
Abstract
Objective:
To assess the outcomes of redo laparoscopic pyeloplasty (RLP) in pediatric patients with recurrent ureteropelvic junction obstruction (UPJO) in contrast to redo open pyeloplasty (ROP). In addition, evaluate the feasibility and efficacy of RLP as a treatment modality for recurrent UPJO in children.
Materials and Methods:
The data of 44 patients from March 2012 to March 2022, who underwent redo pyeloplasty, were retrospectively reviewed. In Group RLP, the children underwent RLP, whereas ROP was attempted in Group ROP. Demographics, clinical manifestations, surgical duration, hospitalization duration, complication rates, and treatment success were examined within the respective groups. Moreover, preoperative and postoperative measurements of anterior–posterior diameter of the renal pelvis (APD), preoperative assessment of differential renal function (DRF), and the percentage of improvement in DRF (PI-DRF) were subject to analysis.
Results:
The study included 28 patients who underwent RLP (Group RLP), and 16 patients who underwent ROP (Group ROP). In all cases, the Anderson–Hynes technique was employed. There was no significant difference between the two groups regarding age, body mass index, gender distribution, affected side, preoperative APD, postoperative APD, and preoperative DRF. In comparison to Group ROP, Group RLP exhibited a shorter hospitalization duration, a longer surgical procedure duration, and a higher percentage improvement in PI-DRF. The median follow-up period for Group RLP was 25 months, whereas it was 25.5 months for Group ROP. Notably, the success rates were similar between the two groups, with a success rate of 89.2% in RLP and 87.5% in ROP (p = 0.634).
Conclusion:
RLP has a comparable success rate to ROP and is a safe, effective, and feasible procedure for the treatment of failed pyeloplasty in children.
Introduction
Ureteropelvic junction obstruction (UPJO) is the most common cause of hydronephrosis in children, with an incidence rate of 1:750–1500. 1 –3 Anderson–Hynes dismembered pyeloplasty has long been regarded as the gold standard owing to its consistently high success rates, 4 including open Anderson–Hynes dismembered pyeloplasty and minimally invasive surgery procedures (laparoscopic pyeloplasty and robot-assisted laparoscopic pyeloplasty). 5 However, ∼11% of patients undergoing pyeloplasty may necessitate repeat procedures. 6 Redo pyeloplasty (open, laparoscopic, and robot-assisted laparoscopic) has demonstrated superior effectiveness compared to endourological procedures such as Double-J stent insertion, balloon dilatation, and endopyelotomy. 7 –11
Redo laparoscopic pyeloplasty (RLP) offers several advantages, including reduced postoperative pain, and less need for postoperative analgesia, ample working space, a shorter hospital stay, and secure anastomosis. 12 –14 In this study, the outcomes of RLP in children were investigated and compared with a cohort of redo open pyeloplasty (ROP). Therefore, the hypothesis of the study was that RLP is also feasible and effective compared with ROP for the surgeon experienced in laparoscopy.
Materials and Methods
Study design
In this study, patients who underwent redo pyeloplasty at our institution from March 2012 to March 2022 were retrospectively reviewed. Patients who underwent RLP were designated as Group RLP, whereas patients who underwent ROP were designated as Group ROP. Patients who presented with concurrent urinary system malformations such as horseshoe kidney, pelvic kidney, duplication of the collecting system, and vesicoureteral reflux, as well as those with bilateral UPJO or incomplete data or who were lost to follow-up, were excluded from the study. The Medical Ethics Committee of First Affiliated Hospital of Guangxi Medical University has approved this retrospective study (2023-E729-01).
The preoperative data, intraoperative parameters, and follow-up information of the patients were collected. The preoperative data included the age, body mass index (BMI), side, gender, clinical presentation, preoperative anterior–posterior diameter of the renal pelvis (APD), and preoperative differential renal function (DRF) of the patients. The intraoperative parameters included operative time and re-obstruction reasons. The follow-up information included hospitalization duration, postoperative APD, preoperative assessment of DRF (PI-DRF), complications, and success. Complications were graded according to the Clavien–Dindo classification. 15 Success was defined as relief of clinical symptoms, stable or improved DRF, and improvement of the APD. Renal function evaluation was conducted using diuretic renography with diethylenetriaminepentaacetic acid (DTPA), whereas the measurement of APD was performed through ultrasound.
