, the LAA incision allows for a simultaneous TP and RP approach to kidney surgery.
In this article, we report our experience with this novel approach and demonstrate its feasibility and reproducibility.
Methods
This study is a prospective review of 78 SP-RAPN cases performed between March 2021 and January 2023 by an experienced high-volume robotic surgeon at a single institution. A total of 115 RAPN were performed during the period of this study of which 78 were SP-RAPN and 37 were MP-RAPN. In the same period of the study, this surgeon has performed over 600 SP procedures, including partial nephrectomy, radical nephrectomy, radical prostatectomy, simple prostatectomy, radical cystectomy, and genitourinary reconstruction. All data were collected under Institutional Review Board (IRB) approval, and patients provided consent for robot-assisted partial nephrectomy using the Intuitive Surgical DaVinci SP robotic platform for image-proven renal masses. The study extracted intra- and perioperative data, including patient demographics, tumor characteristics, operative time, EBL, warm ischemia time (WIT), complications, and tumor pathology. Statistical analyses were performed using Microsoft Excel 2022 (Microsoft, Redmond, WA).
Surgical technique
Patients were placed in the lateral decubitus position with the umbilicus over the break of the bed to allow for slight flexion. Pillows and foam padding were used to secure the patient's legs and arms to the bed and protect all pressure points (see figures below). A 3 cm incision was made at the lateral 1/3 of the distance between the ipsilateral iliac crest and umbilicus (Fig. 1). A ruler was not required to find this point. After dissecting Camper's and Scarpa's fascia, the external oblique fascia was scored using electrocautery and muscle splitting. The internal oblique fascia was then opened, and its muscle fibers were split in a similar manner. For TP cases, the transversalis fascia and peritoneum were opened sharply using Metzenbaum scissors to access the peritoneal cavity. For RP cases, the peritoneum was kept intact, and instead, a finger was used to bluntly open the RP space and palpate the psoas muscle posteriorly.

Left image planning of the SPAM incision with umbilicus and ASIS showing. Upper right image is the SP Access Kit with robot docked. Lower right image is SPAM incision after subcuticular skin incision closure. ASIS = anterior superior iliac spine.
Next, the Intuitive wound protector and access port (Intuitive Surgical, Sunnyvale, CA) were placed inside the fascial incision. Pneumoperitoneum was achieved by placing an 8 mm AirSeal® (ConMed Corp, Utica, NY) port through the side trocar of the access port. Pneumoperitoneum was maintained at 10–12 mm Hg.
In the TP approach, the colon was medialized, and in the case of right-sided masses, the duodenum was sharply kocherized. On the right side, the lateral edge of the inferior vena cava (IVC) was traced to the takeoff of the right renal vein, to identify the renal hilum. The fourth arm was used to provide anterior traction on Gerota's fascia to safely dissect the renal hilum for arterial clamping. The fourth arm is generally placed at 12 o'clock which allows effective retraction of the kidney. The LAA approach lines up the fourth arm well with the kidney which eliminates our need for an assistant port to provide retraction.
In RP cases, Gerota's fascia was lifted anteriorly off the psoas muscle. For right-sided masses, the IVC was identified and was followed cephalad to the renal hilum. For left-sided masses, the renal artery was readily identified coming off the aorta, as Gerota's fascia was lifted off the psoas muscle. The ureter could also be identified medially, which is an especially helpful landmark for lower pole masses (Fig. 2).
