
Abstract
Introduction:
The most recent American Urological Association (AUA) Guidelines advocated laser enucleation of the prostate (LEP) as a size-independent surgical option for benign prostatic hyperplasia (BPH). Despite its endorsement by AUA and the growing body of evidence supporting its safety and efficacy, the utilization of LEP remains limited in the United States. This study aimed to evaluate the utilization trends and perioperative outcomes of LEP compared with other surgical procedures used for BPH management.
Methods:
A retrospective cohort analysis was performed using American College of Surgeons National Surgical Quality Improvement Program data from 2011 to 2020. Patients undergoing prostatectomy for BPH were identified using specific current procedural terminology (CPT) codes. Baseline demographic data, preoperative risk factors, and postoperative outcomes were collected. Multivariable logistic regression was employed to assess predictors of holmium laser enucleation of the prostate (HoLEP) utilization and postoperative complications.
Results:
Out of 8,415,549 patients, 95,144 underwent prostatectomy for BPH. Procedures included HoLEP 5305 cases, transurethral resection of the prostate (TURP) 57,803 cases, repeated TURP (re-TURP) 5549 cases, photoselective vaporization of the prostate (PVP) 23,739 cases, and simple prostatectomy 2748 cases. HoLEP utilization showed a gradual increase, from 4.8% in 2015 to 7.6% in 2020. Multivariable regression revealed that HoLEP selection significantly increased from 2016 to 2020 (odds ratio [OR]: 1.251, p < 0.001), and there was less likelihood of HoLEP selection for African American patients (OR: 0.752, p < 0.001). HoLEP had significantly lower complication rates, including urinary tract infections, blood transfusions, 30-day readmission, and reoperation.
Conclusion:
Despite underutilization, the adoption of HoLEP has slightly increased since 2015, rising from 4.8% in 2015 to 7.6% in 2020. The underutilization could be attributed to a lack of availability and the steep learning curve.
Introduction
Benign prostatic hyperplasia (BPH) is a common urologic problem, the incidence increases with age with peak incidence at age 75 to 79 years. 1 Transurethral resection of the prostate (TURP) has long been the gold standard surgical intervention for BPH; however, some challenges cause its use to be limited. These include large prostate volumes, which makes patients more prone to intraoperative and postoperative complications. 2 Historically, open simple prostatectomy (OP) was the common modality available for the management of markedly huge prostates, despite it being associated with a high risk of complications. 3
The increasing prevalence of BPH in elderly patients coupled with morbidity associated with simple OP and the strides made in medical technology led to the development of surgical alternatives. Recently, the evolution of holmium laser enucleation of the prostate (HoLEP) has addressed the challenge of managing larger prostates with safety and efficacy. 4 Since its introduction, a growing body of evidence has demonstrated that HoLEP provides more favorable outcomes than the conventional TURP. These advantages included a reduction in postoperative catheterization duration, intraoperative bleeding, and shorter hospital stays. 5 In comparison with simple OP, HoLEP provides superior outcomes in terms of blood loss, hospital stay, and catheterization time. 6
Other alternative technologies for laser prostatectomy include photoselective vaporization of the prostate (PVP). Studies comparing PVP with TURP demonstrated comparable outcomes in terms of International Prostate Symptom Score (IPSS) and peak urinary flow rates. However, PVP offers advantages over TURP, including reduced catheterization time and a shorter hospital length of stay. 7,8 Initially, PVP was limited to small-to-moderate size prostates based on the data showing high retreatment rates associated with large prostates. 9 Recently the introduction of 120 W and currently 180 W greenlight “high performance system” (HPS) resulted in adequate tissue removal and lowered retreatment rates allowing its application for large prostates. 10,11
According to the latest American Urological Association (AUA) guidelines, HoLEP is recommended as a size-independent surgical option for BPH. Furthermore, it also recommended HoLEP for patients at higher risk of bleeding. 12 Despite mounting evidence substantiating the superiority of HoLEP over traditional TURP, its adoption remains limited, constituting only 4% of cases, as reported by a recent study evaluating the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2011 to 2015. 13
The purpose of this study was to provide an update on the national utilization trend of HoLEP using data obtained from the ACS-NSQIP database. In addition, it examines factors influencing its adoption.
