
Abstract
Acute kidney injury (AKI) constitutes a significant public health concern, with limited therapeutic options to mitigate injury or expedite recovery. A novel therapeutic approach, local renal treatment, encompassing pharmacotherapy and surgical interventions, has exhibited positive outcomes in AKI management. Peri-renal administration, employing various delivery routes, such as the renal artery, intrarenal, and subcapsular sites, has demonstrated superiority over peripheral intravenous infusion. This review evaluates different drug delivery methods, analyzing their benefits and limitations, and proposes potential improvements. Renal decapsulation, particularly with the availability of minimally invasive techniques, emerges as an effective procedure warranting renewed consideration for AKI treatment. The potential synergistic effects of combined drug delivery and renal decapsulation could further advance AKI therapies. Clinical studies have already begun to leverage the benefits of local renal treatments, and with ongoing technological advancements, these modalities are expected to increasingly outperform systemic intravenous therapy.
Introduction
Acute kidney injury (AKI) is a common clinical syndrome characterized by a sudden increase in serum creatinine, a decrease in urine output, or both. It is caused by various factors, including renal ischemia, sepsis, drug toxicity, and damage due to myoglobin or hemoglobin. 1,2 AKI is a significant global public health problem; ∼13.3 million people worldwide develop AKI annually, and the number is increasing. 1,3 However, there are few treatments for AKI, with the current approach relying only on dialysis to limit the damage or accelerate recovery. Impaired repair during AKI can lead to a decline in the renal reserve capacity and promote progression to chronic kidney disease and end-stage renal disease, which should be avoided as far as possible. 4 –6 There are already some drugs that can reduce kidney injury or even promote kidney regeneration and repair that have been found by researchers, such as stem cells and their exosomes, which is hotspot of AKI therapeutic drug research, to enhance its efficacy and reduce its side effects, and it is often used in the way of local drug delivery. The system of local renal treatment is thus continuously developing and enriching its content.
Current renal-targeted interventions for AKI can be broadly categorized into two principal approaches: perirenal drug administration and regional surgical treatment. Recent literature has increasingly highlighted the potential benefits of perirenal drug administration, with research delving into various administration pathways, including through the renal artery, intrarenal, subcapsular, renal vein, and renal pelvis. Such localized delivery methods offer numerous advantages over traditional peripheral intravenous administration, such as enhanced renal drug concentration, prolonged drug metabolism within the kidney, reduced risk of embolism, and decreased immunogenicity. 7 The technique of renal decapsulation in the management of AKI, which involves the surgical removal of the renal capsule to alleviate pressure on the renal surface, has been historically underutilized. However, it has been long neglected because the benefits of open surgery are not commensurate with the trauma involved. 8,9 Nevertheless, in light of its potential therapeutic role in certain severe and prognostically unfavorable cases of AKI, the reevaluation of renal decapsulation is warranted. 10 –13
Renal local therapy for AKI has yet to establish a comprehensive framework. In this review, we discuss the current state of research on AKI's local treatment and prospective avenues for future research.
Current State of Localized Treatments for AKI
To date, a considerable body of literature has corroborated the enhanced efficacy of perirenal administration of AKI therapeutics compared with systemic intravenous delivery, as summarized in Table 1. Although the surgical techniques employed in animal experimentation present challenges for patient acceptability, the potential benefits of perirenal drug administration—namely enhanced efficacy and reduced systemic side effects—persist in garnering the interest of researchers to pursue further investigations. The surgical management of AKI is less frequently discussed despite its longstanding history, which predates the advent of perirenal administration. Recent years have witnessed a reevaluation of its effectiveness in treating AKI. Unfortunately, the focus on local renal treatments has predominantly been on the development of technical innovations, with a corresponding dearth of research into the detailed mechanisms underlying their therapeutic effects. In this review, we delve into the latest progress in the exploration of renal perianatomical architecture and function, advancements in targeted renal drug delivery systems, and the refinement of surgical interventions for the kidneys.
