
Abstract
Introduction:
Diffusion of Innovation Theory explains how ideas or products gain momentum and diffuse (or spread) through specific populations or social systems over time. The theory analyzes primary influencers of the spread of new ideas, including the innovation itself, communication channels, time, and social systems.
Methods:
The current study reviewed published medical literature to identify studies and applications of artificial intelligence (AI) in endourology and used E.M. Rogers’ Diffusion of Innovation Theory to analyze the primary influencers of the adoption of AI in endourological care. The insights gained were triaged and prioritized into AI application-related action items or “tips” for facilitating the appropriate diffusion of the most valuable endourological innovations.
Results:
Published medical literature indicates that AI is still a research-based tool in endourology and is not widely used in clinical practice. The published studies have presented AI models and algorithms to assist with stone disease detection (n = 17), the prediction of management outcomes (n = 18), the optimization of operative procedures (n = 9), and the elucidation of stone disease chemistry and composition (n = 24). Five tips for facilitating appropriate adoption of endourological AI are: (1) Develop/prioritize training programs to establish the foundation for effective use; (2) create appropriate data infrastructure for implementation, including its maintenance and evolution over time; (3) deliver AI transparency to gain the trust of endourology stakeholders; (4) adopt innovations in the context of continuous quality improvement Plan-Do-Study-Act cycles as these approaches have proven track records for improving care quality; and (5) be realistic about what AI can/cannot currently do and document to establish the basis for shared understanding.
Conclusion:
Diffusion of Innovation Theory provides a framework for analyzing the influencers of the adoption of AI in endourological care. The five tips identified through this research may be used to facilitate appropriate diffusion of the most valuable endourological innovations.
Introduction
Adopting innovation and phasing out obsolete practices are fundamental drivers of high-quality healthcare. 1 Artificial intelligence (AI) is purported to revolutionize health care by enhancing clinical decision support and providing more personalized patient medical care. 2 Machine learning, a subfield of AI that enables computer learning without being explicitly programmed, 3 is especially effective when analyzing and integrating vast amounts and types of health care data (e.g., diagnostic images, electronic health record [EHR] data, and biomarkers). 4,5
By leveraging machine learning algorithms, AI can process and analyze vast amounts of endourological information, including physiological data, EHRs, three-dimensional (3D) images, radiology images, histological evaluation, endoscopic image recognition, genomic sequencing, and administrative and billing data. 6 Endourological clinical decision support systems, including systems that support diagnosis and enable personalized medical measurement and treatment, could improve the accuracy and efficiency of decision-making processes in endourology, ultimately leading to improved patient access, outcomes, and potential costs. 7 AI-based clinical decision support may be especially important in urology given increasing concerns regarding the urologic workforce shortage in the United States. 8,9 The shortage of urologists has resulted in longer wait times for appointments and surgeries, 10 causing delays in receiving care and potentially negatively impacting patient outcomes and quality of life. 11 The urologist workforce shortage is only expected to get worse in the coming years, 12 exacerbating service delivery pressures facing health systems.
The successful diffusion of AI technologies into endourological clinical practice will be influenced by many factors. The current study used Diffusion of Innovation Theory 13 to analyze some of the influencers that require consideration for the adoption of AI in endourological care. The Diffusion of Innovation framework has been primarily used to examine the diffusion of market-ready products over the past six decades. However, results from such an analysis can also be useful in evaluating emerging endourological AI innovations during the design-diffusion lifecycle.