Materials and Methods
Data source
We conducted a retrospective cohort analysis for deidentified data derived from the ACS-NSQIP registry. The ACS-NSQIP serves as a repository of surgical outcome data sourced from multiple health care centers across the United States. Its primary objective is to enhance the quality and safety of surgical care. The database comprehensively collects information on patients' demographics, preoperative risk factors, intraoperative variables, and postoperative outcomes.
Study design and cohort definitions
The ACS-NSQIP was queried for patients undergoing prostatectomy from 2011 to 2020. We extracted and analyzed current procedural terminology (CPT) codes that correlated with HoLEP (CPT 52649), TURP (CPT 52601), TURP for regrowth (CPT 52630), PVP (CPT 52648), and both suprapubic (CPT 55821) and retropubic (CPT 55831) approaches for simple prostatectomy. It is worth noting that the current CPT coding system does not differentiate between robotic and simple prostatectomy procedures, therefore, robotic cases were presumed to be included in the simple prostatectomy cases.
Study variables
We collated baseline demographic data including age, race, functional status before surgery, and comorbidities such as diabetes and bleeding disorders. In addition, preoperative laboratory values and the year of the operation were evaluated. Predictors influencing the choice between HoLEP or alternative approaches were assessed based on the aforementioned factors.
Analysis of trends
To investigate trends in the management of HoLEP over time, we evaluated frequency over other approaches across the years. Statistical analyses were conducted using R Studio. Descriptive statistics were used to analyze clinicodemographics through either t-test or chi-square test for categorical variables. We performed bivariate analyses to determine the association between patient characteristics undergoing HoLEP and other approaches. Subsequently, a multivariable regression model was performed to address cofounders.
Results
A total of 8,415,549 patients underwent proctectomy at participating ACS-NSQIP institutions between 2011 and 2020. After applying our study criteria, a total of 95,144 patients underwent prostatectomy for BPH. The specific procedures performed were as follows: HoLEP in 5305 cases, TURP in 57,803 cases, repeated TURP (re-TURP) in 5549 cases, PVP in 23,739 cases, and simple prostatectomy in 2748 cases (Fig. 1).