Summary of Arterial Administration
Ad-sh = shRNA expression adenovirus; AKI = acute kidney injury; bFGF = basic fibroblast growth factor; CKD = chronic kidney disease; circPTPN 14 = circular RNA PTPN14; EGF = murine epidermal growth factor; eNOS = endothelial nitric oxide synthase; HSP90 = heat Shock Protein 90; HGF-PMCS = hepatocyte growth factor-reducing mesothelial cell sheets; IL = interleukin; IR = ischemia–reperfusion; KLF4 = Krüppel-like factor 4; YAP = yes-associated protein; MetS = metabolic syndrome; MSCs-ex = mesenchymal stem cell-derived exosomes; PKCα = a member of protein kinase C; RAS = renal artery stenosis; TGF-β1 = a member of the transforming growth factor beta; UUO = unilateral ureteral obstruction.
Renal anatomy and its implications for localized treatment
The kidney is nestled amidst critical anatomical entities, such as the renal artery, renal vein, ureter, and the encapsulating renal capsule. This organ is shrouded by a tripartite sheath comprising the renal fibrous capsule (RFC), perirenal fat (PeRF), and the renal fascia. These layers coalesce to form the renal capsule, a composite multilayered structure interspersed with adipose tissue and potential spaces. A thorough grasp of the anatomy and physiology of these perirenal components is pivotal to driving forward the field of local treatment research.
The RFC
The RFC, sometimes called the renal capsule, is a thin, tough, dense layer of elastic fibers. Covering the entire kidney, the RFC folds and terminates in the renal sinus, directly connecting the PeRF and renal cortex. 14 The RFC is easily separated from the renal parenchyma because of the smooth renal surface, so subcapsular injection is possible. The renal capsular vein runs underneath the RFC along the renal surface and extends to the renal hilar fat vein, which together with the peritubular capillaries forms the initial part of the cortical venous drainage system. 14,15 The subcapsular space is also an ideal graft environment for cell or tissue transplantation because it is suitable for cell or tissue growth. 16 –18 Moreover, due to the volume restriction created by the RFC, it becomes a critical factor in the volume/pressure relationship of the kidney. 19 –21 In AKI, renal tubular dilatation and inflammatory edema can cause a significant pressure increase within the RFC, further compromising renal function. 10 The conducive milieu beneath the renal capsule, coupled with the capsule's impact on renal function, has spurred the development of subcapsular drug delivery and renal decapsulation techniques.
The PeRF
The PeRF, also called the renal fat capsule, is fat tissue surrounded by a fibrous membrane that envelops the kidney and adrenal gland. 22,23 The edge and lower pole of the PeRF are thicker than other parts, and the average thickness of the PeRF of an adult is around 2 cm, which protects the kidney. 24 The PeRF is located within the renal fascia, whereas the pararenal fat is located on the surface of the renal fascia; the two should be distinguished, with the PeRF being more closely associated with the kidney. The PeRF consists primarily of neutral fat, which is composed of white adipose tissue and islands of brown adipose tissue. 25,26 It is organ-like, with an intact blood supply, lymphatic drainage, and innervation system. 27 –29 Regrettably, the vascular supply within the PeRF appears to be autonomous or does not directly perfuse the renal parenchyma. This suggests that pharmacological agents introduced into the PeRF may not achieve localized enrichment within the kidney. However, this hypothesis necessitates further empirical validation. 14,30,31 The lymphatic vessels in the PeRF have many anastomoses with the intrarenal lymphatic vessels, which merge with the intrarenal lymphatic vessels at the hilum and eventually drain into the paraaortic lymph nodes. 32 –35
The PeRF is innervated by sympathetic fibers of the autonomic nervous system. Heightened activation of these efferent nerves within the PeRF has been implicated as a significant contributor to sustained hypertension. Consequently, when considering drug administration to this region, meticulous attention to the potential neurological impacts is warranted. 36 At the same time, recent studies suggest that the RFC is a potential source of mesenchymal stem cells (MSCs), so preservation of this layer is recommended to improve the recovery process. 37,38
The renal fascia
The renal fascia is the outermost membrane of the kidney and is a specialized extraperitoneal tissue structure. The renal fascia is continuous with the subdiaphragmatic, iliac, and transversalis fasciae, which encompass the kidney, PeRF, ipsilateral ureter, adrenal gland, and gonadal blood vessels. 39,40 The renal fascia is a multilayered fibrous membrane that supports and protects the kidney; it wraps tightly around the PeRF, exerts some pressure on the kidney, and is connected to the RFC by fibrous bundles that help to hold the kidney in place. 14 As the importance of the renal capsule in facilitating renal recovery has been recognized recently, promising routes for local drug delivery have been developed (Fig. 1).

