
Abstract
Introduction and Objective:
The COVID-19 pandemic and worldwide quarantine resulted in major changes in individual lifestyles. In New York State, March 16, 2020, marked the end of in-restaurant dining and a reported shift to more cooking at home. We investigated the 24-hour urine of patients with known history of nephrolithiasis to see if changes during COVID-19 pandemic altered the risk of stone disease.
Methods:
Retrospectively, patients with history of nephrolithiasis seen for an outpatient visit from April 1, 2020, to December 31, 2020, were studied. All patients had a 24-hour urine study “pre-COVID” defined as before March 16, 2020, “during-COVID” from March 16, 2020, to December 31, 2020; if available, “post-COVID” from January 1, 2021, to October 31, 2022, was also included. Mean study values were compared using paired, two-tailed t-tests.
Results:
Ninety-three patients (M = 54, F = 39) with a mean age of 60 years were evaluated. Twenty-four-hour urine revealed a significant reduction in urinary sodium (uNa) levels from pre-COVID (166.15 ± 7.51 mEq/L) compared with during-COVID (149.09 ± 7.55 mEq/L) (p = 0.015) and urinary calcium (uCa) levels from pre-COVID (214.18 ± 13.05 mg) compared with during-COVID (191.48 ± 13.03 mg) (p = 0.010). Post-COVID 24-hour urine (N = 73) levels for uNa (138.55 ± 6.83 mEq/L, p = 0.0035) and uCa (185.33 ± 12.61 mg, p = 0.012) remained significantly reduced compared with pre-COVID values, but with no difference compared with during-COVID values. Upon age stratification, this significance was found only in patients younger than 65. There were no significant differences in 24-hour urine total volume, magnesium, or citrate levels.
Conclusions:
During the COVID-19 lockdown, dietary choices limited to home-cooked meals allowed patients to better identify their food choices. This study demonstrates that home-cooked meals improved urinary parameters minimizing lithogenic risk factors for stone formation, including hypernatriuria and hypercalciuria. That these changes persisted into the post-COVID period may indicate improved dietary practices after the lockdown ended.
Introduction
The COVID-19
Several studies have begun to characterize the “Pandemic diet.” 1 –7 One study demonstrated greater consumption of vegetables, legumes, and fruits noted in Brazil, Chile, Colombia, Spain, and Italy during the lockdown, with an increase of weekly consumed servings by ∼8%. 2 Population studies in both Spain and Italy showed an increase in homemade meals and a decrease in delivery food, suggesting a healthier diet with lower sodium intake. 3,4 Consumption of fast foods and instant soups was also noted to be significantly less frequent during the pandemic. 5 There is evidence, thus, to support the notion that the COVID-19 diet is marked by healthier dietary habits than those that had existed before lockdown.
However, there is debate whether the “Pandemic diet” has led to improvement or worsening of dietary habits. According to one study, while the majority of participants believed there was a change to their lifestyle habits, only 16.7% of participants felt an improvement in habits, while 37.2% felt a worsening of their habits. 3 One study in Spain reported an overall increase of 6% of daily food intake, with greater ingestion of energy intake and lower overall nutritional quality of food. 4 Similarly in Poland, one study showed an increase in overall daily food intake, with 11.2% of respondents consuming more than five meals daily. 5
Another study demonstrated an increase in eating and snacking during the lockdown in Poland, most notably in individuals who were overweight and obese. 6 Consumption of salty snacks (i.e., crackers, potato chips, fries) significantly increased in frequency from 26.3% to 31.4%. 5 Given these data, it is unsurprising that one population study in France showed that daily sodium intake increased from 2.9 to 3.2 g/day (p < 0.001). 7
While it is not immediately evident whether dietary habits during the COVID-19 pandemic improved (i.e., less dining out, less fast food) or worsened (i.e., more salty snacks), all these population studies do show that diet did change, for better or worse. Since diet is considered a risk factor of stone disease, these dietary changes due to the pandemic may simultaneously change the risk of stone disease in known stone-forming patients. Diet is often considered to be a contributor of increased risk of hypernatriuria, a known risk factor for nephrolithiasis. Inoyatov and colleagues studied a cohort of 80 patients in a prospective survey of dietary habits, stone analysis, and 24-hour urine studies, and reported that patients who were hypernatriuric had a significantly higher percentage of nonhome-cooked meals per week (p < 0.001) and a higher ratio of meals out per week (p = 0.004). 8
In addition, the American Urological Association (AUA) guidelines include reducing sodium intake in a patient's diet as first-line dietary therapy for calcium stone formers and cystine stone formers. 9
As urine sodium levels are reflective of dietary changes, with increased urine sodium positively correlated with eating out, it is suspected that the “Pandemic diet” should lead to a change in urine sodium levels seen in 24-hour urine collections. 8 To our knowledge, there is no study to date examining the changes in 24-hour urine collection studies before and during the COVID-19 pandemic lockdown in patients with known history of nephrolithiasis. This study aims to examine pre-COVID and during-COVID 24-hour urine samples to determine whether the “Pandemic diet” has an overall lithogenic or lithoprotective effect on patients with a known history of nephrolithiasis.