Surgical technique
All patients underwent dismembered Anderson-Hynes pyeloplasty for their repairs. In Group RLP, patients were laid on their healthy side, with the affected side elevated 45° to 70°. A 5 or 10 mm trocar was established through the umbilicus, and insufflation was maintained at 8–12 mm Hg (1 mm Hg = 0.133 kPa). One 5 mm or 3 mm trocar was inserted at the midway of the line between the anterior superior iliac spine and the umbilicus, and another one was inserted at the midway of the line between the xiphoid process and the umbilicus as working ports. A transperitoneal approach was adopted in Group RLP. The colon was mobilized to remove the adhesions.
The procedure involved first identifying the normal ureter distally and then dissecting it proximally toward the renal pelvis to expose both the renal pelvis and ureter. Subsequently, the ureteropelvic junction (UPJ) was identified, and the reasons for the restenosis of the initial pyeloplasty were determined. Complete release of perirenal and ureteral adhesions was achieved, and fibrous tissue was removed using a combination of blunt and sharp dissection techniques. The UPJ was then dissected, and the segment with restenosis was excised, along with ∼1 cm of the adjacent ureter. In cases with a long segment stenosis, which would not allow anastomose without tension, a renal pelvic flap about 1 cm wide was cut, with length depending on the length of the restenosis segment, so as to achieve tension-free anastomosis.
The flap's feeding vessel had to be preserved carefully. The posterior edge of the renal pelvic flap was anastomosed to the posterior wall of the ureter side-to-side. Then, a Double-J stent was inserted retrogradely. Subsequently, the anterior edge of the renal pelvic flap was anastomosed to the anterior wall of the ureter side-to-side and then the residue flap was tubularized using a continuous suture technique. Finally, continuous sutures were used to close the bilateral renal pelvis, completing the pyeloplasty procedure. A tube drain was inserted into the pelvic cavity. Notably, in Group ROP, the pyeloplasty technique followed the same steps as Group RLP.
The drain was removed when the drainage volume was less than 10 mL in 24 hours. Intravenous antibiotics were administered until the patients were discharged, and after discharge, prophylactic antibiotics (cephalosporin at a dose of 50 mg/kg per day) were continued for one week. The Double-J stent was removed between 8 and 12 weeks after the surgery. All patients underwent clinical follow-up to monitor for pain or urinary tract infections (UTIs). Ultrasound examinations were scheduled at 1, 3, 6, and 12 months after removal of the Double-J stent. Diuretic renogram with DTPA was also required 6 and 12 months after removal of the Double-J stent. Furthermore, yearly assessments, including ultrasound and diuretic renography with DTPA, were conducted as part of the long-term follow-up protocol.
Statistical analysis
Data were presented as mean ± standard deviation and the respective groups were compared using Student's t-test in variables with normal distribution. For variables with non-normal distribution, data were presented as median (interquartile range [IQR]) and the groups were compared using Mann–Whitney U-test. Categorical variables were compared using the Pearson's chi-square test, Yates' continuity correction chi-square test, and Fisher's exact test. Statistical analysis was performed using SPSS version 24 software (IBM SPSS Statistics, Armonk, NY: IBM Corp).
Results
In total, 44 patients who underwent redo pyeloplasty were identified, which included 28 patients who underwent RLP and 16 patients who underwent ROP. There was no difference in age, BMI, gender, side and clinical presentation between the groups (Table 1). The reasons for restenosis are presented in Table 2. Briefly, Group RLP had 14 cases of simple anastomotic stenosis, whereas Group ROP had 10 cases. In addition, Group RLP had 1 case of vascular compression combined with anastomotic stenosis, 6 cases of adhesion band compression along with anastomotic stenosis, and 7 cases of anastomotic adhesion. On the other hand, Group ROP had 2 cases of adhesion band compression combined with anastomotic stenosis and 4 cases of anastomotic adhesion.
Demographic Data
BMI = body mass index; IQR = interquartile range; RLP = redo laparoscopic pyeloplasty; ROP = redo open pyeloplasty.