Methods
Overview of diffusion of innovation theory
Diffusion of Innovation Theory, developed by E.M. Rogers in 1962, explains how an idea or product gains momentum and diffuses (or spreads) through a specific population or social system over time. 13 The theory seeks to elucidate the principal factors associated with the dissemination of the innovation, including the innovation itself, the communication channels, over time, and in the context of a social system (Fig. 1). 13,14
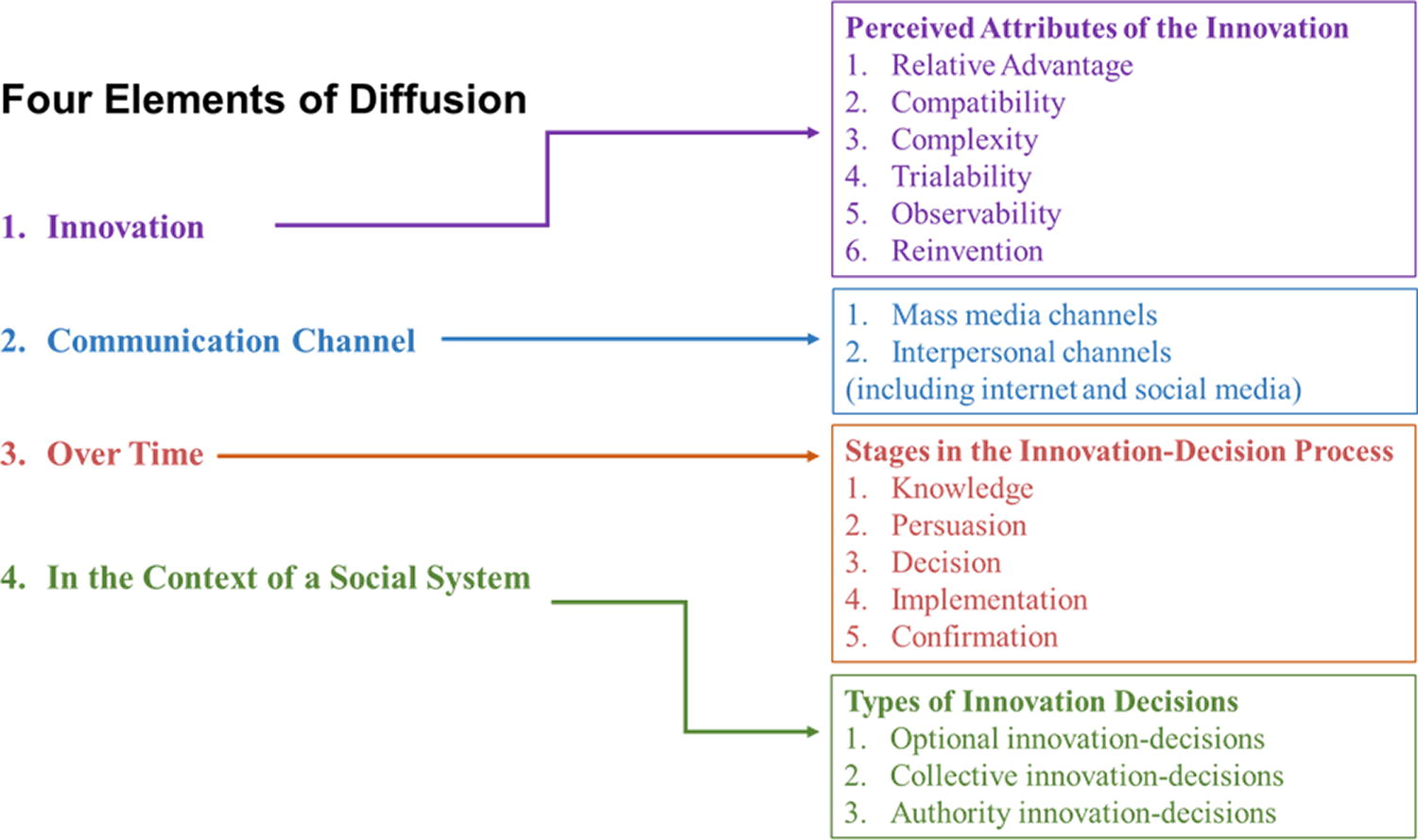
Four key components of Diffusion of Innovation Theory.
The innovation-diffusion process is described as “an uncertainty reduction process,” and five attributes of innovations help to decrease individuals’ perceptions of uncertainty and accelerate the rate of adoption of innovations: (1) relative advantage, (2) compatibility, (3) complexity, (4) trialability, and (5) observability. 14 Innovations with more favorable relative advantage, compatibility, simplicity, trialability, and observability will be more readily adopted. However, adoption of an innovation is challenging; therefore, the optimization of all of these attributes of an innovation facilitates and accelerates its uptake. The innovation-decision type (optional, collective, or authority), communication channels (mass media or interpersonal channels), social system (norms or network interconnectedness), and change agents may also increase the predictability of the rate of adoption of innovations. 14
Diffusion of Innovation Theory categorizes adopters based on their innovativeness, or their willingness to change familiar practices (Fig. 2). 13 Innovators are the gatekeepers who bring the innovation in and are willing to experience new ideas and accept more uncertainty. Their venturesomeness requires them to have passion and an affinity for the technical knowledge associated with the innovation. Early adopters often hold leadership roles in the social system, advising other members about the innovation and playing a central role at virtually every stage of the innovation process. 14 The early majority have good interactions with other members of the social system and are important in the innovation-diffusion process. 14 Economic necessity and peer pressure may lead late adopters to adoption. 14 Laggards hold a traditional view and are more skeptical about innovations and opinion leaders than the late majority.
