
Abstract
Background:
Following its introduction in 2018, the Single-Port (SP) robotic platform has been increasingly utilized for various approaches of robotic radical prostatectomy (RARP). Despite the demonstrable benefits in enhancing postoperative outcomes, there has been limited evidence on its perioperative morbidity, especially when compared to the gold-standard multiport (MP). This study sought to compare the perioperative morbidity between SP and MP-RARP.
Methods:
A retrospective review was performed on 911 patients who underwent RARP between January 2015 and May 2023. At our institution, SP-RARP has been performed since October 2018 with Extraperitoneal and Transvesical (TV) techniques. To reduce the risk of selection bias, only MP-RARP cases performed before October 2018 were included. Baseline clinicodemographic and perioperative parameters were collected. Perioperative complications were classified in accordance to the Clavien–Dindo system with postoperative complications and readmission reported within 90 days of surgery. Statistical analysis was performed with R Packages for Statistical Computing with descriptive statistics as presented.
Results:
Of the 484 SP and 322 MP-RARP cases included in our analysis, one intraoperative complication was reported, which pertained to a small enterotomy during TV SP-RARP. Postoperative complications were identified in 14.5% and 14.6% of SP and MP-RARP cases (p = 0.989), respectively. Major complication represents 4.1% of the SP and 3.4% of MP cohorts. The 90-day rates of hospital readmission following SP and MP-RARP were 5.6% and 4.9%, respectively (p = 0.717). Limitations of this study included the retrospective single surgeon, single institution nature of our series that also included the early learning curve experience associated with the novel SP platform.
Conclusion:
This comparative study provided evidence highlighting the low rates of perioperative complication and readmission following SP-RARP that were comparable to the Transperitoneal MP approach. The low morbidity associated with SP-RARP supports its wider application as an addition to the contemporary minimally invasive surgical armamentariums for prostate cancer.
Introduction
Robotic radical prostatectomy (RARP) has been increasingly utilized as the standard surgical treatment for localized clinically significant prostate cancer. With the continuing evolution of minimally invasive surgical techniques and with growing interest to push the boundaries toward improved perioperative and functional outcomes, recent years have seen the introduction of the novel purpose-built Single-Port (SP) robotic system (Intuitive Surgical, Sunnyvale, CA, USA), which allowed for the development of newer techniques that enriched the repertoire of surgical treatment options for prostate cancer. 1
In addition to its application for the more common Transperitoneal (TP) and Extraperitoneal (EP) techniques, the improved maneuverability with the double-articulating instruments of the SP platform provided the opportunity for urologists to regionalize RARP, such as with the advent of the Transvesical (TV) approach. 2,3 The benefits of the novel technique have been previously demonstrated, including its utility in facilitating same-day discharge, reducing postoperative opioid requirements, as well as in patients where conventional techniques may present some challenges, such as in those with previous abdominal surgeries or patients that may benefit more from regional anesthesia. 4,5 The latter can be facilitated as the direct intravesical access of the TV approach that no longer requires the steep Trendelenburg position that was otherwise required for other RARP approaches.
Despite the various advantages of SP-RARP, there remains a paucity of evidence surrounding the perioperative morbidity of the novel techniques, especially in comparison to the gold-standard multiport (MP) approach. Hence, the primary objective of this study was to describe the perioperative complications associated with two contemporary SP-RARP approaches, namely EP and TV, and to compare them with that of the TP MP technique.
Methods
A retrospective review was performed on the prospectively maintained Institutional Review Board-approved database to identify all patients that underwent RARP between January 2015 and May 2023. The primary objective of our study was to compare the perioperative morbidity associated with SP and MP-RARP. At our institution, SP-RARP has been performed since October 2018, with both SP EP and TV techniques can be safely used for various prostate cancer disease groups. Hence, for the purpose of our study and to reduce the risk of selection bias, only TP MP-RARP cases performed before October 2018 were included as a comparison in our analysis.
All procedures were performed by a single experienced robotic surgeon. The technique for TP MP-RARP has been described previously. 6 Both SP EP and TV cases were completed in a supine position using the DaVinci SP robotic platform based on the techniques first described by Kaouk et al. 2,7 and Ramos-Carpinteyro et al. 3 (Fig. 1). All double-articulating instruments, the endoscopic camera, and the Remotely Operated Suction Irrigation system (Vascular Technology Inc. [VTI], Nashua, NH, USA) were inserted through the multichannel cannula of the purpose-built SP Access Kit (Intuitive Surgical) that was placed via a single 3.5 cm incision. The placement of a surgical drain was based on the surgeon's preference or other intraoperative factors.
