
Abstract
Purpose:
To assess the ability to deliver full-thickness bladder wall cryoablation through a cystoscopic approach using a new closed-loop 6F cryocatheter and thermal dose-controlled protocol.
Materials and Methods:
Evaluations were conducted using a chronic porcine model wherein 10 lesions/animal were created throughout the bladder (bladder wall, trigone region, ureteral orifice, and distal ureter). A 6F cryocatheter was passed through the working channel of a flexible cystoscope. Single 1- and 1.5-minute freeze protocols in a saline environment were evaluated and resultant lesion size was determined. A laparoscopic approach was utilized to observe the transmural extension of the ice propagation.
Results:
Studies demonstrated the generation of transmural lesions characterized by full-thickness histologic necrosis after freezing for 1.5 minutes regardless of tissue thickness (range 2–12 mm). All animals were found to have good overall health (maintained weight, appetite, mobility, and energy levels) throughout the recovery period. No significant deviations were noted in complete blood count and serum chemistry bloodwork except for elevated creatine kinase levels. Importantly, no fistulas or perforations were noted.
Conclusions:
The cryocatheter was able to rapidly and effectively freeze the bladder wall through a cystoscopic approach. The results showed the ability to consistently ablate an ∼1 cm diameter and up to 1.2 cm deep using a single 1.5-minute freeze protocol. Analysis of the ablation efficacy revealed ∼80% destruction within the frozen mass. Although further testing and refinement are needed, these studies demonstrate the potential of this new approach to provide a next-generation strategy for the treatment of bladder cancer.
Introduction
Frequent recurrence of non-muscle invasive bladder cancer and the high morbidity associated with treatment of muscle invasive bladder cancer coupled with increasing incidence underscore the need for new strategies to treat bladder cancer (BC), especially for penetrating T2 to T4 disease. 1,2 Although neoadjuvant chemotherapy after radical cystectomy in patients with invasive BC continues to flourish, 3,4 there have been few advances in ablative approaches.
Ablative therapies (radiofrequency ablation, high focused ultrasound, laser, electrocautery, and cryoablation [CA]) have demonstrated potential efficacy for treating BC, 5 –10 yet use remains limited. The first four treatments heat tissue to lethal temperatures (70°C–90°C) and kill primarily through direct heat damage and necrosis, whereas CA cools tissue and kills through freeze rupture, necrosis, and apoptosis. 11 CA is often considered a dated approach.
However, recent technological advances, 12,13 use as a combinatorial therapy 14,15 and the activation of a systemic immune response after freezing, 16 –18 have repositioned CA on the cutting edge. 19 Freezing has been shown to be as, or more, effective and safer than heat-based ablation. 11,14 Several studies have demonstrated CA to be a safe and effective therapeutic option, including for treating penetrating T2 to T4 disease using, primarily, a percutaneous approach. 6,7,20 –22 Others 21,23 have reported on a cystoscopic-based approach.
Hruby et al. reported on the transurethral CA of the bladder (TUCAB) using a rigid cryoprobe demonstrating that TUCAB is safe and effective. 23 However, the authors noted several issues limiting clinical utility, including the use of a rigid cystoscope and cryoprobe, requirement of laparoscopic access to observe the freeze process, inability to target the trigone region or the ureter orifice (UO), and that the procedure needed to be performed in a gaseous environment. Other issues, including uniformity of ablation, depth of lethal temperature penetration, incompatibility with liquid environment application, concern with bladder wall perforation, necessity of laparoscopic access, procedure time, and inability to target metastatic disease, have further limited clinical adoption. 7,13,17,23 –25
Recently, we developed a new flexible cystoscope compatible cryocatheter (UroAblate) which, when paired with the Pressurized Subcooled Nitrogen (PSN) cryoconsole, delivers ultracold ablative temperatures to a targeted tissue in a closed-loop manner. 12,13 Furthermore, the system also allows for setting and maintaining the ablation tip at a predefined temperature (ablative dose) through an integrated thermocouple within the catheter. The intent of this study was to evaluate this new cryocatheter and controlled thermal dose delivery method (temperature-controlled transurethral cryoablation of the bladder [TC-TUCAB]) for the cystoscopic CA of bladder tissue.