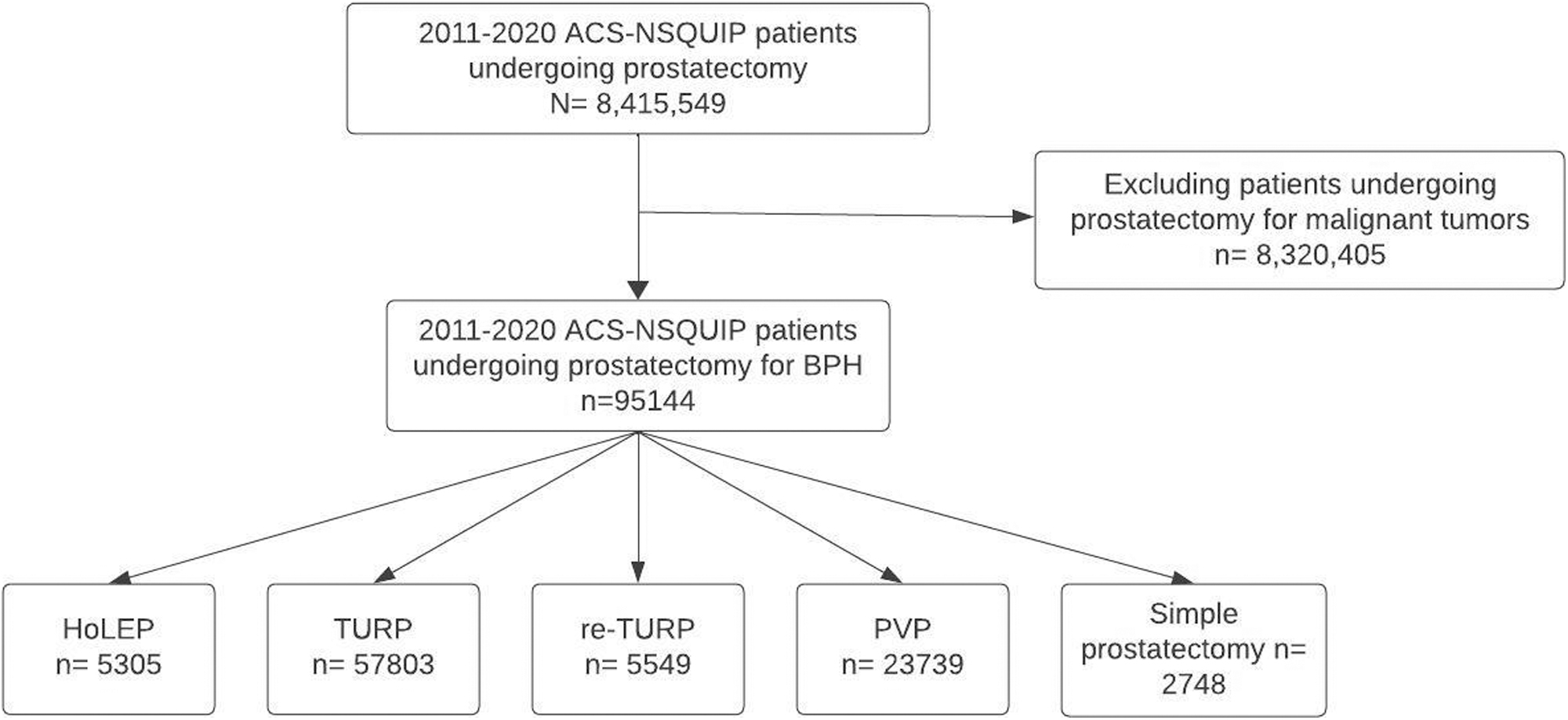
Identification of patients undergoing prostatectomy for BPH. BPH = benign prostatic hyperplasia.
Baseline characteristics
Table 1 summarizes the baseline characteristics for each treatment group from 2011 to 2022. Age distribution showed significant differences across the treatment groups (p ≤ 0.001), with the youngest mean age observed in the HoLEP group (69.58 ± 8.58). Categorically, patients managed with HoLEP were more commonly aged between 61 and 70 years, whereas patients >70 years were similarly represented among the study groups. Racial distribution was significantly different (p < 0.001), with white patients being more frequent in all groups, especially the HoLEP group (80.0%). The presence of bleeding disorders showed significant differences (p < 0.001), with the highest prevalence observed in the PVP group (4.5%).
Baseline Characteristics for the Study Cohort
ASA = American Society of Anesthesiology; BUN = Blood urea nitrogen; HCT = Hematocrit; HoLEP = holmium laser enucleation of the prostate; INR = international normalised ratio; PVP = photoselective vaporization of the prostate; re-TURP = repeated transurethral resection of the prostate; SD = standard deviation; TURP = transurethral resection of the prostate.
Predictors of HoLEP
The multivariable regression analysis (Table 2) showed a significant association between HoLEP selection in the years 2016 to 2020 compared with 2011 to 2015 (odds ratio [OR]: 1.251; [95% confidence interval, CI: 1.123–1.393]; p < 0.001). In contrast, there is a reduced likelihood of HoLEP being selected for African American patients compared with white patients (OR: 0.752; [95% CI: 0.609–0.927]; p < 0.001). Increasing age, diabetes, bleeding disorders, functionally dependent, and the American Society of Anesthesiology (ASA) class are not associated with HoLEP utilization.
Predictors for Holmium Laser Enucleation of the Prostate Utilization
Analysis of trends over time
There was a progressive increase in the absolute number of HoLEP procedures performed annually between the years 2015 and 2020 (Fig. 2). Moreover, the percentage of patients selected for HoLEP out of the total cases demonstrated a significant upward trend (Fig. 3), increasing from 4.8% in 2015 to 7.6% in 2020 (r 2 = 0.98 [p < 0.001]) (Fig. 4).