Reasons of Restenosis
As shown in Table 3, the preoperative APD was 48 (45, 63) mm in Group RLP, whereas 50 (46, 54) mm in Group ROP; there was no difference between both groups (p = 0.470). The postoperative APD in Group RLP was 20 (17, 33) mm, which was not significantly different from Group ROP with a postoperative APD of 26 (10, 45) mm (p = 0.170). In Group RLP, preoperative DRF was 22.0% (15.0%, 33.0%), whereas that of Group ROP was 31.1% (21%, 36%), indicating no significant difference (p = 0.110). The median PI-DRF in Group RLP was 7.46% (2.70%, 10.57%), which was higher than Group ROP (p = 0.019).
Clinical Data
APD = anterior–posterior diameter of the renal pelvis; DRF = differential renal function; PI-DRF = percentage of improvement in DRF.
The mean hospitalization duration of Group RLP was 6 ± 1.6 days, which was shorter than Group ROP (p = 0.011). The mean operative time of Group RLP was 189.8 ± 52.5 minutes, which was significantly longer than Group ROP (p = 0.013). Six patients in group RLP and 2 patients in group ROP used the renal pelvic flap technique, which is described in the surgical technique. As shown in Table 4, all 8 patients had a reduction of hydronephrosis, in addition to an improvement of DRF. One patient underwent nephrostomy because of postoperative urinary extravasation from the ureteropelvic anastomosis, which recorded as major complications (Clavien ≥ III) in Group RLP, whereas no such event (Clavien ≥ III) was recorded in Group ROP (p = 1.000). And the patient was applied renal pelvic flap to completed pyeloplasty.
Data for 8 Patients who Used Renal Pelvic Flap Technique
The median follow-up period of Group RLP was 25.0 (11.2, 33.7) months, whereas the median follow-up period of Group ROP was 25.5 (22.2, 41.2) months, indicating no significant difference between the two groups (p = 0.164). At the end of follow-up, three patients in Group RLP and two patients in Group ROP exhibited persistent hydronephrosis and a deterioration in DRF that necessitated reoperation. In addition, these patients experienced persistent UTIs. The overall success rate in Group RLP was 89.2%, whereas that in Group ROP was 87.5%, which indicated no significant difference.
Discussion
Recurrent UPJO stands out as the primary complication after pyeloplasty, and prior research has demonstrated that around 11% of patients who underwent primary pyeloplasty required a subsequent surgical intervention. 6 Recurrent UPJO can cause repeated febrile UTI, pain, persistent severe hydronephrosis, and impairment of renal function. 13,16,17 Timely and proactive interventions are essential once it is identified after primary pyeloplasty. Previous studies have reported several procedures for the treatment of recurrent UPJO, including Double-J stent placement, endopyelotomy, balloon dilatation, and redo pyeloplasty. 7 –10,18,19 The overall success of endopyelotomy ranges from 25% to 94%.
However, in cases where patients have a long narrowed ureteral segment, severe hydronephrosis, and concurrent cross vessels, the long-term outcomes may be less favorable. 9,10,19 –21 Existing research has revealed that the advantages of double stent placement and balloon dilation include fast recovery, few complications, and absence of incision, whereas the overall success rate ranges from 29.4% to 46.1%, making it a suitable option for carefully selected patients. 7,8 ROP has been considered the gold standard procedure for patients with recurrent UPJO over the past several years, and with the development of minimally invasive techniques, RLP and robot-assisted RLP have been extensively adopted in experienced institutions.
In this study, 28 patients with recurrent UPJO underwent repair through RLP, and 16 patients were managed using ROP. These findings indicate that intraoperative restenosis in these cases was attributed to factors such as anastomotic stenosis, cross vessels, adhesion band compression, and anastomotic adhesion. Asensio et al. 22 reported that unrecognized crossing vessels were the cause of obstruction in three out of five patients in their study, which is consistent with this research. As revealed in previous studies, restenosis after primary surgery can be attributed to factors such as dense adhesions, a redundant pelvis, adhesions causing obstruction, a highly inserted ureter, a long segment stricture, and a twist in the anastomosis. 13,17
In our experience, it is crucial to meticulously preserve the feeding vessels when dismembering the renal pelvis and ureter. In addition, it is advisable to avoid direct clamping of mucosa of the pelvis and ureter. Identifying the lowest point of the renal pelvis is of utmost importance, and Cao et al. 23 previously reported a method to achieve this recognition. Furthermore, it is essential to identify cross vessels during the primary surgery.