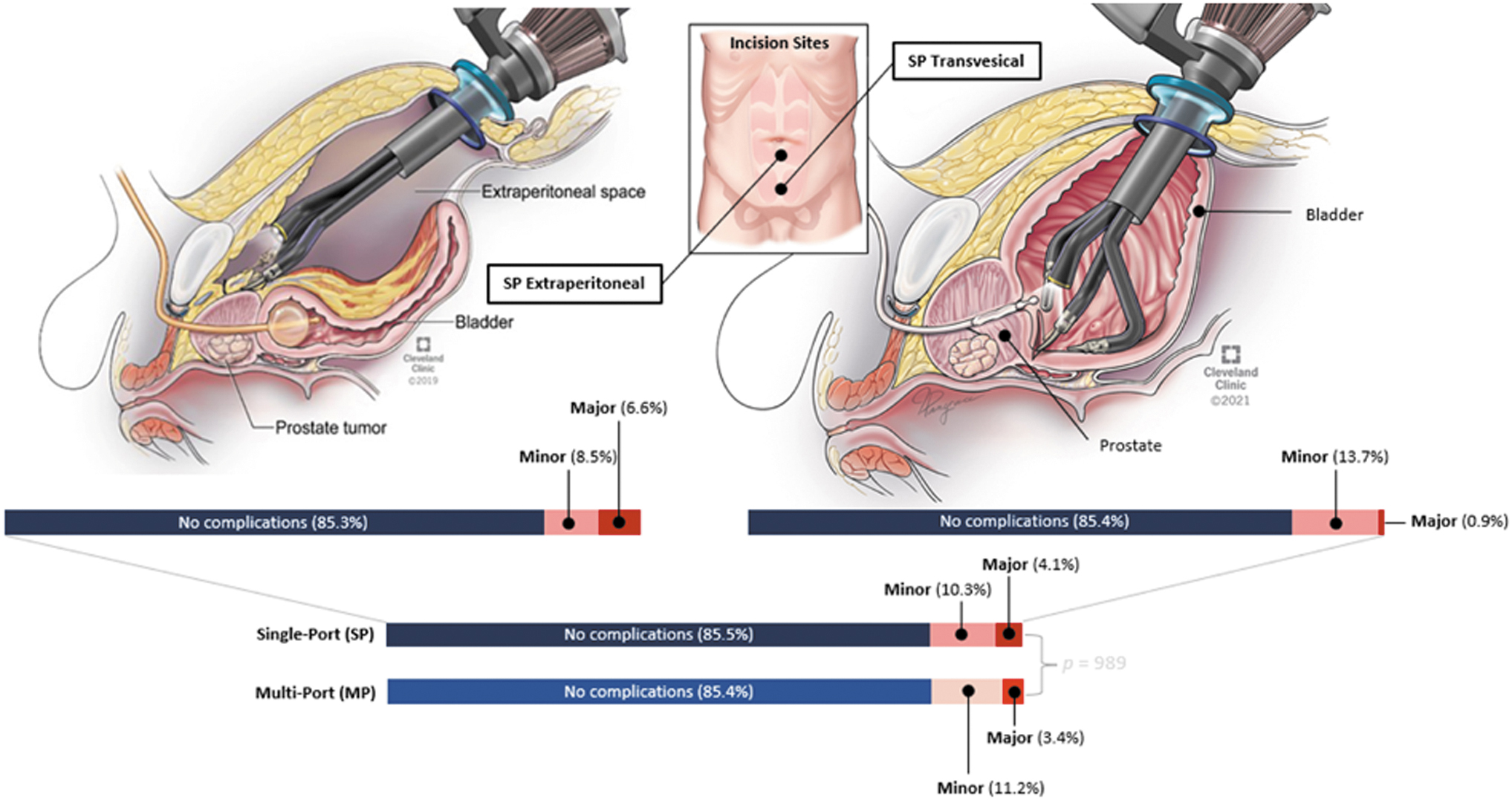
Postoperative complication profiles following SP and MP RARP. The SP cohort included both Extraperitoneal and Transvesical approaches, while MP-RARP was performed via a Transperitoneal approach. MP = multiport; RARP = robotic radical prostatectomy; SP = Single-Port.