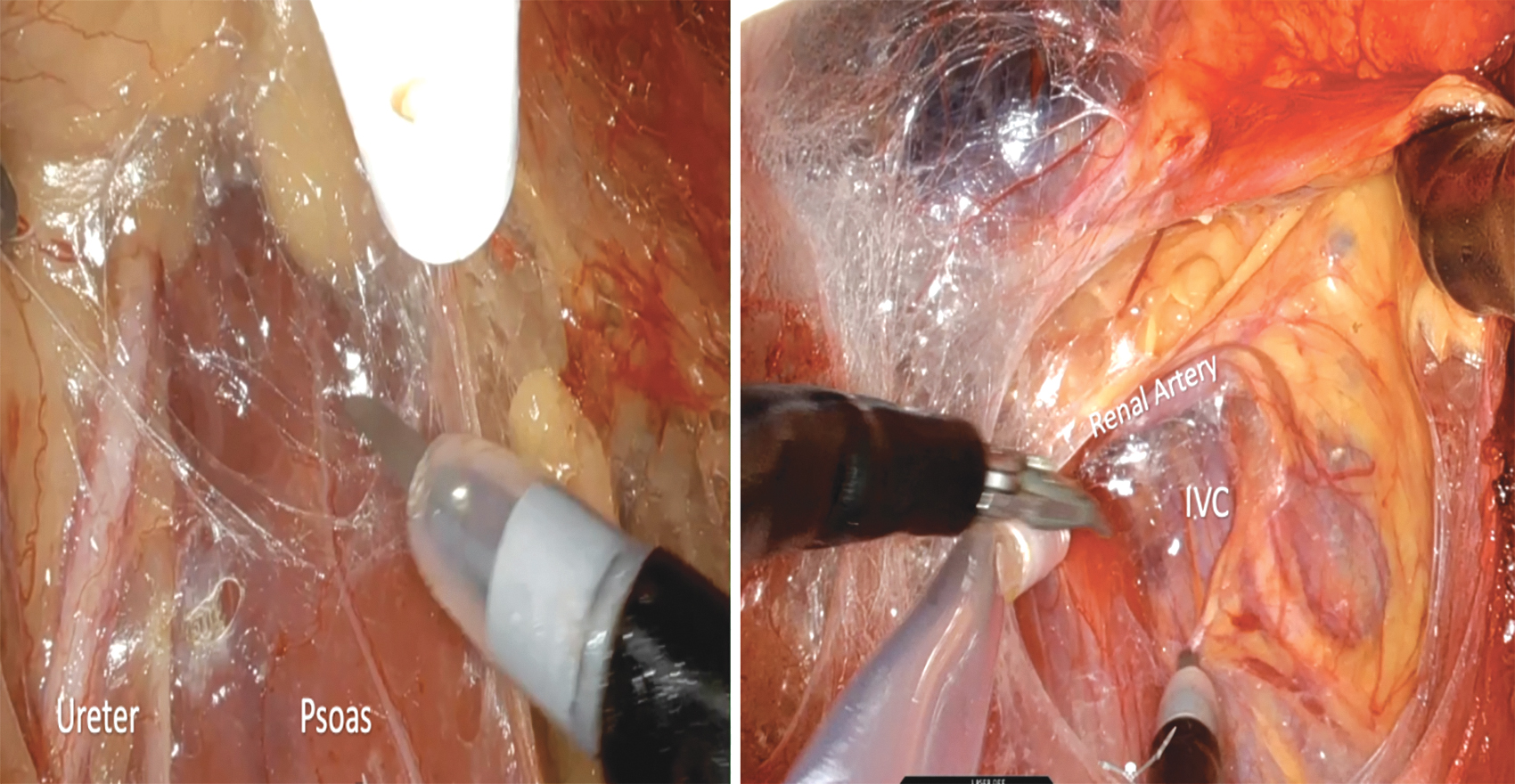
Left image showing ureter and psoas muscle in the initial dissection of a left sided renal mass. Right image showing IVC running parallel to SP robot instruments and renal hilum perpendicular to instruments in a right sided renal mass. IVC = inferior vena cava.
Once the hilum was adequately dissected for arterial clamping, the tumor was identified by opening Gerota's fascia and perinephric fat over the tumor area. Intraoperative ultrasound was used in all cases (BK Medical, Burlington, MA), and the resection site was marked with cautery to ensure an adequate margin. Arterial clamping was performed at the surgeon's discretion using a single bulldog clamp. The tumor was then sharply excised, and a margin was sent intraoperatively to confirm appropriate resection. Renorrhaphy was performed in two layers with a running 3-0 Monocryl for the deep layer and a running 3-0 V-Loc suture for the corticomedullary layer. This technique and approach described is used for all SP-RAPN performed by the surgeon of this study.