Previous studies reported that the transperitoneal approach is commonly used in RLP, as well as the retroperitoneal approach. 24,25 In this study, the transperitoneal approach for treating recurrent UPJO was adopted to dissect through extensive adhesions in the retroperitoneal space, and to limit the dissection to the UPJ and proximal ureter.
Abdel-Karim et al. 13 reported that RLP resulted in a shorter hospital stay and longer operative time compared to ROP. At the same time, the complication rates and success rates between the two procedures showed no significant difference, which aligns with the findings of this study. Furthermore, these findings are supported by Li et al., 12 who reported comparable preoperative and postoperative APD in RLP and ROP, with the complications and success rate similarly exhibiting no significant difference. Similar findings have also been reported in other research. 24 It can generally be considered that RLP has the advantage of fast recovery. Given the substantial presence of adhesions, it is imperative to perform meticulous intraoperative dissection. This accounts for the extended duration of RLP compared to ROP.
There are few studies in which the DRF of recurrent UPJO after redo surgery was assessed. In this research, the PI-DRF of RLP was 7.46% during a 25-month follow-up period, surpassing the corresponding rate for ROP. Such results reveal that RLP may be more effective than ROP. In research conducted by Al-Hazmi et al., 17 the preoperative split renal function was 32% (IQR, 24%–46%), which postoperatively increased to 33% (IQR, 21%–39%) after a median follow-up period of 29 months. Such results differ from those of this study, and could be attributed to the lower preoperative DRF in this study. Castagnetti et al. 26 also reported that patients with moderately impaired preoperative function were most likely to exhibit functional improvement after surgery.
In this study, 6 patients in group RLP using the renal pelvic technique which is described in the surgical technique, whereas 2 patients in group ROP. One patient in RLP who used the renal pelvic flap suffered from urinary extravasation from the ureteropelvic anastomosis postoperatively. And postoperative ultrasound showed some small blood clots accumulated around the Double-J stent, blocking the Double-J stent and causing urinary extravasation. We analyzed that the cause of clot formation was blood oozing from the surgical marginal of renal pelvic flap and ureter. Thence this patient underwent the nephrostomy, and after Double-J stent removal, the nephrostomy tube was removed after the assessment of patency of UPJ and ureter by antegrade pyelography. During the follow-up period, the patient demonstrated an improvement in DRF and a reduction of hydronephrosis.
In addition, all the patients who used the renal pelvic flap had a favorable effect, no patient suffered the worse hydronephrosis and DRF. It showed that in cases with a long segment stenosis, which would not allow anastomose without tension, using a renal pelvic flap was also effective and feasible. The overall success rate of RLP in this study was 89.2%, whereas previous studies have reported success rates between 78.9% and 100%, 7,16,17,27 indicating that these findings are consistent with those of previous research. Patients who underwent robot-assisted laparoscopic pyeloplasty produced the same effect. Jacobson et al. 28 reported that out of 36 children who underwent robot-assisted laparoscopic re-operative repair, only one patient exhibited worsening hydronephrosis in the postoperative ultrasound evaluation.
RLP has well-established advantages, including reduced morbidity, reduced hospitalization duration, and reduced pain compared to ROP. 14 However, this challenging technique must be performed by experienced surgeons owing to the substantial adhesions resulting from prior surgeries. 24 Based on our experience, intra-abdominal adhesions should not be considered a contraindication for redo laparoscopic surgery. The benefits of RLP encompass a clearer surgical field of vision, enhanced exposure, improved anatomical visualization, and greater precision in intraoperative dissection and suturing. Furthermore, laparoscopic surgery allows the identification of distal ureter in cases of multisegment stenosis.