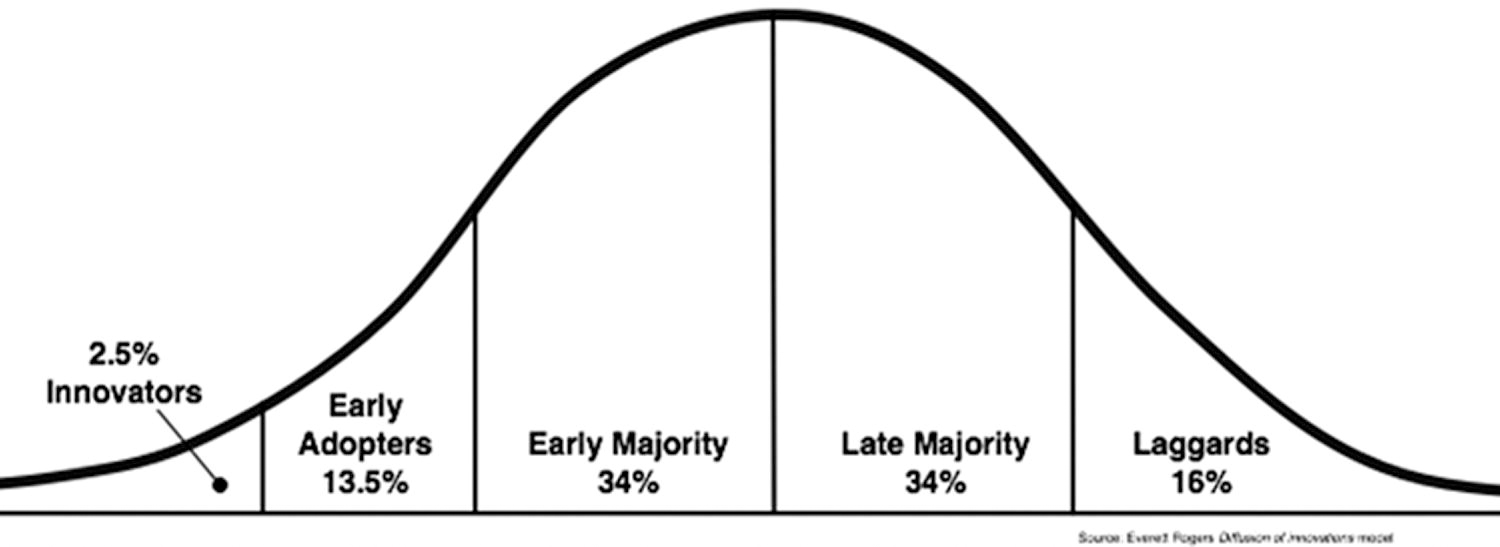
Adopter categorization based on innovativeness.
Identification of studies and applications of AI in endourology
The published medical literature was reviewed to identify existing studies and applications of AI in endourology. A search was carried out using the PubMed electronic database with the following search strategy: (“artificial intelligence” OR “machine learning”) AND (“endourology” OR “urology”). The search was limited to English-language publications. There were no restrictions on the dates of the published literature.
A total of eight published AI in endourology systematic literature reviews were used to gain an understanding of the current applications being evaluated or implemented in endourology. 15 –22 The results of these reviews were described in the context of Diffusion of Innovation Theory to better understand endourological technologies’ potential clinical decision support utility (i.e., where they are on their trajectories of dissemination and the enablers/barriers to delivering their promised goals) and to triage and prioritize AI application-related action items for facilitating appropriate diffusion of the most valuable endourological innovations. A literature review from the end search dates of the published reviews to the present day was conducted to identify any additional emerging applications of AI in endourology.