Materials and Methods
Cryoablation of bladder tissue
In vivo testing was performed using four female Yorkshire pigs in the chronic 7-day survival study at NASMA (Coon Rapids, MN, USA) under IACUC approval. Animals underwent general anesthesia and subjected to a combined cystoscopic and transperitoneal laparoscopic approach. Each animal had two laparoscopic trocars placed through the lower abdomen near the urinary bladder (left and right of midline) to allow for thermocouple (where possible) and laparoscopic camera insertion to observe ice formation on the bladder outer wall.
A flexible aScope 4 Cysto cystoscope (Ambu, Inc., Columbia, MD, USA) was inserted into the bladder using a standard transurethral approach. Once inserted, the bladder was filled with physiologic saline. A 6F (2.0 mm) cryocatheter (UroAblate, CPSI Biotech, Owego, NY, USA) was inserted through the cystoscope working channel, the ablation tip advanced 2 to 3 cm beyond the end of the cystoscope and placed perpendicularly against the bladder wall under observation through the cystoscopic and laparoscopic cameras (where possible). Single 1- and 1.5-minute freeze applications using a temperature control protocol of −30°C and −50°C were evaluated. A minimum of 10 lesions/animal were created throughout the bladder (bladder wall, trigone region, UO, and distal ureter).
In procedure assessment
Time to ice formation on the inner and outer wall, freeze duration, and lesion location were recorded. Real time observation of the freeze process was monitored through the cystoscopic and laparoscopic cameras. After freezing (last 5 seconds), lesions were visually assessed to approximate luminal frozen tissue diameter. Time to tip release from the tissue and tissue thaw was also recorded. Once all freezes were complete, before animal revival, bladder integrity was visually assessed through the cystoscopic camera and cystogram with contrast.
Postsurgical assessment
Animals were maintained for 7 days and assessed daily for overall health (weight, appetite, activity, water intake, and urine output). Subjects were assessed for hydronephrosis on day 4 through ultrasound (US) and upon sacrifice through visual inspection. Upon sacrifice, necropsy evaluations of observed pathologic changes were performed. Bladders were removed, inflated with saline to assess integrity, and then fixed with luminal installation of 10% Neutral Buffered Formalin.
After fixation, the bladder mucosa was exposed, lesion sites identified, labeled, and imaged before sampling for histopathology. Representative samples were processed routinely for paraffin embedding and stained with hematoxylin and eosin (H&E) for evaluation. Quantitative assessment of lesion size (diameter and depth at the center of the lesion) and notation of transmurality was recorded. Standard complete blood count (CBC) and serum chemistry analysis was conducted presurgery and at sacrifice to allow for the identification of any alterations outside of normal ranges.
Data analysis
All CA protocols were performed on a minimum of two animals and had a minimum of six lesions (repeats). Data were grouped by freeze time and temperature and averaged (±standard deviation) to determine mean lesion diameter and depth. Percent transmurality for each protocol (time and temperature) was calculated. Statistical significance was determined using single-factor analysis of variance.
Results
Freeze procedure
All animals underwent TC-TUCAB using the 6F cryocatheter. The average ablation (freeze/thaw) time (min:sec) ranged between 1:28 (±0:16) and 2:25 (±0:19) for the −30°C cohorts and 1:37 (±0:18) and 1:55 (±0:14) for the −50°C cohorts for the 1- and 1.5-minute freeze protocols, respectively (Table 1). The average time to initial visual ice on the inner wall was 10 seconds (±4) and 6 seconds (±2) and on the outer wall was 21 seconds (±8) and 11 seconds (±0.9) for the −30°C and −50°C 1- and 1.5-minute cohorts, respectively.
Procedure Freeze–Thaw Data
SD = standard deviation.