Regional anatomy around the kidney: AG = adrenal gland; CLV = communicating lymphatic vessels; GV = gonadal vein; ISA = inferior suprarenal artery; LA = lumbar artery; LCA = left colic artery; PaLN = para-aortic lymph nodes; PaRF = pararenal fat; PeRF = perirenal fat; PLV = perirenal lymphatic vessels; RA = renal artery; RCV = renal capsule vein; RF = renal fascia; RFC = renal fibrous capsule; SLV&ILV = subcapsular and interenal lymphatic vessels; TA/OA = testicular/ovarian artery.
Status of local drug delivery in AKI
Arterial administration
With advances in modern interventional radiology, renal artery access has become feasible (Figs. 2 and 3). 41 Drug delivery through this artery offers several advantages over peripheral intravenous injection, such as reduced systemic side effects, increased accumulation at the target organ, avoidance of clearance by the reticuloendothelial system, and reduced pulmonary retention, such that the trapping of a large proportion of cells in the pulmonary microvessels can be avoided. 42 –47 A drug is distributed evenly throughout the kidney following the blood flow of the renal artery, and when MSCs are injected, they can also be implanted locally and remain in the kidney for some time. 48 Many studies have adopted arterial administration to deliver chemical compounds, genes, and cells or their derivatives (Table 1). Renal artery injection has shown good delivery performance in animal studies and no significant handling-related complications have been reported. The clinical safety and acceptability of this method have been confirmed in phase I 49 and II 50 clinical trials.

Local renal treatment: a new combined treatment for acute kidney injury.
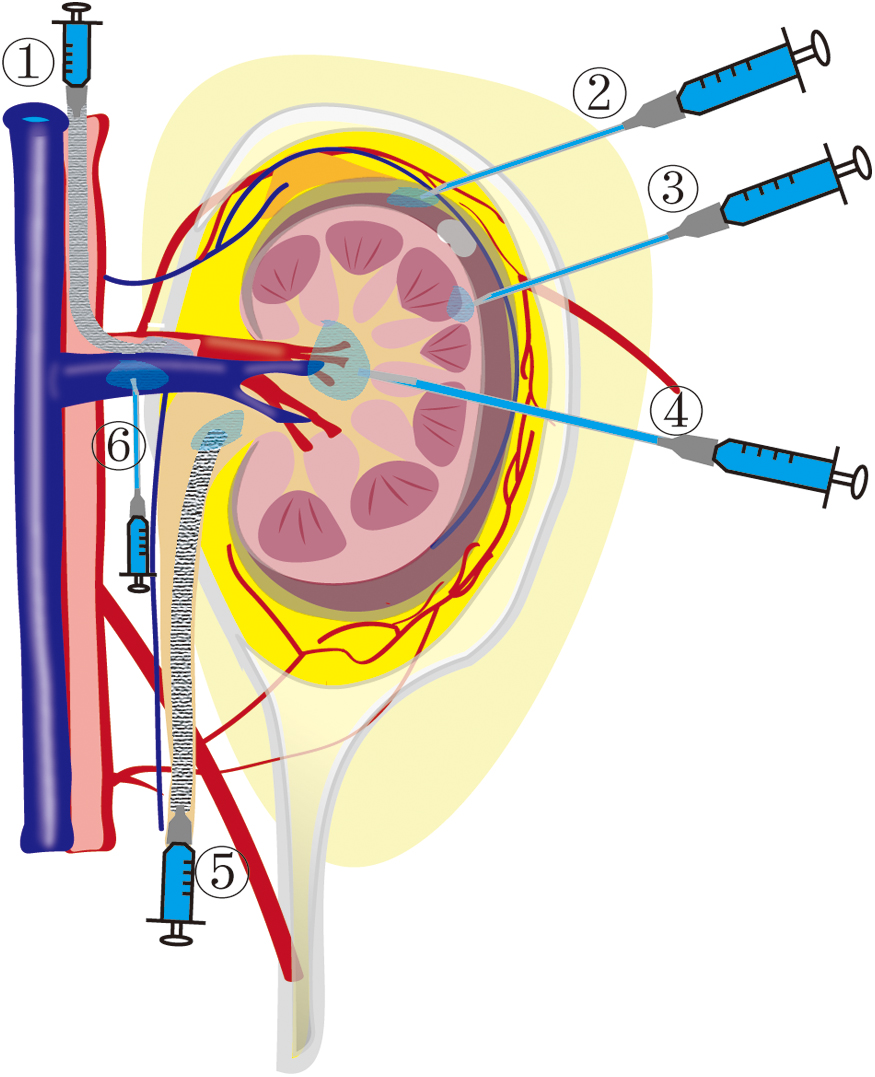
Different routes of topical renal administration: through ①, the artery; ②, the renal subcapsular; ③, the parenchyma or subcortical; ④, the renal pelvis injection through parenchyma; ⑤, the renal pelvis injection through the ureter; ⑥, the renal vain.