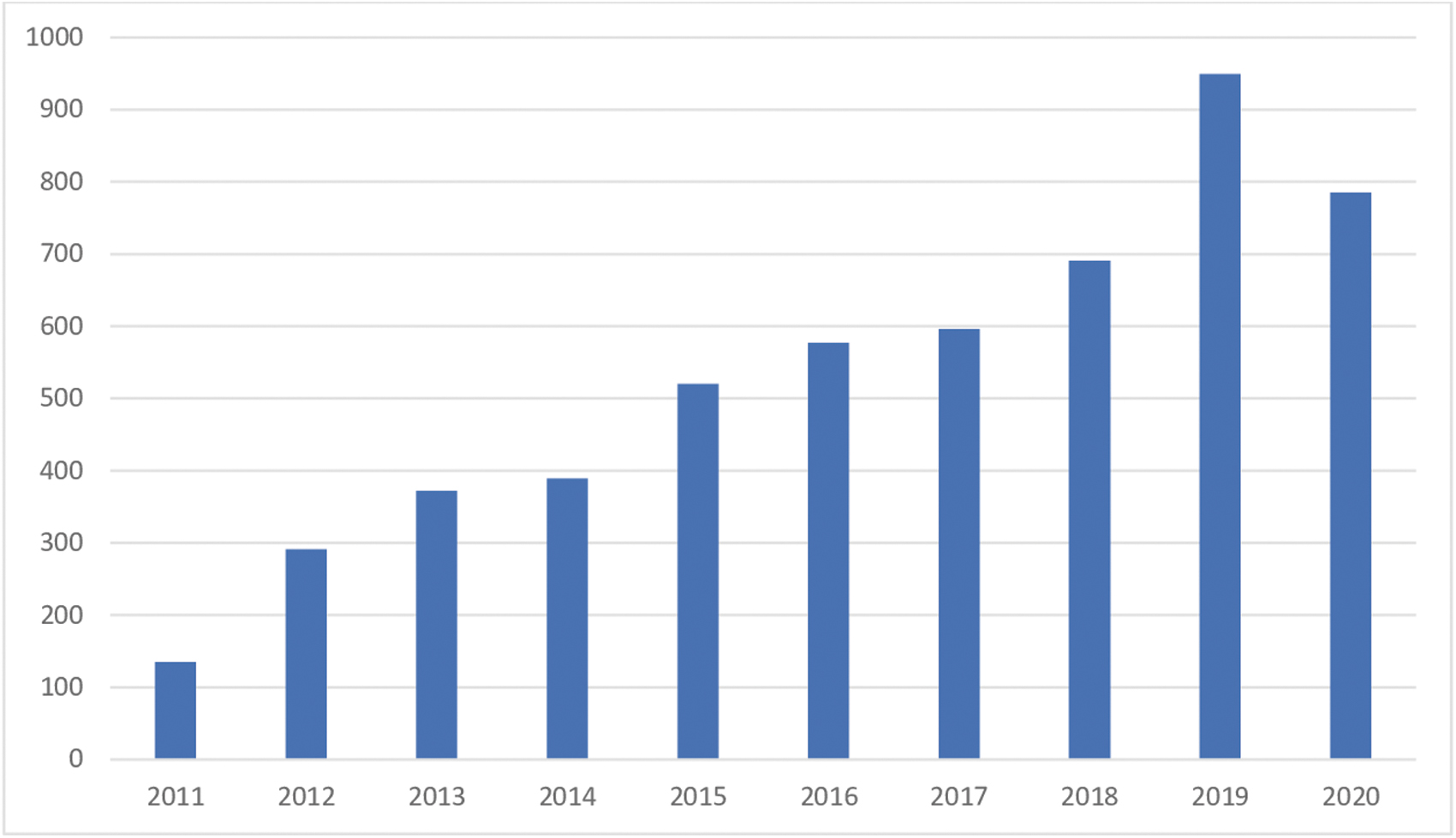
Trend of HoLEP utilization in the United States from 2011 to 2020. HoLEP = holmium laser enucleation of the prostate.