Visual estimations of frozen tissue luminal diameters ranged between 8 and 10 mm for −30°C and between 12 and 15 mm for −50°C lesions. Regardless of the freeze time or temperature, probe tip release after freezing averaged 29 seconds (±17). After the freeze–thaw process, no bleeding was observed from any of the ablation sites. Cystogram analysis revealed no bladder wall irregularity, perforations, or extravasation. Representative images from the cystoscopic and laparoscopic cameras are depicted in Figure 1.
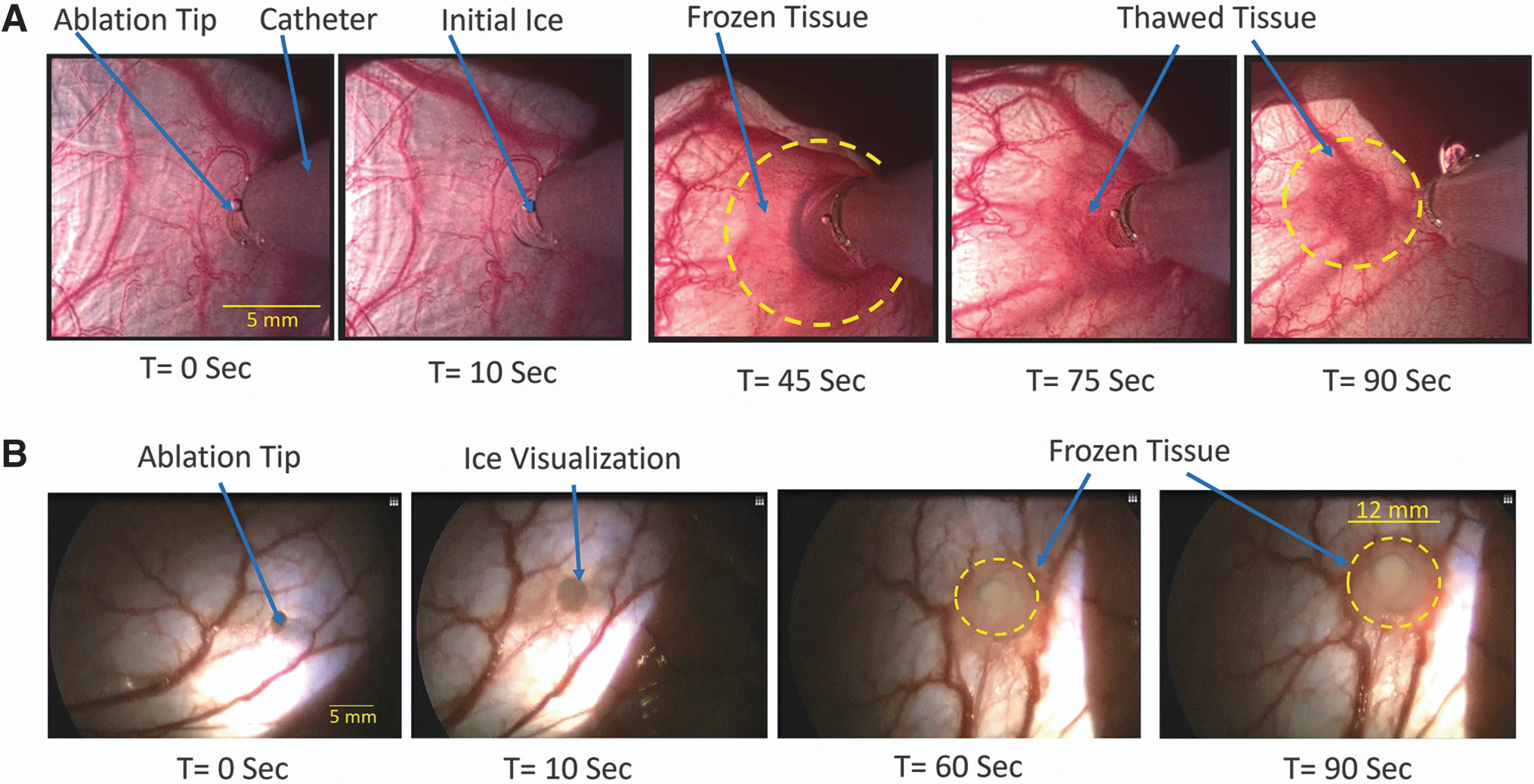
Representative images of the inner and outer surface of the porcine bladder during cryoablation.