The intra-arterial injection technique offers a prospective pathway for clinical application; however, the risks associated with the procedural aspects and the side effects due to potential overdosage warrant careful consideration. 51
Parenchymal or subcortical administration
Parenchymal or subcortical administration, referred to as intrarenal injection, is a method for directly diffusing a drug around the injection site. This approach is highly feasible, causes some reversible kidney damage, and is a common method of drug delivery in animal studies (Table 1). The rapid blood flow in the renal artery allows a drug or cells to remain only for a short time after injection, and intrarenal injection can overcome this disadvantage. However, the uniformity of drug distribution with intrarenal injection is inferior to renal artery injection and they provide therapeutic effects only near the injection site. Intrarenal injection has several major disadvantages, including risks of bleeding, renal injury, and procedure-related complications. Even with laparoscopy, this route of administration has been associated with more procedure-related complications in clinical trials, although the relevance and cause have not been conclusively demonstrated. 52
In addition, current animal studies often use multiple injections to achieve a more even distribution of therapeutic agents throughout the kidney, which increases the risk of complications. This suggests that promoting intrarenal injection in clinical practice is challenging unless we can develop a less invasive injection tool.
Renal subcapsular administration
Renal subcapsular administration is an innovative method that has been proposed recently; its unique advantages in the treatment of AKI have attracted increasing attention. The RFC and renal cortex are easily separated due to the potential space below the RFC and the smooth surface of the kidney. The space beneath the RFC is suitable for cell or tissue transplantation and the grafts do not trigger a significant immune response. 16 –18,53,54 It is even an ideal culture site to maintain the intrinsic properties of stem cells and provide adequate nutrients for cell growth. 55 Based on its anatomy, a drug injected under the RFC can directly contact the cortex, and the renal capsular vein can also help drugs penetrate the renal parenchyma. 15 It is an effective delivery route and can reduce the renal inflammatory response, promote cell proliferation, and improve renal repair (Table 1). However, few clinical studies have examined renal subcapsular administration because the space is relatively narrow and difficult to accurately locate without open surgery.
Recognizing the subcapsular space accurately and safely under ultrasound guidance is a worthwhile endeavor, and establishment of the subcapsular drug delivery route will provide new options for the emergency treatment of AKI.
Comparison of different administration routes
There is currently great interest in the use of MSC-based therapies as a strategy to improve efficacy. MSC exerts its therapeutic effects through multiple mechanisms, including paracrine signaling, immune regulation, and in situ colonization. 56 –59 Several studies have also used MSCs to treat AKI, making it easier to compare different administration routes.
Studies have shown that when MSCs are infused through a peripheral vein, >60% of the cells accumulate in the lungs, while <7% are able to function in the kidneys. 60 This suggests that for MSC therapy, the local application of MSCs will significantly increase efficacy. A meta-analysis of 21 studies using MSCs to treat AKI showed that both transarterial and intrarenal injection of MSCs had better therapeutic effects than peripheral intravenous injection. 61 Transarterial injection was more efficacious than intrarenal injection because MSCs remain around the injection site after intrarenal injection, whereas MSCs follow the rich blood flow throughout the kidney. 62
Compared with parenchymal administration, administration through the RFC has a better therapeutic effect because the graft under the RFC has a larger coverage area. 63 In addition, RFC has a higher renal implantation rate, longer cell retention time, and lower risk of embolization than renal artery administration. Thus, the advantages of renal subcapsular administration make its worthy of further research so that it can be used more safely and is more clinically acceptable (Fig. 4).

Comparison between different routes of topical administration.