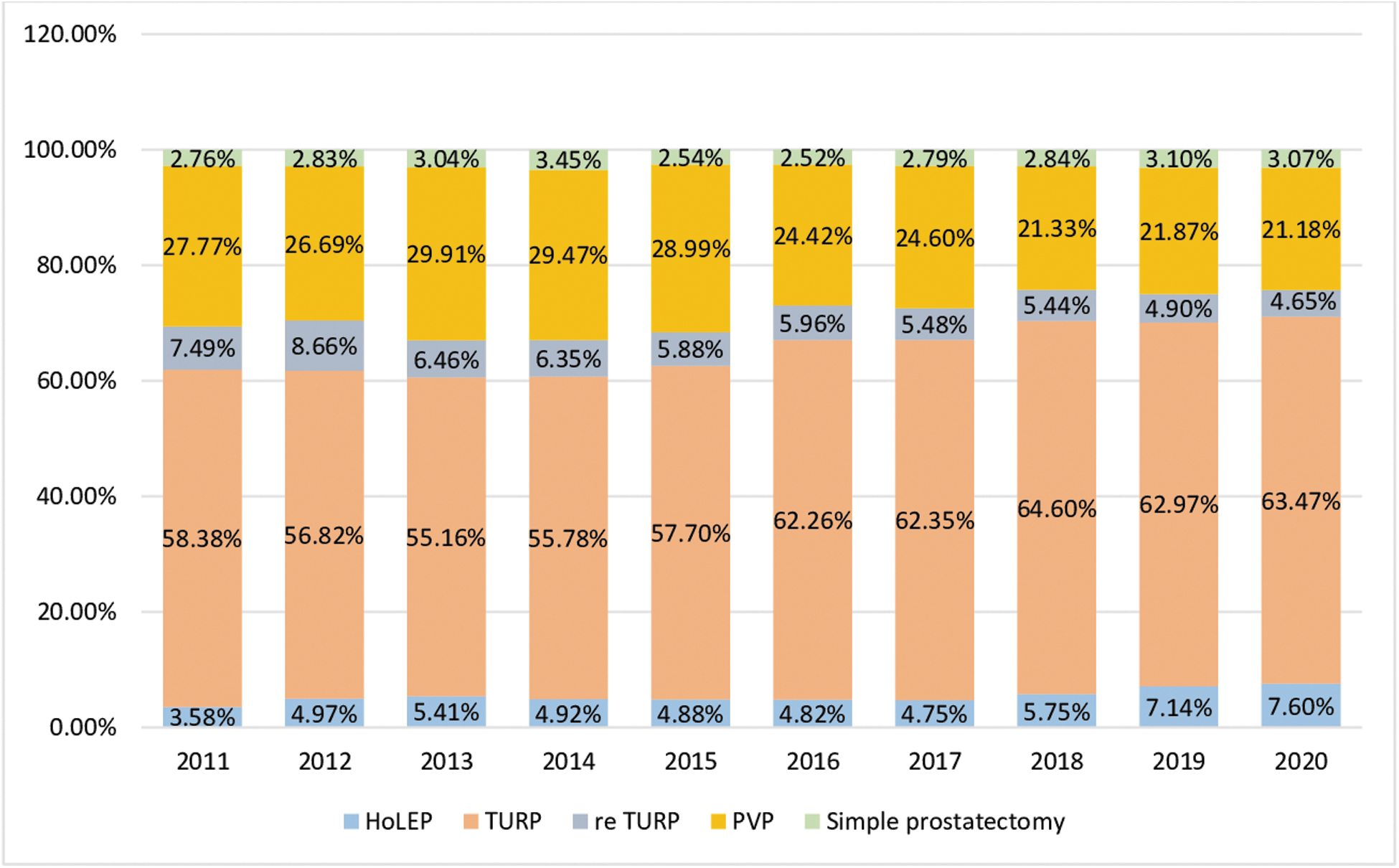
Proportional HoLEP procedures compared with other approaches (2011–2020).
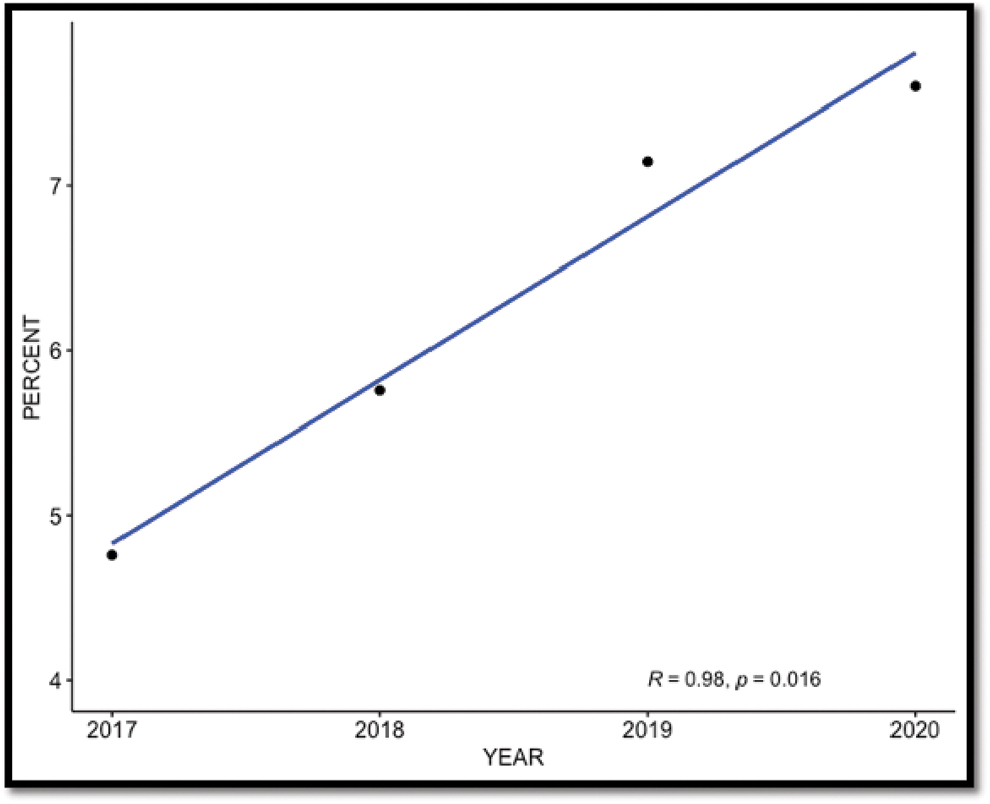
Correlation between proportion of HoLEP cases and years.