Overall health
All animals survived and were found to remain in good overall health, maintaining weight, appetite, mobility, energy levels, and so on, through the 7-day recovery period. US examination of the bladder and kidneys on day 4 of recovery revealed no fistulas or any abnormal swelling or blockages. Urine output decreased on days 1 and 2 postablation but returned to normal by day 3. CBC and serum chemistry revealed no significant deviations for any parameter except for creatine kinase (CK), wherein three animals were found to have elevated CK levels at sacrifice (Table 2).
Average Complete Blood Count and Serum Chemistry Data

Highlighted to emphasis Elevated Level.
A/G = albumin/globulin ratio; AST = aspartate transaminase; BASO = basophils count; BUN = blood urea nitrogen; CO2; EOS = eosinophil count; GGT = gamma-glutamyl transferase; HCT = hematocrit; HGB = hemoglobin; ISE-Cl = ion specific electrode-Chlorine; ISE-K = ion specific electrode-Potassium; ISE-Na = ion specific electrode-Sodium; LYMPH = lymphocyte count; MCH = mean corpuscular hemoglobin; MCHC = mean corpuscular hemoglobin concentration; MCV = mean corpuscular volume; MONO = monocyte count; MPV = mean platelet volume; NEUT = neutraphill count; PLT = platelet count; RBC = red blood cell count; RDW = red cell distribution width; WBC = white blood cell count.
Histopathology analysis