Baseline variables collected include age, body mass index (BMI), history of previous abdominal surgery, American Society of Anesthesiologist score, Charlson Comorbidity Index score, as well as preoperative prostate volume, Prostate Specific Antigen (PSA) level, Gleason grade group of preoperative biopsy specimen, clinical T (cT) stage, and prostate cancer risk stratification according to the National Comprehensive Cancer Network (NCCN). 8 Risk of lymph node invasion was calculated based on the Briganti nomogram with patients scoring above 7% often referred for extended lymph node dissection (LND), most commonly pursued with the SP EP approach. Intraoperative parameters included total operating time, estimated blood loss (EBL), placement of additional port, surgical drain, as well as any evidence of intraoperative complications. Histopathology of the specimen was reported by our in-house pathology department in accordance with the American Joint Committee on Cancer TNM staging guidelines. Postoperative parameters reported in our study include length of inpatient stay, postoperative analgesia requirement, Foley catheter duration, as well as evidence of postoperative complication and hospital readmission within 90 days of the respective surgery. Postoperative complications were reported according to the Clavien–Dindo classification with major complications defined as those of Clavien–Dindo 3a and above. 9
Data were analyzed using R Packages for Statistical Computing version 1.3.1 (Vienna, Austria). Continuous variables were reported as the median and interquartile range. Categorical variables were reported as absolute and relative percent frequencies. Chi-square and t-tests were used for categorical and continuous variables, respectively, with a p-value of <0.05 considered statistically significant.
Results
A total of 806 patients were included in our analysis, which consisted of 484 and 322 patients who underwent SP and MP-RARP, respectively. The SP cohort consisted of 272 EP and 212 TV cases. A comparison of baseline demographic and clinical characteristics between the SP and MP cohorts, as well as between the two SP approaches were summarized in Table 1. Of note, patients who underwent SP-RARP were identified to be older (median, SP 63.9 vs MP 62.1, p ≤ 0.05), had higher preoperative PSA (median, SP 6.2 vs MP 5.6, p ≤ 0.05), and with a greater proportion of higher NCCN risk categories (Intermediate, SP 68.6% vs MP 66.8%; High–Very High, SP 17.6% vs 10.2%, p ≤ 0.05). In terms of other baseline disease characteristics, the two groups had similar distributions of cT stages (p = 0.156) and Gleason Grade Groups on preoperative biopsy specimens (p = 0.056). Despite not reaching statistical significance, history of previous abdominal surgery was more often encountered in the SP cohort (SP 40.3% vs MP 34%, p = 0.101). When comparing the two SP approaches, however, prior abdominal surgery was significantly more common in the TV group (EP SP 32.4% vs TV SP 50.5%, p ≤ 0.05).
Baseline Demographic and Clinical Characteristics of All Included Patients
ASA = American Society of Anesthesiologist; BMI = body mass index; CCI = Charlson Comorbidity Index; cT = Clinical T; EP = Extraperitoneal; IQR = interquartile range; MP = multiport; NCCN = National Comprehensive Cancer Network; PSA = prostate specific antigen; SP = Single-Port; TP, Transperitoneal; TV = Transvesical.
All cases were completed successfully without the need for conversion or additional ports. A summary of the perioperative outcomes and histopathology reports were presented in Table 2. SP-RARP was associated with significantly lower intraoperative EBL (median, SP 100 vs MP 200 mL, p ≤ 0.05), but with a longer total operating time (median, SP 194 vs 171 minutes, p ≤ 0.05). The placement of surgical drain was significantly less common in the SP cohort (SP 1.3% vs MP 99.1%, p ≤ 0.05). An intraoperative complication was identified in only one patient throughout our series, which represented 0.2% of all SP-RARP cases. The complication pertained to a small enterotomy during TV SP-RARP on a 69-year-old with multiple previous abdominal surgeries, including exploratory laparotomy, hemicolectomy, diverting loop ileostomy, and open appendectomy. The injury was closed with polydioxanone suture with the assistance of the General Surgical team, and the patient was discharged home on postoperative day 3 without any clinical sequelae.
Intraoperative, Postoperative, and Histopathology Outcomes Associated with the Different Single-Port and Multiport-Robotic Radical Prostatectomy Approaches Included in This Study
dHb = differences between preoperative and postoperative Hemoglobin levels; pN = Pathology N; pT = Pathology T.