Advances in local surgical interventions for AKI
Historical application of surgery in AKI
No surgery was available for AKI until renal decapsulation was proposed around the beginning of the 20th century, before dialysis became widely available. 8,9 The purpose of renal decapsulation is to relieve the pressure on the kidney surface by opening the RFC, thereby promoting renal recovery. Renal decapsulation was previously used by transplant surgeons to prevent possible graft rupture due to excessive pressure during acute rejection. 64,65 Renal decapsulation has even been proposed for the treatment of inflammatory nephropathy, under the assumption that it can reduce renal parenchymal pressure in the acute phase and promote angiogenesis in the atrophied kidney in the chronic phase, thereby promoting the recovery of renal function. 9
Efficacy of local surgical treatments for AKI
Based on current research, renal decapsulation can effectively treat some cases of ischemia reperfusion injury/AKI when high pressure is maintained below the RFC. 10 –13 After 45 minutes of renal ischemia in mice or pigs, the pressure under the RFC increases due to early renal tubular dilation, renal interstitial edema, and fluid accumulation. Renal decapsulation can prevent a further reduction in renal function. 12,13 Like ischemia, renal decapsulation also plays a protective role in unilateral ureteral obstruction. 66 In addition, renal decapsulation is thought to prevent anuria and the rapid deterioration of renal function 2–3 days after allogeneic kidney transplantation, and it may also prolong the life of the transplanted kidney. 67 However, it is currently unclear whether patients with intrinsic renal compartment syndrome (IRCS) caused by AKI can be observed clinically; this requires further research.
However, complete renal decapsulation results in a short-term decrease in renal function, presumably due to a short-term decrease in the filtration capacity of the renal tubules and surrounding capillaries as a result of their dilation. 68 It has also been suggested that complete renal decapsulation compromises the role of MSCs in the renal peritoneum in promoting recovery from renal injury. 38 Partial renal decapsulation may be sufficient to prevent IRCS while avoiding the additional side effects of excessive renal compliance and loss of MSCs. 12 In addition, partial renal decapsulation may preserve the PeRF and promote its potential reparative effects on the injured kidney, such as stem cell migration or proangiogenesis. 8,69 The potential therapeutic benefits of renal decapsulation and the appropriate surgical methods deserve further evaluation.
Prospects
Integration with diverse biomaterials
Hydrogels have been widely used in local treatments with four primary effects: controlling sustained release, providing a suitable microenvironment, enhancing the therapeutic effect, and achieving a more uniform drug distribution. 7 When injected under the RFC, a hydrogel solidifies slowly at body temperature and can remain in place without leaking. The most commonly used hydrogels are alginate, 70 chitosan, 71,72 hyaluronic acid, 73 collagen, 63,74,75 extracellular matrix, 76,77 and gelatine. 78 Hydrogels enable sustained release, which can be improved by modifying the hydrogel structure. 79 –82 A hydrogel also creates a favorable environment for cell survival, proliferation, migration, and maturation and increases the efficacy of AKI treatment; examples include chitosan-based, 72 renal extracellular matrix, 83 and IGF-1C domain 71,84 hydrogels. In addition to being a vehicle for drugs, hydrogels have significant therapeutic benefits and can promote the regeneration of new renal tubules and growth of new blood vessels, as well as reduce renal fibrosis. 85
To overcome the problems of high diffusion resistance and uneven distribution of a hydrogel under the renal capsule, an artificial kidney capsule made by 3D printing was fabricated to wrap the hydrogel perfectly. 78 In conclusion, hydrogels are suitable for local application, and further investigation of their combination and optimization is warranted.
Ultrasound-assisted local administration
Low-frequency, low-intensity ultrasound (about 1 MHz and 0.1–0.5 W/cm2) promotes stem cell proliferation and activity. 86 –90 It may be quick, convenient, and economical to ultrasound the kidney after MSC transplantation, but this needs to be confirmed. Combined with microbubble destruction, ultrasound-targeted microbubble disruption (UTMD) is another possible method to improve the efficacy of MSC therapy. For example, UTMD promotes the homing of MSCs to the injured kidney. 91 –93 UTMD causes cavitation and sonic hole effects, which temporarily and reversibly opens vascular endothelial and cell uptake channels. 94,95 It is effective at unblocking vascular embolisms, 96 –98 opening the blood–brain barrier, 99,100 promoting gene transfection, 101,102 facilitating cell homing, 103 and enhancing the local penetration of exosomes. 104 In addition, the feasibility of UTMD-assisted gene delivery to the kidney has been demonstrated. 105 –107 Studies show that topical application of microbubbles is more efficacious than peripheral intravenous infusion. 101 With the improvement of ultrasonic microbubbles, it will become a safer and more effective tool for local delivery (Fig. 5). 108

Prospect: the application of ultrasound in combined treatment of acute kidney injury.