Complications
Table 3 describes the incidence of post procedure complications. HoLEP exhibited a lower rate of urinary tract infections at 3.1%, compared with TURP (5.1%), re-TURP (4.6%), PVP (5.6%), and simple prostatectomy (6.0%; p < 0.001). Similarly, HoLEP showed a lower 30-day readmission rate at 3.9%. In multivariate analysis (Table 4), when considering various predictors for operative complications and comparing HoLEP with non-HoLEP procedures, HoLEP exhibited a significantly lower OR (0.719; [95% CI: 0.648–0.798]; p < 0.001).
Complications
UTI = urinary tract infection.
Predictors for Operative Complication
Discussion
Prior research using the ACS-NSQIP database has ∼4% of patients undergoing HoLEP for BPH management. 13 This study provides an updated assessment of the utilization trends of HoLEP in the management of BPH. We observed that the primary treatment modality for most cases is TURP. HoLEP utilization showed slightly increasing trends (4.8% in 2015 to 7.6% in 2020). This increase is a coincidence with the AUA's 2018 recommendation for HoLEP as a size-independent surgical approach for BPH treatment. 12 However, despite this increase, TURP increased at a greater rate (58.38 in 2015% to 63.47% in 2020). In contrast, the frequency of re-TURP and PVP has shown a decreasing trend.
We evaluated the factors influencing the selection of HoLEP. Intriguingly, parameters such as age, diabetes, bleeding disorders, functional dependence, and ASA class failed to predict HoLEP utilization. It was anticipated that parameters such as the presence of bleeding disorders would predict HoLEP utilization, given the evidence that HoLEP is a safer option for patients with bleeding tendencies. 14 However, our analysis revealed that this expectation was not met, suggesting the presence of barriers hindering the wider adoption of HoLEP. It is crucial to emphasize that the underutilization of HoLEP carries consequences for patients with comorbidities or patients at risk of bleeding. As per HoLEP being safer for these certain patients, patients who are deprived of this service might experience avoidable complications. 15
In this study, HoLEP outperformed TURP and simple prostatectomy in terms of postoperative complications. Our findings are consistent with a growing body of evidence demonstrating the superiority of HoLEP over alternative prostate surgical procedures. A recently published metanalysis that included 11 randomized controlled trials (RCTs) comparing HoLEP with TURP demonstrated that HoLEP has superior outcomes.