Results
SP-RAPN was effectively completed in 78 patients (38 females and 40 males) without conversion to open or laparoscopic techniques. The mean age was 61.2 ± 12.1 years. The mean tumor size was 3.0 ± 1.2 cm, 43 were right-sided masses, and 35 were left sided. One kidney had two renal masses. The R.E.N.A.L Nephrometry score ranged from (4–11) with an average of 7.0 ± 1.9. Average operating room time was 90.5 ± 24.6 minutes, EBL was 88.3 ± 134 mL, and length of stay of 1.07 ± 0.7 days. Of the 78 cases, 40 required clamping of the renal artery with average WIT of 19.4 ± 6.7 minutes in patients who underwent clamping. Of the 78 cases, 22 were performed in a RP manner. No complications were seen in all of 78 patients. Pathology of the removed masses included 42/78 clear cell renal cell carcinomas (RCCs), 13/78 papillary RCCs, 8/78 chromophobe RCCs, 4/78 angiomyolipoma, 10/78 oncocytomas, and 1/78 carcinoids. All patients achieved negative margins. See Tables 1 and 2 for details.
Patient Demographics, Tumor Characteristics, and Surgery Parameters of Single Port Robot-Assisted Partial Nephrectomies
BMI = body mass index.
Pathology of Resected Masses of Single Port Robot-Assisted Partial Nephrectomies
RCC = renal cell carcinoma.
Discussion
In this study, we aimed to establish a new standardized approach to SP-RAPN and demonstrate its feasibility and reproducibility. We believe that the LAA incision provides the greatest flexibility, ease of access, and visualization when performing SP-RAPN. This technique offers unique visualization of the surgical field, allowing for simultaneous access to either a TP or RP approach. Moreover, it aligns the hilum and provides parallel access to the great vessels during clamping, leading to ease in clamping or stapling.
Previous studies have demonstrated several benefits of the RP approach. Stifelman and coworkers compared 296 TP and 74 RP partial nephrectomies and found that the RP approach was associated with a shorter hospital stay, despite a longer WIT. This shorter hospital stay can be attributed to limited colonic mobilization, resulting in reduced postoperative ileus. 12,13 Stifelman and colleagues compared RP to TP partial nephrectomy in multiport cases but this study looks at a combined cohort of TP and RP. A follow-up study with a subanalysis of SP RP vs TP is warranted and would further elucidate the potential benefits of RP partial nephrectomy.
Hughes-Hallett and associates conducted a retrospective cohort study involving 103 patients, 44 of whom underwent MP RP and 59 of whom underwent MP TP. The authors found that RP resulted in shorter operative times (148.5 vs 195.3 minutes, p < 0.01) than TP. The authors concluded that these differences could be due to the RP approach requiring less extensive dissection, resulting in faster access to the renal hilum and avoiding colonic mobilization. 14
A multi-institutional study by Porter and colleagues compared the RP and TP MP approaches to partial nephrectomy. A total of 493 patients (99 RP and 394 TP) were reviewed from a prospective database. In the study, patients who received RP had smaller tumors (2.9 vs 3.4 cm, p = 0.004); therefore, selection bias was reduced by performing stabilized inverse probability of treatment weighting (IPTW) matching. After comparing the two groups using IPTW, the RP group had a lower EBL (100 vs 125 mL, p = 0.007) and shorter hospital stay (LOS) (1.0 vs 3.0 days, p < 0.001) than the TP group. The authors concluded that the RP approach was comparable to the TP approach and should be considered based on the characteristics of the renal mass. 15
At our institution, we are among the first to adopt a SP robotic platform. Initially, the SP approach closely resembled the multiport approach. 11,16,17 However, we observed that using a single flank incision for RP partial nephrectomy led to incisional bulging, likely due to the increased length of the incision compared with multiport procedures and dissection of multiple layers of muscle fibers. A meta-analysis of flank hernias demonstrated an incidence of 17% in the literature. 18 Andreollo and coworkers report in their study that the drawback to a flank incision is the dissection of multiple muscle fibers which ultimately requires a musculoaponeurotic reconstruction during repair. 19 In addition, a flank approach requires an assistant to retract the kidney owing to perpendicular access to the renal hilum. In an effort to overcome these issues, we developed a new incision and approach for SP partial nephrectomy. The incision was made at an oblique angle along the lower ipsilateral abdomen.
This incision approach has several unique advantages. Depending on the location of the mass, we were able to determine which approach (TP vs RP) to take, without having to change the incision location or redock the robot.
