
Abstract
Background:
Distinguishing between organ-confined disease and extraprostatic extension (EPE) is crucial for the treatment of patients with prostate cancer. EPE is associated with an increased risk of biochemical recurrence, positive surgical margins, and metastatic disease. An MRI-based EPE scoring system was developed by Mehralivand in 2019; however, it has not been adopted in the Urology community. The purpose of this study is to evaluate the association of MRI-based EPE scoring with the pathologic EPE (pEPE) after radical prostatectomy.
Methods:
We conducted a retrospective review on a prospectively collected database of male patients who underwent a prostate MRI with EPE scoring by a trained genitourinary radiologist and subsequent robotic radical prostatectomy at our institution from September 2020 to December 2022. The associations between MRI EPE (mEPE) score and the presence of EPE on surgical pathology (pEPE) were examined using multivariable logistic regression.
Results:
A total of 194 patients met inclusion criteria with a median age of 63 years and prostate specific antigen (PSA) 7 ng/mL. Among those with mEPE score 3, 96% had pEPE. Those patients with an mEPE score ≥2 had an increased risk of pEPE compared with those with mEPE score 0 (odds ratio 3.79; 95% confidence interval 1.28–11.3) Furthermore, those with an mEPE score 3 were significantly more likely to have pEPE compared with those with mEPE score 0, 1 and 2 independently.
Conclusion:
MRI EPE is a straightforward tool that strongly correlates with the presence of pEPE. If validated prospectively, this scoring system could assist in counseling patients regarding nerve-sparing approach.
Introduction
Prostate cancer is the second most prevalent cancer in men in the United States, with an estimated 268,490 cases diagnosed in 2022. 1 The past decade has seen significant progress in the diagnosis and treatment of prostate cancer. From the adoption of surgical techniques such as the hood and Retzius-sparing approaches, to the implementation of focal therapies, including high-intensity focused ultrasound and cryoablation, urologists are searching for enhanced techniques to minimize post-treatment urinary incontinence and erectile dysfunction without compromising cancer control. 2 –4
In addition to the rapid evolution of treatment modalities, the role of imaging, and particularly MRI, in the diagnosis and management of prostate cancer has made significant advancements. By offering enhanced visualization of potentially clinically significant lesions, MRI aids in patient selection for biopsy, provides data on tumor extent, and facilitates detection of disease progression for patients on active surveillance. 5 Major improvements in MRI capability, including multiparametric prostate MRI, have expanded the role of MRI in the diagnosis and surveillance of prostate cancer and may even allow for confirmatory biopsy to be deferred in patients on active surveillance. 6,7
Prostate MRI has also recently been utilized to assess the presence of extraprostatic extension (EPE), which has been associated with increased risk of recurrence, positive surgical margins, and metastatic disease. 8 In 2019, an MRI-based scoring system was developed by Mehralivand et al. 8 (Table 1). This scoring system, ranging from 0 to 3, assesses several radiological criteria, including curvilinear contact length, capsular irregularity and bulge, or evidence of extraprostatic spread. Despite studies demonstrating excellent inter- and intrareader correlation, the MRI EPE (mEPE) scoring system has not yet been widely adopted by the Urology community. 9 Streamlining the assessment of the presence and location of EPE could help guide the decision for nerve-sparing approach, provide additional evidence in the preoperative counseling of patients, and allow better prediction of adverse pathology after radical prostatectomy. The purpose of this study is to evaluate the association of MRI-based EPE scoring with the EPE based on surgical pathology.
Mehralivand Radiologic MRI EPE Scoring System
EPE = extraprostatic extension.
Materials and Methods
Following Institutional Review Board approval, a retrospective chart review was performed on a prospectively collected database of adult male patients (>18 years old) who had a diagnosis of localized prostate cancer. All patients underwent a robot-assisted laparoscopic radical prostatectomy at a single high-volume, tertiary-level academic institution. Inclusion criterion was the presence of preoperative prostate MRI in which the mEPE scoring system developed by Mehralivand et al. was documented. 8 All MRIs were read by board-certified genitourinary radiologists with subspecialty fellowship in abdominopelvic imaging or body MRI. In addition, the radiologists underwent further training for EPE scoring. An example of the scoring system is given in Figure 1. Both pre- and postoperative characteristics were collected from the database. In addition to demographic data, preoperative prostate specific antigen (PSA), Gleason score, and MRI data, including EPE score were extracted. Intraoperative nerve-sparing approach and postoperative surgical pathology data were also collected. Because our research question pertained solely to the correlation of EPE with MRI findings, margin status was not analyzed as part of this study.