Gross pathologic tissue observation revealed no fistulas in the bladder walls or in any of the surrounding tissues (bowel or abdomen) (Fig. 2). Examination of the kidneys revealed no obvious swelling or other damage/abnormalities from the CA procedure. Analysis of bladder wall thickness revealed a high degree of variability ranging from 2.1 to 10.4 mm with an average thickness of 6.5 mm (±2.6).
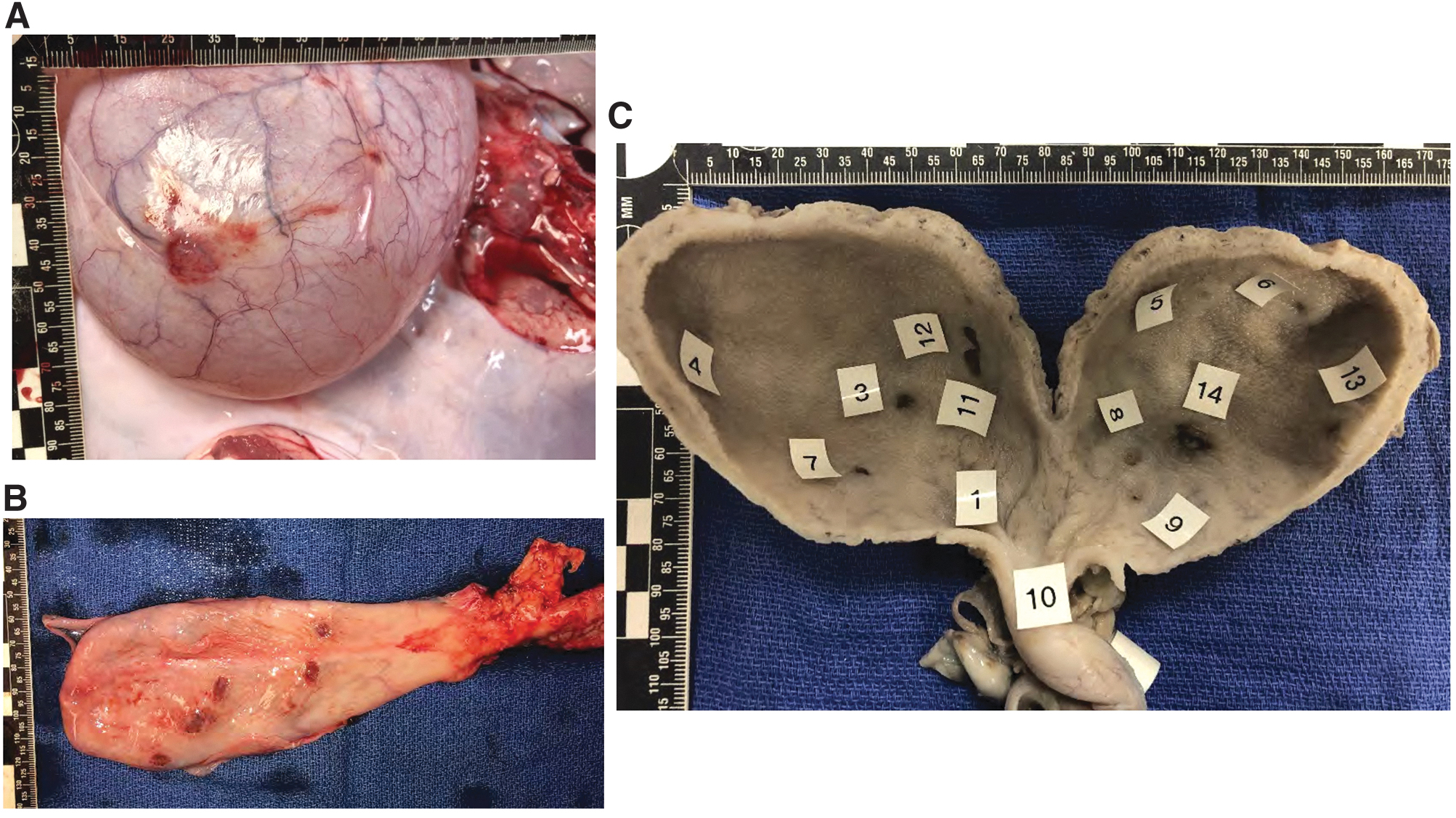
Representative necropsy images of porcine bladder 7 days after cryoablation.
Analysis of the 1-minute freeze cohort revealed an average ablation depth ≤3 mm for both the −30°C and −50°C protocols (Table 3). Histologically, lesions were characterized as partial thickness with superficial smooth muscle attenuation, separation, and loss (Fig. 3A). Furthermore, minimal to mild submucosal edema, extravasated erythrocytes, and minimal vascular necrosis and thrombi were observed (Fig. 3B). Application of the 1.5-minute freeze yielded an increase in the average ablation depth to 8.3 mm (±1.65) and 6.1 mm (±2.66) for the −30°C and −50°C cohorts, respectively (Table 3) (p = NS). Examinations revealed an average lesion diameter of 11.1 mm (±6.35) and 10.75 mm (±3.52) for −30°C and −50°C, respectively (Table 3). Statistical comparison of the −30°C and −50°C 1.5-minute data yielded no significant difference in ablation depth (p = 0.04) or maximum diameter (p = 0.9).