Results
Based on the published medical literature, AI is currently still a research-based tool in endourology; it is not widely used in clinical practice. 15,22 The eight reviews of published studies of AI in endourology described studies using AI models and algorithms intended to assist with the detection of stone disease (n = 17), the prediction of management outcomes (n = 18), the optimization of operative procedures (n = 9), and the elucidation of stone disease chemistry and composition (n = 24). The following sections use the components of Diffusion of Innovation Theory to illustrate the anticipated enablers and barriers for the adoption of AI innovations in endourology.
Perceived attributes of the innovation
Relative advantage
The degree to which an innovation is perceived as being better than the idea it supersedes is the relative advantage. 13 The effectiveness, cost, and social status motivation aspects of endourological innovations have been identified as important elements of relative advantage. 15 The innovation’s ability to support a differential diagnosis, treatment choice, pathology, surgical outcomes, and training outcomes will be important indicators of relative advantage. 15 –21 Analyses of cystoscopic images are an example in which AI applications can demonstrate relative advantages in object detection, image classification, and image segmentation. 18 Since cystoscopies are one of the most common endourologic procedures, the volume of cases combined with an existing repository of data make them an appropriate target for AI applications. 18 Preventive innovations often have a slower rate of adoption as there is more uncertainty regarding their relative advantage. However, incremental endourological AI innovations that replace existing devices and approaches as well as provide beneficial outcomes in a short period are likely to be more rapidly adopted. The consideration of justice, equity, diversity, and inclusiveness are essential factors in defining beneficial outcomes and relative advantage. 23
Compatibility
Compatibility reflects the ability of the innovation to match potential adopters’ current needs and circumstances. The applicability of endourological machine learning algorithms to patients from one site to other sites and to all groups of patients will determine their compatibility. 15 Another important aspect of compatibility for endourological AI innovations is whether sites have the data infrastructure required for implementation. 15,18,22 The absence of external validation was noted as a reason for the slower uptake of AI innovations that have demonstrated utility at a single endourological site. 15,17 –19,21 Finally, the impact of the innovation on workflow is an important compatibility consideration (e.g., need for additional space and special staff training and expertise).
Complexity
The excessive complexity of an AI endourological innovation is an important obstacle to its adoption. 15,22 For example, studies have been reported on the development of machine learning-based prediction models and identification of stone composition using deep learning convolutional neural network. 21 However, because of the complexity of the models, they are still not incorporated into routine clinical practice. 21 The additional demands on clinicians to implement clinical decision support using AI are yet to be determined, and both the burdens and gains associated with integration of AI need to be taken into consideration. 23
There are also applications in which AI innovations can help clinicians manage the complexity associated with effective endourological care (e.g., AI-assisted laser settings would facilitate adoption of new technology). Improved training that incorporates AI innovations supports better surgical skill development and surgical outcomes. 16,20,21 Applications of Virtual Reality, Augmented Reality, and Mixed Reality in endourology demonstrate the roles of simulation-based education in trainee preparation and subsequent patient outcomes. 16 AI applications in percutaneous nephrolithotomy (PCNL) are supporting safer implementation with better training along with others that are still at the nascent stages. 21
Trialability
Trialability reflects the ease with which the potential adopters may test or try the innovation. The more an innovation is tried, the faster its adoption. Earlier adopters are typically more likely to see trialability as an important aspect of the intervention. The trialability of endourological AI technologies is impacted by the availability of data infrastructure and the generalizability of the data to other sites. 15,16 Proprietary features of the endourological AI technology, including the costs associated with proprietary algorithms and the complexity of use in terms of agreements that need to be negotiated to even test them out, are also important considerations.
Observability
Observability describes the extent that the innovation’s impact is visible to other potential adopters. The training applications noted above reflect examples of observability. 16,20,21 It is important that adopters are able to see or observe the use of the innovation by others. 14
Communication channels
The paths through which opinion leaders and others communicate about an innovation are communication channels. The internet and social media are the most important communication channels of the modern era. Medical journals and professional conferences also play a role in interpersonal channels for near peers who have worked with endourological AI.