Potential pathways for clinical implementation of local AKI treatments
Other routes are being investigated, such as the renal vein and renal pelvis. Renal vein administration has higher transfection efficiency than peripheral vein administration, but does not appear suitable for patients. 109 The injection of plasmids, 110,111 viral vectors, 112,113 or nanomicelle-encapsulated mRNA 114 through the renal pelvis has higher gene transfection efficiency compared with the renal vein. However, suitable clinical approaches have not yet been developed.
As a potential stem cell nest, the PeRF can promote renal function recovery and is a possible space for local administration. 37,38 Although the PeRF has an adequate blood supply, its venous drainage to other sites may reduce drug concentrations in the kidney. 14,32 –34 However, after the RFC is removed, the PeRF communicates directly with the cortex, which may provide a better opportunity for the PeRF to assist in renal recovery. Perhaps combined with local surgery, the PeRF will become an ideal approach for administration.
Minimally invasive surgical techniques
The lack of tools to measure the pressure in the RFC led to inaccurate screening of suitable candidates, which may have resulted in uncertainty regarding the efficacy of surgery. A recent study indicates that renal decapsulation significantly protects renal function with ischemia for 45 minutes, but not for 35 minutes. 12 Therefore, renal decapsulation is unsuitable for all types of AKI, such that accurate screening and identification of patients with IRCS is required. In the IRCS pig, the pressure maintained in the RFC exceeds 20 mm Hg. 13 Clinical research recommends that the intraabdominal pressure should not exceed 20 mm Hg or anuria will occur. 115 To diagnose IRCS, it is important to consider multiple indicators, such as anuria and the rapid deterioration of renal function, before making a final judgment. Renal blood flow signals and intraabdominal pressure may reflect the pressure in the RFC, 65 and ultrasound elastography has been proposed for measuring the pressure under the RFC noninvasively, which offers the possibility of a fast diagnosis of IRCS. 116 In the context of minimally invasive surgery, laparoscopic renal decapsulation is more acceptable to patients. 117,118
Since laparoscopy requires expensive equipment, it would be ideal if a less invasive, more widely available surgical method could be developed to facilitate the emergency treatment of severe AKI in more modest settings (Fig. 6).

Prospect: renal decapsulation and subcapsular administration can be achieved with a single tube.
Conclusion
Local renal treatments of AKI, including local drug administration and surgery, have demonstrated markedly superior efficacy in animal models, garnering increasing interest among researchers to pursue this modality of treatment. When administering drugs locally, it is important to weigh the pros and cons of the different approaches before deciding on a new one. This review compared different approaches to help guide future laboratory work and clinical trials. Clinical studies of arterial and intrarenal injections confirm the clinical feasibility of both modalities. More clinical studies on the local renal treatment of AKI are worthwhile. The efficacy of renal decapsulation in the treatment of IRCS-AKI is supported by much evidence that justifies its reintroduction into clinical practice. However, the use of new diagnostic techniques, establishment of surgical indications, and invasive nature of the procedure must be considered.
Stem cell-based therapies, recognized for their potential to alleviate renal damage and promote kidney repair, demonstrate enhanced therapeutic efficacy and reduced side effects when applied locally. Furthermore, these therapies can be integrated with biomaterials, surgical interventions, or ultrasound stimulation, creating a comprehensive treatment system for renal restoration. A concept first introduced in this review is the use of a multifunctional ultrasound for diagnosis, surgery, and drug delivery in combined treatment. Ideally, ultrasound should be less invasive and more convenient as this would facilitate early treatment and improve the prognosis of patients with renal injury in emergency or military environments. We anticipate with optimism the future translation of more minimally invasive and efficacious localized treatment modalities into clinical practice.
Footnotes
Authors' Contributions
Y.-H.C. and T.X. contributed equally to this work; G.-Y.C., Q.H., and X.-M.C. conceived and designed the project; Y.-H.C. and T.X. wrote the article; X.-M.Z., Y.X., K.-T.Z., and W.-J.W. helped collect literature and draw pictures and tables; all authors read and approved the final article.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was supported by the National Natural Science Foundation of China (82170686), Grant for G.-Y.C. (22KJLJ001), and the National Key Research and Development Program of China (2022YFC3602900, 2018YFA0108803).