Methods
A retrospective review was conducted for all patients with a history of nephrolithiasis seen for an outpatient visit either via telehealth or in-office between April 1, 2020, and December 31, 2020. Patients were included in the study if they had a 24-hour urine study both before March 20, 2020, defined in this study as the “start of quarantine,” and between March 20, 2020, and December 31, 2020, defined in this study as the “quarantine” date ranges. Patients were excluded from the study if no urine sample was obtained in those date ranges. Data, including the collection date, total urine volume, urinary sodium (uNa), urinary calcium (uCa), urine magnesium, oxalate, and citrate, were collected from the pre-COVID and during-COVID urine studies, as well as the post-COVID urine study (defined in this study as after December 31, 2020) if available. Stone composition, if available, was collected as well.
Paired two-tailed t-tests were done to compare average pre-COVID and COVID 24-hour urine collection values; ANOVA tests were performed to compared pre-COVID, COVID, and post-COVID 24-hour urine collection values when available. Cohort subanalyses were performed, defined by demographics, including gender, age older or younger than 65, and stone type. Statistical significance was determined by a p-value <0.05. IRB approval was obtained before the initiation of the study. Stony Brook IRB2022-00117.
Results
Ninety-three patients (M = 54, F = 39) with a mean age of 60 years were evaluated. Patients were recurrent stone formers followed with annual 24-hour urine screening. All 93 patients had 24-hour urine screening dates that fell into the pre-COVID and during-COVID date ranges. Seventy-three patients had additional 24-hour urine screening dates that occurred during the post-COVID date range (M = 42, F = 31). Fifty-one patients were younger than the age of 65, and 42 were age 65 and older.
Twenty-four-hour urine screening revealed a significant reduction in the uNa in pre-COVID (uNa mean = 166.15 mEq/L) when compared with during-COVID levels (uNa mean = 149.09 mEq/L) (p = 0.015). Of the 93 patients, 46 patients had decreased uNa levels, 31 had increased uNa levels, and 16 had no change in uNa,. which was defined as a change <15 mEq/L. This difference persisted when comparing pre-COVID uNa with post-COVID levels (uNa mean = 138.55 mEq/L) (p = 0.0035) (Fig. 1A). Of the 46 patients who had decreased uNa levels during COVID, only 1 patient reverted back to the prepandemic uNa levels. There was no significant difference noted in uNa levels when comparing those from during-COVID with ones post-COVID. There was a significant decrease in the uCa levels noted between pre-COVID (uCa mean = 214.18 mg) and during-COVID (uCa mean = 191.48 mg) date ranges (p = 0.010). Of the 93 patients, 48 patients had decreased uCa levels, 11 had increased uCa levels, and 14 had no change in uCa. This difference persisted when comparing pre-COVID uCa with post-COVID levels (uCa mean = 185.33 mg) (p = 0.012) (Fig. 1B). There was no significant difference noted in the uCa levels when comparing 24-urine analysis performed in the COVID date range with that in the post-COVID date range. When stratified by age, there were significant differences in sodium and calcium for patients age <65 (N = 51) from pre-COVID to during-COVID. Specifically in this subanalysis, mean uNa levels decreased from 165.63 to 145.86 mEq/L (p = 0.046). uCa decreased from 244.84 to 208.33 mg (p = 0.00733) (Fig. 1).