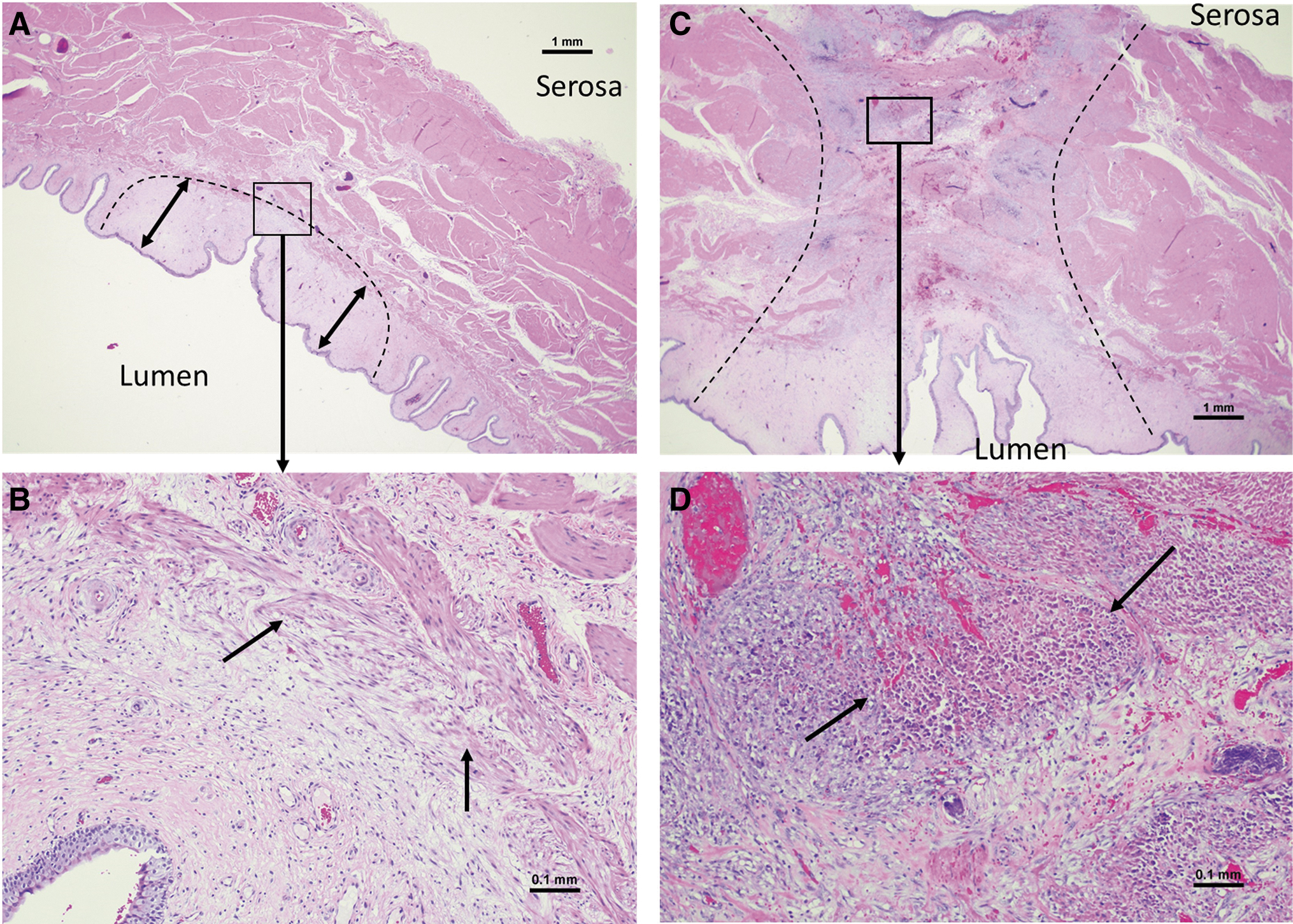
Histologic micrographs of bladder wall tissue after a 1- and 1.5-minute freeze protocol and 7-day recovery.
Average Lesion Created with the 6F Cryoablation Catheter
Histologic examination of the 1.5-minute cohort revealed transmural well-demarcated ablation injury for the majority of lesions (Fig. 3C). The lesions were characterized by necrosis extending from the mucosa to the serosa. Submucosal edema, fibrin, hemorrhage, and necrosis were found to extend into muscularis. Smooth muscle necrosis and mineralization along with interstitial inflammation were observed at the serosal surface. Inflammation consisted of neutrophils, macrophages, and lesser lymphocytes (Fig. 3D).