We did not identify any differences in the 90-day rates of postoperative complications and readmissions between SP and MP-RARP (Postoperative complications, SP 14.5% vs MP 14.6%, p = 0.989; Readmission, SP 5.2% vs MP 5.3%, p = 0.988). Major complications were reported in 4.1% and 3.4% of the SP and MP cases, respectively (p = 0.717). Symptomatic lymphocele requiring percutaneous drainage (Clavien–Dindo 3a) was the most common major complication in the SP cohort (n = 16, 3.3%), with 94% of the cases reported following EP SP-RARP. Other major postoperative complications following SP-RARP included urine leaks requiring percutaneous drainage (n = 3, 0.6%) and return to the operating room for postoperative bleeding (n = 1, 0.2%). The latter was secondary to an inferior epigastric arterial injury during an EP SP-RARP for a 75-year-old with a previous history of herniorrhaphy with mesh. Intraoperative findings during the initial surgery included significant adhesion and the anterior abdominal mesh that was stuck to the bladder wall. The injury was promptly repaired using suture ligation on the same day, and the patient was discharged home without any complications on postoperative day 4.
Among the 11 patients who experienced major postoperative complications in the MP cohort, one patient presented with a supraumbilical incisional hernia 3 months postoperatively, measuring ∼4 cm. The patient was a 69-year-old with a previous history of open inguinal hernia repair as a child. He underwent a laparoscopic incisional hernia repair with mesh 6 months following his MP-RARP. In addition, one patient presented with a bilateral reducible inguinal hernia 3 months following his initial surgery. The patient was a 65-year-old man who did not have any history of previous abdominal surgery. Given the larger hernia on the right side that was also associated with intermittent discomfort, the patient proceeded with an open right inguinal hernia repair with mesh 5 months after his RARP. Thus far, we have yet to identify any case of ventral hernia following both EP and TV SP-RARP.
The three most common minor complications following SP-RARP included acute urinary retention (AUR) (n = 15, 3.1%), urinary tract infection (UTI) (n = 6, 1.2%), and ileus (n = 5, 1%). Of the 15 SP-RARP patients with AUR, eight were identified following the EP approach and seven presented following TV SP-RARP. In terms of minor complications following MP-RARP, urine leak for conservative management was the most common (n = 9, 2.3%), followed by UTI (n = 7, 1.8%), and ileus (n = 7, 1.8%). Venous thromboembolism was identified in 1.2% and 1% of the SP and MP patients, respectively. Despite most of the cases being managed with therapeutic pharmacological anticoagulation (Clavien–Dindo 2), two cases from the MP cohort were classified as major complications as one required percutaneous thrombectomy and the other necessitating placement of Inferior Vena Cava filter. A comprehensive description of the different postoperative complications and reasons for readmission were presented in Table 3.
Postoperative Complication and Readmission Within 90 Days Following Single-Port and Multiport-Robotic Radical Prostatectomy
AUR = acute urinary retention; Major Complications = Clavien–Dindo ≥3a; Minor Complications = Clavien–Dindo ≤2; UTI = urinary tract infection.
Discussion
Following Food and Drug Administration approval in 2018, different approaches of SP-RARP have been introduced including TP, EP, Retzius-sparing, Transperineal, and TV. The various benefits of the different approaches have been previously demonstrated, especially with the more regionalized TV approach providing the opportunity to facilitate outpatient-sparing outpatient RARP and for the procedure to be pursued in patients with a hostile abdomen and with a contraindication to general anesthesia. 3 –5,10 To our knowledge, this study represents the first large single-institution series that comprehensively described the perioperative complications associated with SP-RARP and compared them with the outcomes of the gold-standard TP MP-RARP.
Herein, we identified that the 90-day rates of postoperative complications of 14.5% and 12.9%, as well as the 90-day rates of hospital readmissions of 5.6% and 4.9%, were similarly low following SP and MP-RARP, respectively. The postoperative complication rates in our series were within the 2% to 30% range of postoperative complications following MP-RARP, as previously reported in a meta-analysis by Novara et al. 11 In addition, the rates of readmission in our series were also within the 3% to 18% range as reported in recent publications, with perioperative factors such as baseline comorbidities and LNDs demonstrated to increase the predisposition for hospital readmission. 12 –14
Of the different complications, we have identified a marked reduction in nonurological complications with SP-RARP (SP 2.9% vs MP 4.6%). When comparing the two SP approaches, the incidence of nonurological complications was lower in the TV cohort (EP 2.9% vs TV 2.4%). Among the nonurological complications, two cases of postoperative hernia were identified in our series, both following TP MP-RARP. These included one case of incisional hernia and one case of inguinal hernia. The absence of postoperative hernia in our SP-RARP series was important to appreciate, especially given the older age, equivocally overweight BMI, and the greater proportion of patients with a previous history of abdominal surgeries including herniorrhaphy, all of which have been previously demonstrated as risk factors for postoperative hernia. Furthermore, we have identified the previous history of hernia repair to be most prevalent in the TV SP-RARP cohort (26%), followed by EP SP-RARP (18%) and MP-RARP (11.6%). Despite the more prominent risk factors, the significantly reduced incidence of postoperative hernia can be likely attributed to the minimal disruption of the peritoneum with the more localized SP approach. 15 The importance of preserving the peritoneum was also evident in the reduced risk of postoperative ileus following SP-RARP (SP 2.9% vs MP 4.6%).