Time and stages in the Innovation-Diffusion process
The knowledge stage
During the knowledge stage, adopters learn about the innovation’s existence and gain knowledge about the innovation. 14 According to Rogers, three types of knowledge are gained: (1) awareness-knowledge, (2) how-to-knowledge, and (3) principles-knowledge. 13
Awareness-knowledge
Awareness-knowledge is when the individual is aware of and familiar with the existence of the innovation. 13 Awareness-knowledge encourages the potential adopter to increase their how-to- and principles-knowledge concerning the innovation. The existence of the systematic literature reviews summarized in this article suggests that awareness-knowledge has been established; however, the specifics linked to the other types of knowledge are not as well understood.
How-to-knowledge
Even individuals who have technical backgrounds may not use the technology if they do not have knowledge of how to use it correctly. 14,24 How-to-knowledge is especially important for complex interventions such as the more hidden predictive analytics-based applications. For the more visible training-related applications, the providers of the technologies and the educators need to ensure that the training needs are adequately assessed, competencies measured, and value to patient outcomes demonstrated. 16,20,21
Principles-knowledge
The biggest barrier to use the technology may be a lack of vision of why or how to integrate the technology. 25,26 Successes with the implementation of the Triple Aim and the Quadruple Aim have demonstrated the importance of sharing “know-why” experiences at the knowledge stage. 27 –29 The importance of ensuring equity in the deployment of AI innovations 23 is an important component of the principles-knowledge.
The persuasion stage
The persuasion step pertains to adopters’ formulation of their opinions and beliefs about an innovation. Opinions and beliefs about the innovation may change; a negative attitude may be converted to a positive attitude and vice versa. A positive initial experience with the first use of a new endourological AI technology would be important for persuasion. The certainty of the innovation’s value and social reinforcement from other adopters would also affect opinions and beliefs. 14 For example, AI-based data collected during robotic-assisted surgical training that has improved assessment of surgical skills 18 can be persuasive in demonstrating the value of integrating AI in robotic-assisted surgical applications. Truly valuable “use cases” that have been replicated at multiple sites will be a key factor in persuasion. 15,17,19,21 AI has shown promising results in studying the complicated intraoperative environment to optimize and guide surgeons’ preferences and strategy in extracorporeal shockwave lithotripsy (ESWL), PCNL, and retrograde intrarenal surgery. 17 Collective or authority adoption (e.g., incorporation of AI-based tools into endourological practice guidelines) and market pressures (e.g., loss of market share drove physicians/hospitals to adapt and adopt robotic prostatectomy) will also be notable persuasion factors.
The decision stage
Adoption or rejection of the innovation occurs at the decision stage. AI applications that improve accuracy and diagnosis of urinary stones, selection of treatment, and patient outcomes accordingly 19,20 will be more likely to be adopted in clinical decision support for endourological care. Operational workflows may change with AI implementation, and the planning for these workflow changes and their cost-benefit impact will need to be considered by hospital administrators and other decision makers.
The implementation stage
Implementation of the innovation may be challenged if there is still uncertainty regarding the innovation’s value. Change agents and opinion leaders may help reduce uncertainty at this stage. The Plan-Do-Study-Act (PDSA) cycles of continuous quality improvement (CQI) best practices are examples of how uncertainty can be reduced at the implementation stage 30 and have shown success in guiding improvement processes in real-world settings, particularly in other disease management. 31 The innovation-decision process will end, since “the innovation loses its distinctive quality as the separate identity of the new idea disappears.”
At the implementation phase, the innovation may be “reinvented”—changed and modified to facilitate adoption and institutionalization. 13 Computer-based innovations enable many possible opportunities and applications, and hence are more open to reinvention, 14 including customization of AI innovations to a specific local application.
The confirmation stage
Adopters look for support of their decision at the confirmation stage. 14 It is possible that the decision will be reversed at this stage, depending on the support for adoption of the innovation and the attitude of the individual. 14 Two types of discontinuance may occur: replacement discontinuance, where the individual rejects the innovation to adopt a better innovation, or disenchantment discontinuance, where the innovation is rejected because of dissatisfaction with its performance, potentially because of premature adoption or because of it not meeting their needs. 14
Social system
The diffusion of innovations takes place in the social system, defined by Rogers as a set of interrelated units engaged in joint problem solving to accomplish a common goal. 13 The US Food and Drug Administration recognizes the increased use of AI across a range of therapeutic areas. 32 The Agency for Healthcare Research Quality’s Digital Healthcare Research Program’s mission is to determine how the various components of the ever-evolving digital healthcare ecosystem can best come together to positively affect healthcare delivery and create value for patients and their families. 33 A shift in the clinical care paradigm will be evident as AI applications are incorporated in the practice guidelines and they become part of the standard of endourological care. 15 It is important that the adoption of endourological AI technologies does not increase existing inequities in our healthcare system; appropriate deployment of endourological AI technologies should work toward decreasing existing inequities. Inequality of healthcare services may widen with initial adoption and refinement of AI by academic medical centers and specific private medical facilities before the cost of AI can be reduced and be adopted later by others outside of these practices.