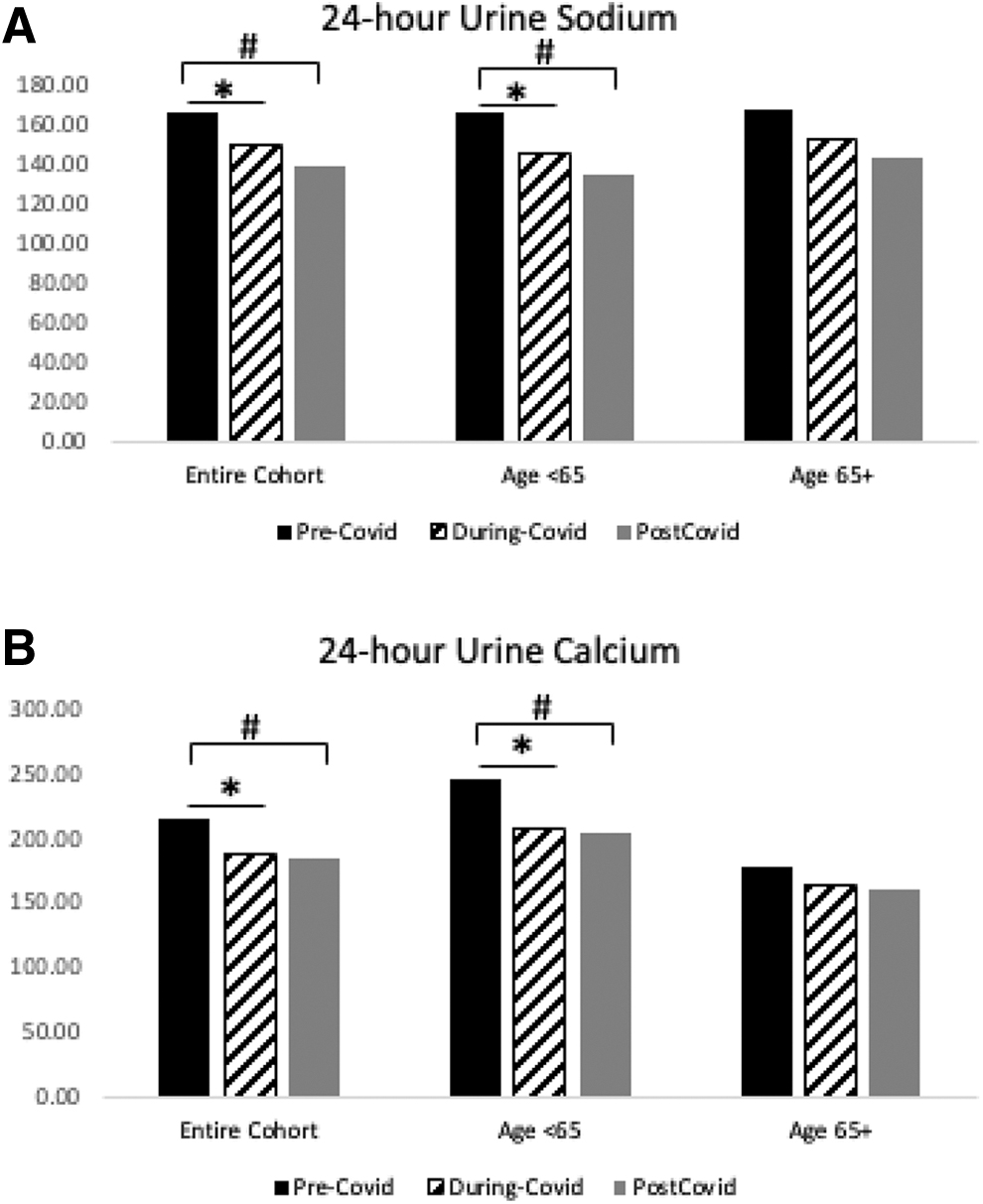
Differences in 24-hour urine parameters pre-COVID, during-COVID, and post-COVID.
These changes from pre-COVID persisted to post-COVID mean uNa 134.55 mEq/L of (p = 0.0011) and mean uCa 205.03 mg (p = 0.011). These changes did not uphold in patients aged >65. Other 24-hour urine parameters, including total volume, magnesium, oxalate, and citrate, revealed no significant differences across the three time periods in all groups. Stone analysis revealed calcium oxalate (61%), calcium phosphate (15%), uric acid (15%), other (9%).