In our series, the risk of symptomatic lymphocele was the highest following EP SP-RARP (6.3%). All cases were reported in patients who underwent LND. Despite the higher incidence compared to the 0.5% and 1.3% rates following TV SP-RARP and MP-RARP, respectively, the risk of symptomatic lymphocele in our EP SP cohort remains lower than what was presented in previous studies, especially with up to 28.9% reported following EP MP-RARP. 16 –22 Several risk factors for the development of lymphoceles in RARP have been previously identified, including higher BMI, longer robotic console time, higher lymph node yield, and more aggressive tumors. 16,17 To help address this complication, we have proposed a technical modification to our EP SP-RARP approach by means of a small peritonotomy before the fascial closure at the end of the procedure. Following this modification, we have observed a substantial reduction in the incidence of symptomatic lymphocele from 8.7% to 2% in the most recent 100 cases.
This study was not devoid of limitations with the first pertaining to the descriptive, retrospective nature of this consecutive single-surgeon series that also included the early learning curve experience with the novel SP platform and techniques. Second, to reduce the risk of selection bias, we have intentionally excluded all MP cases performed after October 2018. Despite the resulting SP and MP groups having similar comorbidities, preoperative prostate volumes, and some baseline disease characteristics, there remain some differences, such as in terms of age, preoperative PSA, and NCCN risk categories in favor of the MP cohort. In addition, given the availability of at least two SP approaches to date, there were some differences, especially in the clinicodemographic characteristics between those who underwent EP and TV SP-RARP. Of note, the TV approach was initially offered for patients with smaller prostate glands below 80 grams and with lower-risk prostate cancer disease groups. The Briganti nomogram was routinely used to establish the need to pursue LND with those scoring above 7% referred for the procedure via an EP approach. Nevertheless, despite this initial selection criteria, technical refinements have seen the expansion of TV SP-RARP in a wider array of patients. The approach has since been completed in larger glands of up to 150 mL and in higher-grade disease, especially in those with a hostile abdomen. 23
Furthermore, given that the primary objective of this study was to compare the perioperative complications between SP and MP-RARP, detailed evaluations of oncological and functional outcomes following the different procedures were not pursued. Nevertheless, with regard to pathological outcomes, we identified an identical positive margin rate (PSM) between SP and MP-RARP of 26.5% and 25.7%, respectively (p = 0.877). A breakdown of the PSM according to the different pathological T stages was presented in Table 2. Of the cases with PSM, many represent focal involvements, which included 55%, 78%, and 65% in the EP SP, TV SP, and TP MP, respectively. In terms of functional outcomes, our earlier experience provided evidence highlighting the feasibility of an earlier Foley catheter removal on postoperative days 3 to 4 following the TV approach. Previous publications have also highlighted one of the benefits of the SP approach, with nearly 50% of patients who underwent TV SP-RARP achieving immediate continence. 3,24
Conclusion
SP-RARP is associated with a low 90-day risk of perioperative complications and hospital readmissions, which were comparable with the current TP MP technique. The regionalization of RARP with the TV approach, as facilitated by the novel purpose-built SP platform, offered a reduced risk of major and nonurological postoperative complications, such as ventral hernia and ileus. The results of this study provided evidence toward the safe utility of SP-RARP among the repertoire of minimally invasive surgical treatment options for prostate cancer.
Footnotes
Authors' Contributions
Conceptualization: N.A.S., J.K. Methodology: N.A.S., J.K. Data collection: N.A.S., J.S.C., R.R.C., C.D.M., A.M.P. Formal analysis: N.A.S. Writing–original draft: N.A.S. Writing–review and editing: N.A.S., J.S.C., R.R.C., C.D.M., A.M.P., J.K. Supervision: J.K.
Author Disclosure Statement
J.H.K.: Speaker for Intuitive; Consultants for VTI, MethodAI, and EndoQuest Robotics. Other authors have no conflict.
Funding Information
No funding was received for this project.