Discussion
CA has been investigated for the ablation of BC in preclinical and clinical settings. 6,7,20,22,23 Although effective, these studies revealed numerous technical challenges (requirement of insufflated bladder [gas environment], limited control of the ablation process/nadir temperature, and need for monitoring outer wall temperature, among others) limiting clinical utilization. Rigid cryoprobes often require a percutaneous approach necessitating piercing of the bladder wall. Spray-based cryocatheters for cystoscopic-based freezing require a drained insufflated bladder and provide limited penetration of ablative temperatures, restricting their use to superficial disease. 6,7,23,25 –27
One of the biggest concerns with BC ablation, CA, or other is compromise of bladder integrity during or after a procedure. 6,7,13,23,26,27 Compromising bladder wall integrity is associated with the delivery of excessive ablation (freezing or heating) throughout the target tissue. The challenge is that application of ultracold temperatures is necessary to drive the minimal lethal temperature (MLT) of −25°C through the entire tissue to effectively ablate the target. 13,28 The crux of the situation is, given the variability in bladder wall thickness (among others) when attempting to attain full-thickness lesions, overfreezing can occur resulting in fistula development—an issue similar to overheating/overtreating with hyperthermia and electrocautery approaches. 5,8 –10,26,27,29,30
We previously reported on the ability to rapidly deliver ultracold temperatures to ablate bladder tissue through a transurethral approach using PSN and an 8F cryocatheter. 13 That study also identified several issues, including lack of cystoscope compatibility and confirmed fistula development (2 of 24 lesions [8.4%]) after extended freezing (5 minutes) and attainment of outer wall to temperature <−60°C (luminal temperatures <−100°C). For all other lesions where the outer wall temperature was >−50°C and/or an exposure time of 1 minute, no fistulas were reported. 13
Given those promising results and in attempt to overcome the identified issues, we developed a new cystoscope compatible 6F cryocatheter and evaluated a temperature-controlled CA protocol (TC-TUCAB). Our goal was to develop an approach for which rapid controlled full-thickness ablation could be attained while eliminating the risk of fistula development independent of bladder wall thickness. Furthermore, our objective was to apply this using a standard cystoscopic approach wherein ablation is conducted in a liquid environment. Based on previous studies suggesting increased risk of fistula after extended exposure to temperatures <−60°C, we evaluated a TC-TUCAB protocol wherein ablation tip temperature was maintained at −30°C or −50°C (±5°C). These temperatures were selected in an effort to deliver <−25°C (BC MLT 23,28 ) across the bladder wall while eliminating the possibility of tissue exposure to temperatures <−60°C regardless of the freeze time. As such, theoretically the only issue that remains would be to determine the freeze time and catheter hold temperature (dose) necessary to attain full-thickness ablation in a warm saline environment.
Results demonstrated UroAblate was easily utilized in conjunction with a flexible cystoscope. The cryocatheter was found to have minimal impact on maneuverability and deflection. This enabled targeting of sites throughout the bladder, including the UO, bladder neck, and trigone region with the cystsoscope fully retroflexed. Results demonstrate the ability to effectively attain full-thickness bladder wall ablation with no fistula development while having no negative impact on overall animal health.
The application of a 1-minute −30°C or −50°C freeze protocol resulted in partial thickness ablation (<3 mm). Luminal diameter of the 1-minute lesions was found to be larger after freezing at −50°C compared with −30°C (p < 0.01; Table 3). Increasing the CA time to 1.5 minutes yielded an increase in the average ablation depth to ∼8 mm resulting in >75% of lesions yielding full-thickness necrosis (−30°C = 75% and −50°C = 83%; Table 3; Fig. 3). Regardless of the bladder wall thickness, the average cross-sectional diameter of the ablated tissue on the serosal surface was 11 mm for the 1.5-minute protocols.
Visual assessment of luminal frozen lesions revealed −30°C yielded a smaller frozen diameter compared with −50°C. We hypothesize that the warm saline environment had a greater impact on the −30°C condition yielding a smaller frozen mass. This is supported by the differential in time to ice (all freeze times) and lesion diameter in the 1-minute freeze conditions (Table 3). Comparison of the 1.5-minute −30°C and −50°C results revealed no significant difference in average lesion depth (p = 0.04) or serosal diameter (p = 0.9). This was hypothesized to be a result of the combination of reduced serosal surface heat load and innate insulative properties of ice resulting in attainment of maximal isotherm spread within the frozen mass in the −30°C and −50°C for the 1.5-minute freeze interval. Increasing the freeze time to 2 minutes using the −30°C protocol had minimal effect on lesion depth or diameter compared with the 1.5-minute −30°C and −50°C cohorts (p = 0.04 and p = 0.8, respectively), further supporting terminal isothermal spread for the −30°C protocol (Table 3).