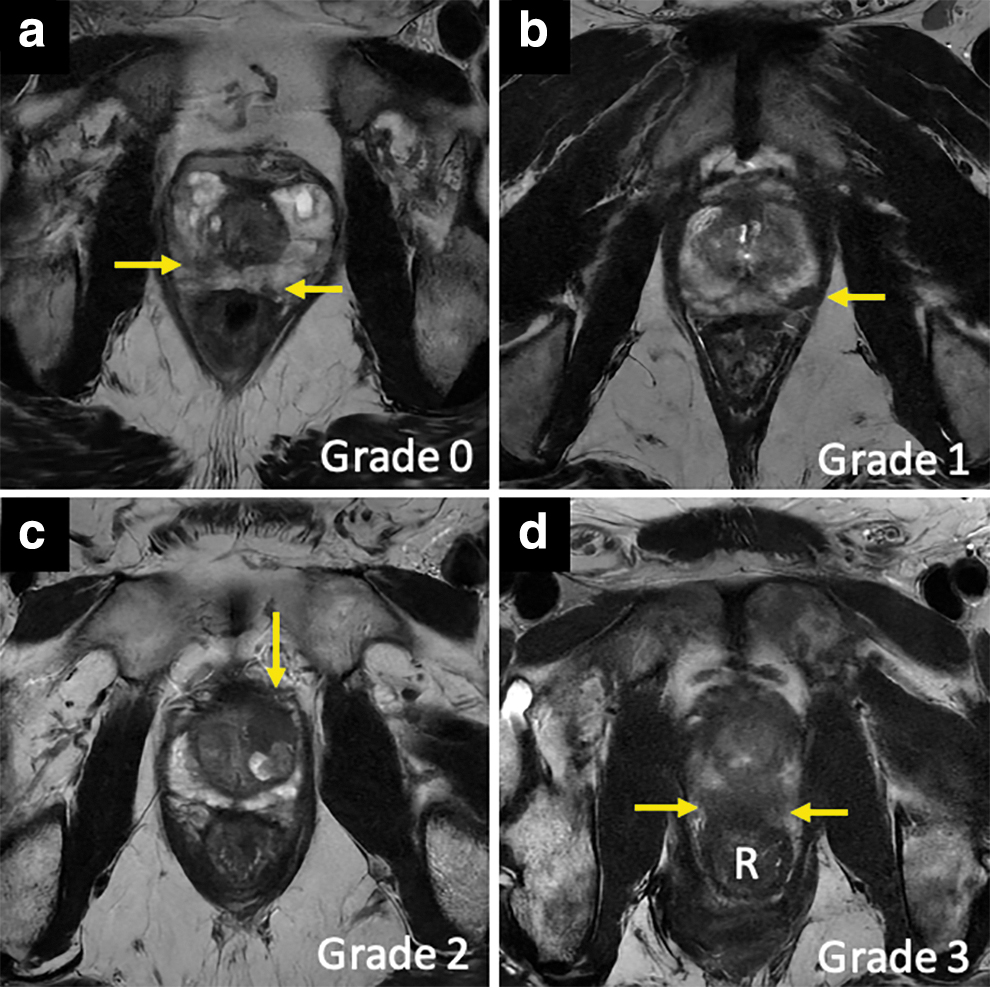
Examples of EPE grades 0 to 3 on MRI. Axial T2-weighted images of the prostate are shown in four different patients with pathology-proven prostate cancer. Images are cropped and magnified for clarity.
Prostate MRI technique
All MRI examinations are performed on a 3.0 T magnet (Premiere or 750w, General Electric, Milwaukee, WI, USA) using a multichannel body array coil. Patients are requested to refrain from (1) ejaculation 72 hours prior and (2) eating and drinking 4 hours before the exam. The prostate MRI examination comprises T2-weighted images in three planes, axial diffusion-weighted images with an apparent diffusion coefficient map, and T1-weighted fat-saturated gradient echo for multiphasic dynamic contrast-enhanced imaging. One milligram of intramuscular glucagon is administered to reduce bowel motion artifact. Intravenous gadobutrol contrast is administered at a standard 0.01 mMol/kg dose.
Statistical analyses
Baseline and clinical–pathological characteristics were summarized using medians and interquartile ranges (IQR) or frequency counts and percentages.
We examined the association of clinical features with the presence of EPE on pathology using univariable and multivariable logistic regression. Multivariable model included all the characteristics from the univariable analysis. The results are summarized using odds ratios (ORs) with 95% confidence intervals (CIs). Categorical variables were modeled as described in Table 2, except EPE scores 2 and 3 were combined together due to small cell values, whereas continuous variables were modeled as linear continuous variables.
Baseline Characteristics
IQR = interquartile range; pEPE = pathologic EPE; PI-RADS = Prostate Imaging Reporting and Data System; PSA = prostate specific antigen.
Statistical analyses were performed using R version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two-sided, and p-values <0.05 were considered statistically significant.