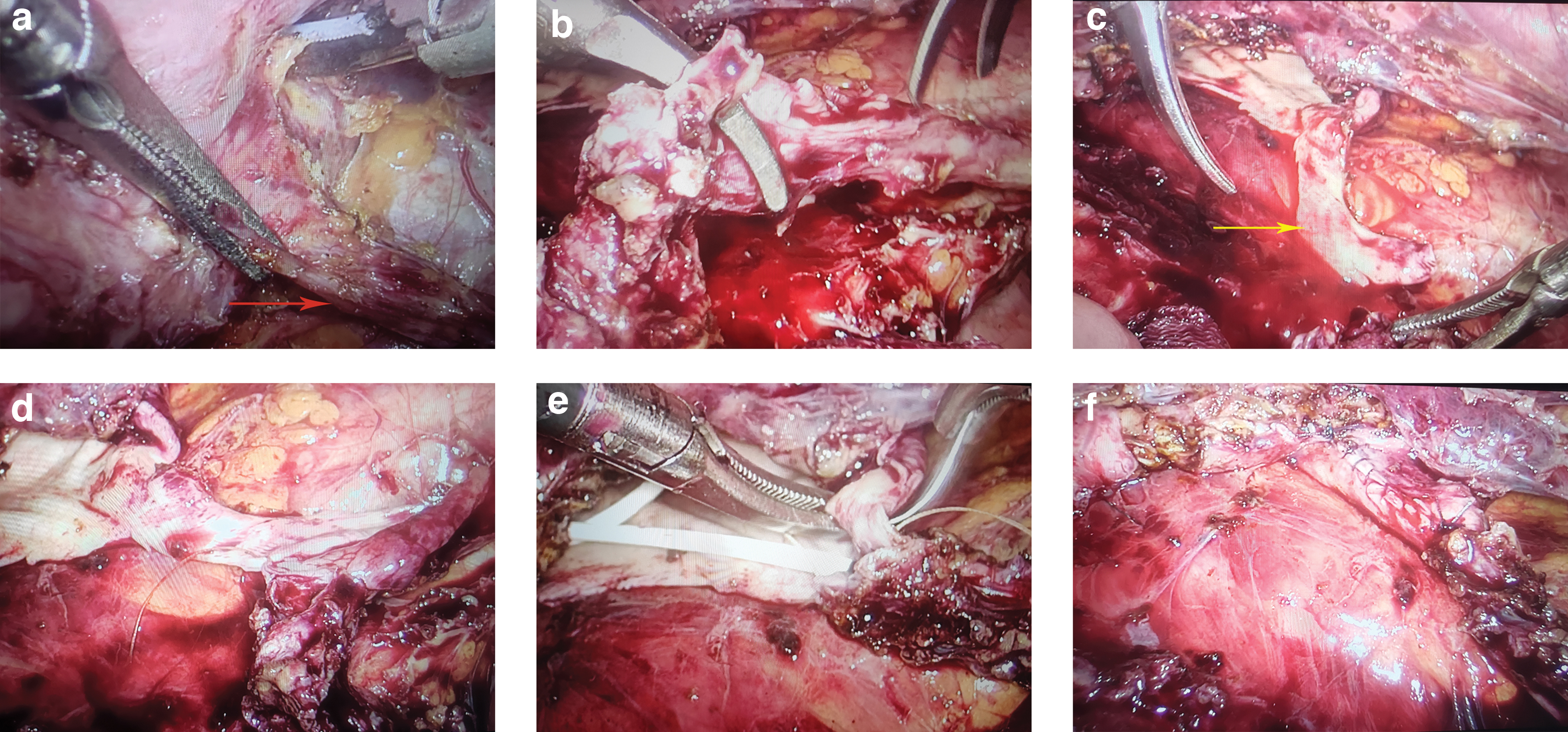
Surgery steps of redo laparoscopic pyeloplasty.
Nevertheless, this study is subject to several limitations, primarily stemming from its nonrandomized, single-center design, as well as its relatively small patient sample size and absence of long-term follow-up data. Therefore, further research in this field is warranted to provide more comprehensive insights in the future.
Conclusion
RLP is an effective and feasible procedure for recurrent UPJO, with a success rate on par with ROP. It should be contemplated as a viable alternative for specific pediatric cases after unsuccessful primary pyeloplasty.
Footnotes
Authors' Contributions
Q.K.X.: Writing–original draft, investigation, formal analysis, and writing—review and editing (lead). C.J.W.: Conceptualization (supporting) and writing—review and editing (equal). C.S.: Writing—review and editing (equal) and formal analysis (supporting). B.S.: Writing—review and editing (equal) and methodology (supporting). Y.L.: Writing—review and editing (equal) and investigation (supporting). J.Q.W.: Writing—review and editing (equal) and investigation (supporting). C.C.: Conceptualization (lead), methodology (lead), and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (82060129), the “Medical Excellence Award” funded by the Creative Research Development Grant from the First Affiliated Hospital of Guangxi Medical University (2017026).