Assessment of bladder integrity revealed no fistula development for any of the lesions (Fig. 2). This was attained without bladder drainage (Foley catheter placement) during recovery. US analysis (day 4) and gross pathologic assessment (day 7) of the kidneys revealed no damage or swelling. Urine output was found to return to normal by day 3 of recovery. Surrounding tissue analysis revealed no collateral damage even in cases wherein the abdominal wall and bowel were intentionally placed into contact with the bladder wall and frozen. This was done to determine the impact in the event adjacent tissues were inadvertently frozen.
Blood work revealed no deviations beyond normal ranges apart from elevated CK levels (Table 2). This was not unexpected as elevated CK levels are associated with muscle damage and effective full-thickness ablation results in bladder wall muscle damage. This combined with the ≥10 lesion sites within each animal are believed to be responsible for the elevated CK levels. Another important observation was the ability to create multiple lesions within a bladder without issue (Fig. 2).
This was seen even in several cases wherein ablation sites overlapped (e.g., double freeze) suggesting that multifocal tumors may be targeted with multiple freeze sites. Lastly, individual lesion analysis revealed the attainment of full-thickness ablation and no fistula development regardless of bladder wall thickness (range 2.5–14.1 mm) using the TC-TUCAB protocol.
Although promising, this study has several limitations. First, the study was limited to four subjects. Second, studies were conducted on healthy bladder tissue. Finally, tissue analysis was limited to H&E staining after 7 days survival. Future studies will focus on an expanded cohort, trichrome staining to examine extent of cell death within a lesion to confirm transmural destruction, in vivo tumor models and investigational device exemption clinical studies.
Conclusions
The results demonstrate that using the 6F Uroablate cryocatheter and temperature-controlled dose delivery method (TC-TUCAB), safe full-thickness bladder wall ablation can be attained using a standard cystoscopic approach in a warm saline-filled environment. Although promising, given the investigational nature of this study the extent of conclusions that can be drawn are limited and clinical corroboration is required.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank Ms. Janelle Schmidt (NAMSA-APS Senior Business Development Associate); Dr. Kadambari Shaker, MS, PhD (NAMSA-APS Study Director); and Ms. Olivia Prestrud (NAMSA-APS Study Coordinator); and the entire NAMSA-APS staff for their diligence and assistance in executing the in vivo studies.
Authors' Contributions
Conception: A.T.R., J.M.B., K.L.S., and K.K.S. performed study design. R.V.B., J.G.B., A.C., and A.K. provided review and feedback on study design. Performance of work: A.C., A.K., A.T.R., and J.M.B. performed all experimentation for this study. Interpretation or analysis of data: J.M.B., A.T.R., K.K.S., and K.L.S. conducted data analysis and interpretation. A.K., A.C., R.V.B., and J.G.B. reviewed and provided guidance and feedback on data analysis and interpretation. Writing the article: J.M.B. prepared the article. A.C., A.K., A.T.R., K.L.S., K.K.S., R.V.B., and J.G.B. provided revision input for the article. All authors read and approved the final article.
Availability of Data and Material
The data that support the findings of this study are available from CPSI Biotech but restrictions apply to the availability of these data, which were used under license for this study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of CPSI Biotech.
Author Disclosure Statement
Financial: A.T.R., J.M.B., K.L.S., K.K.S., and R.V.B. are employees of CPSI Biotech. Nonfinancial: J.G.B., A.K., and A.C. served in an advisory role to CPSI as collaborators on this project. J.M.B. and J.G.B. are related.
Funding Information
This study was supported in part by funding from the National Institutes of Health National Cancer Institute Grant No. 1R43CA210761-01A1 awarded to CPSI Biotech.