Results
A total of 330 patients underwent a robot-assisted laparoscopic radical prostatectomy since the implementation of the mEPE scoring system in September 2020 to December 2022. Of these, 194 met eligibility criteria and had an MRI scan with the prerequisite EPE scoring system. The median age at surgery was 63 (IQR 59–60) years with a median PSA of 7 (IQR 5–11) ng/mL. A total of 114 (59%) of patients had a Prostate Imaging Reporting and Data System (PI-RADS) 5 lesion by MRI with a median prostate volume of 41 mL 3 (IQR 32–58) (Table 2).
On surgical pathology, 95 (49%) patients had pathologic EPE (pEPE) (i.e., at least pT3a) disease. On bivariate analysis, higher mEPE score was associated with an increasing risk of pEPE, ranging from 23% for EPE 0 to 96% for EPE 3 (Table 3) (p < 0.05). Patients who had an mEPE score ≥2 were more likely to have pEPE compared with those with mEPE score of 0 (Table 4) (OR 3.79; 95% CI 1.28–11.3). Similarly, those with mEPE score 1 were almost three times more likely to have pEPE than patients with mEPE score 0 (OR 2.70; 95% CI 1.22–5.97). Lastly, those with an mEPE score 3 were significantly more likely to have pEPE compared with those with mEPE scores 0, 1, and 2 independently (p < 0.05).
EPE on Pathology Report By Highest Score
Univariable and Multivariable Logistic Regression Model—EPE on Pathology
p < 0.05.
CI = confidence interval; OR = odds ratio.
Among those with pEPE, 54 (59%) patients had nonfocal extension (extensive pEPE). There was no correlation between degree of extension (focal vs extensive) and EPE score. In fact, 13% of patients with EPE scores 0 to 1 also had extensive pEPE. The location of pEPE correlated with mEPE location 59% of the time with an unreported location in 20%.
Regarding nerve sparing, of those patients with mEPE score 3, 21 (91%) underwent either unilateral nerve-sparing or non-nerve-sparing technique (Table 5). Only one of these patients did not have pEPE. Of the 66 patients with mEPE 0, 33 (50%) underwent bilateral nerve sparing, however, only 14% of these had pEPE. Comparatively, 42% of patients with mEPE score 1 underwent complete nerve sparing with 15% having pEPE.
Nerve Sparing By EPE Score
C/P = complete/partial; mEPE = MRI EPE score.
On multivariable analysis, those patients with a PI-RADS 5 lesion were more likely to have pEPE than those with PI-RADS 4 or below (OR 2.67; 95% CI 1.04–6.86). Although PI-RADS score was significantly correlated with pEPE, Gleason score was not significantly associated. Patients with larger lesions were also found to have an increased risk of pEPE (2.57; 95% CI 1.66–3.97).
Discussion
Significant advancements have been made in the use of prostate MRI to aid in the diagnosis and treatment of prostate cancer. In the progression of MRI clinical adaptation, numerous MRI criteria have been employed to better predict EPE. 10 Mehralivand et al. developed an mEPE system to radiographically predict the presence of pEPE, 8 however, the accuracy and clinical utility of mEPE remains exploratory. In this study, we evaluated the association of mEPE with pEPE, which can aid in surgical planning (e.g., amount of nerve sparing) and patient counseling.
Several different methods of predicting EPE by prostate MRI have been proposed. Mehralivand et al. found that among a cohort of 553 patients, those patients with mEPE score 3 had a 66% positive predictive value of having postprostatectomy pEPE. 8 Park et al. compared four scoring systems (mEPE, European Society of Urogenital Radiology [ESUR] score, Likert scale, and capsular contact length) and found that mEPE more consistently correlated with the extent of pEPE postoperatively. 9 On the other hand, Reisaeter et al. found equivalent diagnostic performance between mEPE score and EPE Likert scoring. 11 Although both the ESUR and Likert scores provide good diagnostic performance, according to Asfuroglu et al., they are based on subjective qualitative measures, which makes reproducibility difficult and as for the ESUR, more difficult to interpret as well. 10 The advantage of the mEPE scoring system is its inclusion of both qualitative and quantitative criteria, such as tumor contact length, which makes it easily reproducible, while also maintaining the highest level of accuracy compared with the other measures. 10
Park et al., similarly concluded that the simplicity in assessing the MRI criteria of the mEPE score while still maintaining significant performance in detection of EPE compared with other scoring systems allows it to be more readily adaptable within the radiology community. 9 Despite these efforts, more work is required to validate these methods of EPE prediction before widespread adoption.