Discussion
The current study reviewed published medical literature to identify studies and applications of AI in endourology and used E.M. Rogers’ Diffusion of Innovation Theory 13 to analyze primary influencers of the adoption of AI in endourological care. Based on the published medical literature, study findings showed that AI is currently still a research-based tool in endourology; it is not widely used in clinical practice. Most publications focused on diagnostic tools and prediction of outcomes after clinical interventions. Diffusion of Innovation Theory has primarily been used to examine market-ready products’ diffusion. However, results from this analysis have proven useful in evaluating emerging endourological AI innovations during the design-diffusion lifecycle.
Although AI is currently still mostly a research-based tool in endourology, it has the potential to eventually revolutionize stone disease care. AI-driven treatment strategies hold great promise for the future and AI is an essential step forward in providing improved shared decision making and more precise personalized patient care, particularly in selecting treatment modalities. One may envision the path of the future that a patient with stone disease may take … At home, the patient enters their symptoms and family history. AI directs them to the possibility of kidney stones and advises them to present to the emergency room (ER) if the pain is moderate to severe or to urgent care if the pain is mild. Ultrasound, urinalysis, and computed tomography (CT) are ordered. AI interprets the test results and schedules an appointment for the patient in 1–2 weeks if there is no hydronephrosis or if the stone size is <4 mm. Otherwise, AI interprets the CT imaging to predict and optimize evidence-based outcomes for observation, ESWL, ureteroscopy, or PCNL. AI incorporates patients’ preferences (i.e., pain vs. success vs. risk) to recommend the “best” procedure. AI also interprets any emerging postoperative symptoms as stent-related vs. potential infection. Complicated intraoperative decision making and optimization of laser settings based on prediction of stone composition on endoscopy viewing will be facilitated with AI. AI will also enhance surgical training with the aid of Virtual Reality, Augmented Reality, and Mixed Reality. 16
The most pertinent insights gained from the literature review of endourological AI may be summarized as five tips for facilitating appropriate adoption of endourological AI; they are: (1) Develop and prioritize training programs to establish the foundation for effective use, (2) create the appropriate data infrastructure for implementation, including its maintenance and evolution over time because it is a prerequisite for successful AI-applications, (3) deliver AI transparency to gain the trust of endourology stakeholders, (4) adopt innovations in the context of CQI PDSA cycles because these approaches have proven track records for providing improvements in the quality of care, and (5) be realistic about what AI can and cannot do at this time and document that realism to establish the basis for shared understanding among stakeholders.
While it holds tremendous promise, AI could add yet another layer of complexity to the practice of endourology. Stress and burnout among urologists is a significant concern as it has been linked to decreased job performance, increased medical errors, interpersonal conflicts, and depression. 34 Some research even suggests that urologists have higher rates of burnout compared with physicians in other specialties. 35 AI innovations that help clinicians manage the complexity associated with effective endourological care will be well received. Following this first tip may potentially convert “late majorities” that initially avoided AI-based innovations because of feeling uncomfortable with its use. Providers of the technologies and the educators need to ensure that the training needs are adequately assessed, competencies measured, and value to patient outcomes demonstrated if the promise of AI in endourological care is to be realized. 16,20,21 Training tailored to the learning needs and styles of urologist physicians and residents is needed to establish the foundation for effective use of endourological AI.
Data infrastructure is an important influencer for the adoption of endourological AI innovations. 15,18,22 AI requires a continuous supply of high-quality data. Data quality issues may entail accuracy, completeness, consistency, timeliness, integrity, relevance, data collection, preprocessing, management, data governance, and data labeling. 36 Storage challenges, processing challenges, data management challenges, data heterogeneity, data privacy and security, bias and representativeness, and data access are also data quality considerations. 36 Hameed and colleagues (2021) 15 hypothesized that data infrastructure may be a main reason for the absence of use of AI in endourological clinical practice. Hence, implementation of this second tip could prevent subsequent abandonment of AI applications because of disappointments related to their value because the data were lacking. Accessibility of large databases to developers of AI is also essential for helping develop and refine algorithms and for faster adoption. It will be critical to ensure data sharing is conducted ethically with adherence to information protection laws to gain trust in data sharing to drive a better end product to also support the adoption.