A LAA incision was made with the intent of staying in the retroperitoneum. A potential space was created by finger dissection until the lower tip of the kidney was palpated. Once space was created with blunt dissection, we advanced the SP Access Kit and inflated the retroperitoneum. Once the robot was docked, dissection began to identify the psoas muscle without entering the peritoneum. Landmarks to look for are ureters that can be traced as much as the hilum. On the right side, the inferior vena cava can be traced to the right renal vessels. If there were any challenges or difficulties that could not be overcome, we were able to incise the peritoneum and convert it to the less challenging TP approach while also maintaining access to the retroperitoneum if needed.
This approach has increased the use of RP surgery in our practice, allowing us to realize the benefits of RP partial nephrectomy. In situations in which the RP approach is not feasible based on imaging, the SP robot also allows a transmesenteric approach to access the retroperitoneum. This limits colonic mobilization and may also achieve the same benefits of RP partial nephrectomy. A small incision can be made lateral to the colon by advancing a SP to the line of Toldt. The SP robot can be advanced into this space, and the surgery can be performed in a manner similar to a RP approach.
Prior studies and experiences with SP-RAPN using conventional incisions have revealed excellent outcomes. Fang and associates in 2020 reported their experience with 13 SP-RAPN (6 TP and 7 RP) with an average operative time of 176 minutes, EBL of 200 mL, and length of stay of 1.9 days. All partials were off-clamp in this study. 20 Another study by Shukla and coworkers in 2021 performed 12 SP-RAPN (all TP) with an average operative time of 172 minutes, an EBL of 68 mL, and a length of stay of 1.2 days. 21 In our experience with the single port Ahmed modification (SPAM) approach, the average operative time was 90.5 minutes with an average EBL of 88.3 mL and an average length of stay of 1.07 days. These data compare favorably with previously reported literature for SP-RAPN.
In terms of average WIT, our results are comparable to those of other studies. In a prospective cohort study of 146 patients who underwent SP-RAPN, the WIT was 18.29 ± 10.49 minutes. 22 Shukla and associates found that WIT was <25 minutes in all 12 SP-RAPN. 21 Hughes-Hallett and colleagues in their study also found that WIT was about (19.1 minutes). 14 In our study, we found an average WIT of 19.4 minutes. A key advantage of SPAM incision is the parallel nature of the robot to the hilum. The incision lined up the robotic trocar with the hilum, allowing the assistant to easily place the bulldog on the renal artery and allow clamping in a parallel manner. Like the study by Fang and coworkers, our study had a large cohort of off-clamp partial nephrectomies. The surgeon of this study often used an off-clamp approach to partial nephrectomy with the multiport robot. There was not a change in practice patterns or surgical approach when switching from the multiport robot to the SP robot.
In our series, we measured the complexity of the renal mass using the R.E.N.A.L nephrometry score. 23 The mean nephrometry score of the resected masses was 7, range from (4–11). Eleven of the masses had a nephrometry score of ≥10, as calculated by the R.E.N.A.L score. We found that the SPAM approach can be utilized for a variety of renal masses and is not limited to small exophytic tumors with 13 cases in this study being performed on primarily endophytic tumors.
Finally, in our analysis, no perioperative complications were associated with this approach. No hernias were reported with the LAA incision.
Overall, our study establishes a new standardized approach to SP-RAPN using the LAA incision and demonstrates its feasibility, reproducibility, and benefits in terms of operative time, blood loss, length of stay, WIT, and renal mass complexity. This technique provides a valuable addition to the armamentarium for RAPN procedures.
Conclusions
This study demonstrated the feasibility and reproducibility of SP-RAPN using a LAA incision. The LAA incision provides a standardized approach for surgeons to transition to a RP approach using the SP platform.
Footnotes
Authors' Contributions
F.S.—conceived the project, contributed to the design and implementation of research, data collection, analysis of the results, and writing the article. J.N., M.R., B.R., and T.I.—contributed to data collection and analysis. M.B.—conceived project, contributed to the design of research, and helped supervise the project. M.A.—conceived the original and supervised the project.
Author Disclosure Statement
Mutahar Ahmed is consultant at Intuitive, BioTissue, and Ethicon.
Funding Information
No funding was received for this article.