These advantages include shorter hospital stay and reduced bleeding, in addition to improved quality of life (QoL) scores and lower post voiding residual (PVR) volumes at both 1 and 2 years, moreover, the maximum urinary flow rate (Qmax) at 6 and 12 months. 5 Furthermore, when assessed against OP for prostates exceeding 100 g, HoLEP emerged as a favorable option with benefits in terms of reduced bleeding, lower transfusion rates, shorter catheterization durations, and hospital stays. 6
It is pertinent to highlight that HoLEP transcends the limitations of being exclusively viable for markedly larger prostate volumes. A study by Zhang and colleagues 16 corroborated HoLEP's efficacy across a spectrum of prostate volumes, surpassing the outcomes of TURP. Furthermore, HoLEP has exhibited its merit in addressing specific patient conditions, as evidenced by its ability to achieve a 100% catheter-free rate in cases of urinary retention. 17 Similarly, for patients afflicted with atonic bladder conditions, a noteworthy 95% success rate is achieved in normal voiding function. 18
As evidence accumulated, the AUA guidelines endorsed the utilization of HoLEP as a size-independent intervention for BPH and recommended the consideration of HoLEP for medically complex patients and patients at risk of bleeding. 12
Despite its evident advantages HoLEP, there is still a sluggishness to adapt this technology. The underutilization can be attributed to various factors, mainly the steep learning curve precluding its broad adoption. 19 The procedure demands meticulous dissection that involves surgical plans and requires skills in endoscopic technique. 20 However, strategies such as dedicated training programs encompassing 25 to 50 cases can effectively overcome this learning curve. 17 Regional disparities further contribute to the overall underutilization of HoLEP. Analysis conducted in 2014 revealed that a significant number of states in the United States had minimal hospital-referring regions performing a low number of HoLEP procedures annually. 21
Financial factors also play a role including the lack of economic incentives and higher total costs compared with alternative procedures. 21
The limited exposure to HoLEP during residency programs also contributes to its underutilization. Surveys conducted among residents have shown lower exposure to HoLEP than other surgeries for BPH. Furthermore, residents expressed a relatively lower perceived need for additional exposure to HoLEP compared with other procedures. This lack of exposure during training can influence future practice patterns and familiarity with the HoLEP technique. 22 Considering the substantial benefits HoLEP offers, its incorporation into residency training should be considered.
Other reasons include criticism directed at HoLEP, with concerns about its association with higher rates of postoperative persistent retrograde ejaculation and stress urinary incontinence (SUI) especially in the early learning curve. 23 Robert et al. 19 reported some surgeons discontinued HoLEP after the first case experienced severe stress incontinence. Elshal and colleagues 24 found 28% of the patients suffered from SUI during the learning process. These concerns have captured the attention of urologists who argue that robotic surgery provides a better continence rate, as it enables the removal of the adenoma without manipulation of the sphincteric mechanism. 25 Surgeons who have mastered robotic simple prostatectomy often achieve superior results compared with HoLEP in terms of continence rates. 23,26
In our study, PVP showed a decreasing trend from 2017 to 2020. The Comparing GreenLight-XPS Laser Vaporization of the Prostate and Transurethral Resection of the Prostate for the Treatment of Benign Prostatic Obstruction (GOLIATH) trial, a randomized controlled study with a 2-year follow-up, concluded that PVP demonstrated noninferiority to TURP in terms of functional outcomes and safety profile, however, PVP had significantly shorter catheterization time and hospital stay. 8 In a comparison between HoLEP and PVP, an RCT including prostate volumes exceeding 60 g demonstrated superior outcomes for HoLEP in reducing PVR and lower postoperative transrectal ultrasonography volume.
Nevertheless, PVP was associated with a 22% conversion to TURP. 27 A retrospective analysis comparing HoLEP and PVP for long-term QoL and IPSS reduction demonstrated that HoLEP exhibited a greater magnitude of improvement in IPSS and higher Qmax values. 28
The most common criticism of PVP is the lack of long-term follow-up data; however, recent evaluations have assessed the retreatment rates for PVP at 5 years, which were reported as and 8.9% and 10.3%. 29,30 More favorable outcomes were reported by Hueber and colleagues 11 at 24 months (1.2%) and by Stone and coworkers 10 (2.9%). In our study, both HoLEP and PVP demonstrated lower complication rates than TURP and simple prostatectomy. Despite presenting a viable approach for addressing large prostates and high-risk patients, the reasons for the observed decreasing utilization trends remain unclear.
Limitations of this study include its retrospective nature and the absence of CPT codes for robotic simple prostatectomy precluding the inclusion of this procedure in the analysis. In addition, the study scope is confined to data available only until the year 2020, potentially overlooking subsequent changes in procedural trends. Another notable limitation is the unavailability of prostate volume data, preventing the categorization of trends based on prostate size.
Data Access Statement
We utilized the NSQUIP database for prostatectomy data spanning the years 2011 to 2020.
Ethics Statement
This study did not require ethics approval.
Footnotes
Authors' Contributions
Conceptualization was primarily conducted by A.M.M., whereas methodology was jointly developed by A.A., A.E., and F.A. M.B. did the statistical analysis with E.E.D. Data curation was the responsibility of A.E. The initial draft of the article was composed by A.A., A.E., K.A.S., and F.A., with substantial contributions to the writing and review by S.T. and A.M.M. The supervision of the project was carried out by M.L. and A.M.M.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.