AI models can be difficult to interpret and explain, which can make it difficult for stakeholders to understand how decisions are made. 22,36 It is important to ensure that AI models are transparent and explainable to gain and maintain the trust of healthcare professionals, patients, and other decision-makers. An understanding of machine learning and deep learning methods should be attainable for audiences without extensive technical computer programming background. 37 The ability for critical appraisals by urologists is the keystone to validating theoretical models and designing prospective studies for the benefits of AI to be realized in clinical practice. 22 Ethical considerations call for AI systems to adhere to the principles of fairness and nondiscrimination. 38 Advances in modern medicine are sometimes stymied by the inability to translate evidence-based care to all patients. 23 Transparency of AI models, the focus of the third tip, is essential to be able to evaluate and ensure their relevance for diverse populations and the ability to translate the innovations to all settings of care.
The fourth tip is based on the multi-decade-proven experiences of implementing positive change using CQI methods. Adopting innovations in the context of PDSA cycles of CQI best practices 30 would reduce uncertainty about the consequences of the implementation of an endourological AI technology and uncover factors that might not have been evident at the onset. The key to any CQI initiative is using a structured planning approach to evaluate the current practice processes and to improve systems and processes to achieve the desired outcome and vision for the desired future state. 30 CQI principles, strategies, and techniques are critical drivers of new care models and of high-quality healthcare. Rogers found that reinvention, the degree to which an innovation is changed or modified by a user, was an important part of an innovation’s implementation as the more reinvention took place, the more rapidly the innovation was adopted and became institutionalized. 13 PDSA cycles are demonstrated ways of adapting the implementation of new processes and capabilities to the specific circumstances of an organization and have shown success in quality improvement in other disease management.
Finally, it is important that researchers and implementers of endourological AI technologies are realistic about what AI can and cannot do at this time. This fifth tip is about reducing the hype and assuring that hopes are achieved. The future of endourological AI includes many predictions and promises, but building upon foundations of realism and acknowledging that there are challenges to overcome are essential for actually improving clinical outcomes and patient care. The capabilities as well as the limitations of endourological AI technologies should be evaluated and documented for shared understanding.
One strength of this research is that, to our knowledge, this is the first study using Diffusion of Innovation Theory to analyze the primary influencers of the adoption of AI in urological care. Discerning common themes applicable across AI applications into tips for effective use is intended to support innovation that benefits patients and empowers clinicians. Limitations of this research include that published medical literature was relied upon for understanding the availability and utilization of urological AI innovations. It is expected that proprietary AI technologies are being developed and that there is a lag in their presentation and availability in the scientific literature. Each AI-based innovation can also be analyzed with the Diffusion of Innovation Theory so that specifics to each can be considered given its place in the design-development lifecycle.
Conclusion
Endourology is well suited for AI given the rich visual information and data available. The reviews highlighted ways that AI is striving to help us enhance our understanding of very complex urological systems through stone disease detection, prediction of treatment outcomes with different choices, optimization of operative procedures, and elucidation of stone disease chemistry and composition. AI clinical decision support systems have the potential to improve the accuracy and efficiency of decision-making processes in endourology, ultimately leading to improved patient access, equity, outcomes, and costs. Diffusion of Innovation Theory provided a framework for analyzing the influencers of the adoption of AI in endourological care. The five tips identified through this research offer a way to facilitate appropriate diffusion of the most valuable endourological innovations.
Footnotes
Authors’ Contributions
M.M., E.T., J.W., and S.B.: study design, data interpretation, and article editing; N.E. and S.R.: study design, implementation of data analysis, data interpretation, and article writing and editing.
Author Disclosure Statement
N.E. is a health services research consultant paid by Boston Scientific. S.R., E.T., J.W., and S.B. are employees of Boston Scientific. M.M. was not compensated for his participation in this study.
Funding Information
This work was supported by Boston Scientific.