Discussion
This study aimed to assess the impact of the COVID-19 pandemic on the dietary habits of recurrent nephrolithiasis patients, as highlighted through 24-hour urine analysis. Our results suggest that changes made during the COVID period may in fact be lithoprotective through the alteration of urinary sodium and calcium levels. A statistically significant decrease in both urine sodium and urine calcium was seen in these patients when comparing pre-COVID levels with during-COVID levels. While population studies on diet and dietary sodium varied between studies, it is certainly possible that both salty snack consumption and home cooking increased, but a net decrease in sodium intake ultimately occurred.
Regardless of the overall specifics of the “Pandemic-diet,” the results of this study suggest that the Pandemic-diet is lithoprotective. This is most likely due to decreased sodium intake, possibly due to an increase in home-cooked meals in the face of widespread lockdowns, a trend seen in other populations. 3,4 It was also noted that patients younger than 65 had a greater contribution to the changes noted compared with those older than 65. Younger patients appeared to feel a greater effect of the pandemic on their dietary habits than older patients who may have more rigid dietary habits.
Post-COVID date ranges occurred during a time where many community restrictions were lifted, resulting in the reopening of restaurants and a slow return to life seen before the start of the pandemic. Of note, urinary sodium changes observed in the during-COVID period persisted through this time frame. While this may be a feature of ongoing fear of dining in restaurants given the continuation of the pandemic, it is also possible that any dietary improvements persisted due to patient choice.
Calcium stones are the most common stones comprising 80% of stones in the literature, which is in congruence with the 76% calcium stones in our study (61% calcium oxalate, 15% calcium phosphate). 10 Hypernatriuria is a well-known risk factor for nephrolithiasis, with sodium intake playing a major role in calcium stone occurrence. The link between sodium intake and urinary calcium excretion has been observed in many studies, showing that low-sodium diets can reduce calcium excretion in hypercalcuric stone formers. 11 It is for this reason that lowering dietary sodium intake is often a first-line recommendation in stone formers, with the AUA recommending clinicians counsel patients with calcium stones to limit sodium intake. 9 This is reflected in this study with significant decreases in urinary calcium from pre-COVID to during-COVID time periods and even into the post-COVID period.
It is important to note that while other 24-hour urine values were studied in the analysis, including total volume, magnesium, oxalate, and citrate, these values remained largely unchanged. In addition, when stratified by stone type, no differences were found, suggesting that the main drivers behind any protective effect from this diet are mainly a result of dietary sodium changes.
This study is an important start in assessing the trends of 24-hour urine analyses as affected by the COVID-19 pandemic in recurrent nephrolithiasis patients, but there are limitations. The major limitation of this study is not knowing the dietary practices of the patients included in the analysis. Another major limitation is the inability to determine if these patients were having to change their dietary intake due to COVID regulations or if it was the result of dietary counseling for stone prevention or medication changes. With additional information obtained by patient food diaries and/or subjective questionnaires, the elucidation of the reasons behind the 24-hour urine study changes observed may become clearer.
Conclusions
A decrease in lithogenic risk factors occurred during the COVID-19 pandemic and these may be due to lifestyle changes adapted by the general population as a result of the lockdown. Hypernatriuria is a known risk factor for nephrolithiasis and reducing dietary sodium intake is often considered first-line dietary therapy for calcium stone formers. Other studies have shown that during the COVID-19 lockdown, dietary choices were limited to home-cooked meals which allowed patients to better identify their food choices, including salt reduction, limiting risk factors for stone formation. Salt reduction played a further protective role by likely resulting in a decrease in urinary calcium excretion as well, strengthening the lithoprotective effect of this diet against stones.
Furthermore, these changes appeared to persist in the “post-COVID” era of 2021 possibly due to the ongoing pandemic and continued fear of dining out despite lifting of government restrictions or due to sustained improvements to dietary habits. We speculate that these dietary changes played an important role in decreasing nephrolithiasis risk for stone-forming patients and recommend these patients continue their new dietary habits postpandemic.
Footnotes
Acknowledgment
This abstract was previously published in Abstracts of the 39th World Congress of Endourology: WCE 2022, abstract number MP12-08 in Journal of Endourology 2022 36:S1, A1–A315; DOI: 10.1089/end.2022.36001.abstracts
Authors' Contributions
B.S. performed the data collection, statistical analysis, and wrote the article. K.Z. performed the data collection, statistical analysis, and wrote the article. J.Y.L. performed data collection and reviewed the article. P.K., S.H., and H.S. performed data collection. D.S. reviewed the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.