Our study found those patients who had mEPE score 3 on preoperative MRI had a 96% likelihood of EPE postprostatectomy. This is similar to the results found by Park et al. in which >92% of patients with mEPE score 3 had pEPE. 9 However, Mehralivand et al. found significantly lower detection rates of pEPE compared with our cohort. Only 66% of patients with mEPE score 3 had pEPE and only 38% of those with mEPE score 2 had pEPE in their cohort. 8 Conversely, 66% of our patients with mEPE score 2 had EPE at the time of surgery. This difference may be attributable to improved MRI technology (i.e., enhanced deep-learning denoising algorithms, newer-generation body array coils with a greater number of channels) and more experience in mEPE scoring since its inception. We found on univariable and multivariable logistic regression that patients who had an mEPE score ≥2 had a significantly increased risk of having EPE on pathology, when compared with individuals with a mEPE ≤1. Moreover, those with an mEPE score 3 were at a significantly increased risk of having pEPE compared with an mEPE score 2. While the rate of pEPE is understandably lower when comparing mEPE 0 or 1 vs 3, deciphering between mEPE 2 vs 3 may be challenging.
Although we found a significant increase in those with mEPE score 3 vs 2, this is mostly driven by the fact that only one patient in our cohort with mEPE score 3 did not have pEPE. While the differences between mEPE 0 and 3 are definitive, the radiologic findings between grades 1 and 2 may be subtle with a significant clinical impact. The presence of both a large curvilinear contact length (≥1.5 cm) and capsular irregularity/bulge portends an increased risk of EPE. In surgical planning, the surgeon should have a lower threshold for performing non-nerve or partial sparing on the affected side. Radiologic annotation of location and size of contact length and/or capsular irregularity is crucial for operative planning.
To our knowledge, the use of mEPE to plan nerve-sparing approach has not been explored. Nerve sparing may not only assist with regaining sexual function, but also urinary continence. 12 Currently, a variety of clinical features, including Gleason score, PSA density, volume of disease, age, and intraoperative surgeon discretion assist in planning for nerve-sparing technique without compromising oncologic control. 13,14 In our study, patients with mEPE score 3 were more likely to undergo unilateral or non-nerve sparing compared with those with mEPE score 0 or 1. With 96% of patients with mEPE score 3 having pEPE, the Mehralivand scoring system has been shown to accurately identify patients likely to have extracapsular extension, precluding a nerve-sparing technique.
Despite the accuracy of the preoperative MRI, we resected nerves in a number of patients with a low mEPE score and subsequently no EPE. Of patients with mEPE score of 0 or 1, 14% to 15% had pEPE, yet we performed bilateral nerve sparing in only 50% and 42%, respectively. While patients with mEPE score 3 may benefit from a more conservative unilateral or bilateral nerve-sparing approach, the study provides evidence that those with mEPE score 0 or 1 may safely undergo more aggressive nerve sparing without oncological compromise. A prospective study that assesses preoperative mEPE score-based nerve-sparing plan with intraoperative approach would clarify the feasibility of mEPE score in nerve sparing.
There are several limitations within our study. First, this is a retrospective analysis conducted from a single academic center, which might limit the generalizability of our results to nonacademic centers. Furthermore, the location of the pEPE correlated with mEPE 59% of the time. This was limited by the fact that the location of the EPE was not noted in the pathology report in 20% of cases, thus limiting the ability to ascertain if the mEPE correlated with the same pEPE identified on the pathology report. Although it is possible that many of these cases of mEPE did actually correlate to the pEPE, prospective pathologic validation of this scoring system will be necessary. Lastly, all of our studies were performed using a 3Tesla MRI and thus our results are not applicable to 1.5T systems.
Despite the limitations, our data confirm that mEPE can help identify patients with pEPE before treatment. Further prospective work can expand on identifying the efficacy of mEPE score in predicting pEPE location and resulting nerve-sparing approach.
Footnotes
Acknowledgment
The abstract was previously published in Abstracts of the 40th World Congress of Endourology: WCE 2023. Published Online: September 27, 2023,
Authors' Contributions
U.B.: Conceptualization, methodology, validation, formal analysis, investigation, data curation, writing––original draft, visualization, and writing––review and editing. A.E.: Conceptualization, methodology, validation, investigation, data curation, writing––original draft, and writing––review and editing. J.B. and T.W.: Investigation, and writing––original draft. S.K.: Software and formal analysis. C.C.: Investigation, resources, data curation, and project administration. J.S.: Investigation, resources, and data curation. L.L.T.: Methodology, investigation, writing––review and editing, visualization, and supervision. J.M.-D.F.: Investigation, resources, data curation, and writing––review and editing. B.G., P.C., and A.A.W.: Conceptualization, methodology, validation, writing––review and editing, and supervision.
Author Disclosure Statement
The authors declare there is no relevant disclosure or conflicts of interest that relate to the research presented in this study.
Funding Information
There was no funding for this study.