
Abstract
Objective:
To perform a systematic review to assess the incidence of reoperation rate for residual/regrowth adenoma after transurethral surgeries for benign prostatic enlargement.
Materials and Methods:
A systematic literature search was performed on November 12, 2023, using Cochrane Central Register of Controlled Trials, PubMed, and Scopus. We only included randomized studies comparing monopolar (M)/bipolar (B) transurethral resection of the prostate (TURP) vs ablation vs enucleation procedures. Incidence of reoperation was assessed using the Cochran-Mantel-Haenszel Method and reported as risk ratio (RR), 95% confidence interval (CI), and p-values. Statistical significance was set at p < 0.05.
Evidence synthesis:
Forty-eight studies were included. Six studies compared enucleation vs TURP, 41 ablation vs TURP, and 1 study enucleation vs ablation vs TURP, encompassing 457 patients in enucleation, 2259 in ablation, and 2517 in the TURP group. The pooled incidence of reoperation was 6.2%, 0.7%, 2.3%, and 4.3% after ablation, enucleation, M-TURP, and B-TURP, respectively. Meta-analysis showed that the incidence of reoperation was significantly lower in the enucleation group (RR 0.28, 95% CI 0.10–0.81, p = 0.02), but the difference accounted only in studies with follow-up between 1 and 3 years (RR 0.18, 95% CI 0.04–0.85, p = 0.03). The incidence of reoperation was significantly lower in the enucleation compared with the B-TURP group (RR 0.14, 95% CI 0.03–0.77, p = 0.02). Meta-analysis showed that the incidence of reoperation was significantly higher in the ablation group (RR 1.81, 95% CI 1.33–2.47, p = 0.0002), but there was no difference in studies with follow-up up to 1 year (odds ratio 1.78 95% CI 0.97–3.29, p = 0.06) longer than 5 years (RR 2.02, 95% CI 0.71–5.79, p = 0.19). The incidence of reoperation was significantly higher in the ablation compared with the M-TURP group (RR 1.91, 95% CI 1.44–2.54, p < 0.0001).
Conclusions:
In mid-term follow-up, reoperation rate for residual/regrowth adenoma was significantly lower after enucleation, although was significantly higher after ablation compared with TURP.
Introduction
Benign prostatic enlargement (BPE) is the leading cause of lower urinary tract symptoms (LUTS) in middle-aged and elderly men. Surgery is advised when pharmaceutical treatments prove ineffective or complications related to bladder outlet obstruction arise. 1 Since its introduction in the late 1930s, monopolar transurethral resection of the prostate (M-TURP) has remained for many decades the primary surgical choice for patients with a prostate volume ranging between 30 and 80 mL. 2 Over the past 30 years, new transurethral enucleation and ablation techniques showed equal or even superior effectiveness, coupled with reduced morbidity, even in cases of large prostate volume. 3,4
Patient satisfaction after BPE surgery not only relies upon improvement of symptoms, micturition parameters, and quality of life in the early postoperative period but also on the long-term durability of the same. As life expectancy among patients increases, this arises a greater likelihood of requiring reoperation for recurrent LUTS owing to regrowth adenoma after initial BPE surgery. Yet, a recent analysis of patients' perspectives on attributes, although choosing minimally invasive BPE surgery, demonstrated that 97% of respondents considered the ability to avoid further treatments as either “very important” or “extremely important” when selecting a procedure. 5 This scenario frequently poses challenges to the long-term outcomes of any BPE intervention, underwhelming the outcomes of the original surgery. The need for reoperation not only has social but also financial effects.
This review aims to systematically assess the incidence of surgical retreatment for residual/regrowth adenoma after BPE transurethral treatment in studies comparing TURP vs ablation vs enucleation procedures.
Evidence Acquisition
Aim of the review
The main outcome of this study was to assess differences in the incidence of surgical retreatment among different transurethral procedures, namely ablation, enucleation, and TURP. The secondary outcome was to assess the difference in retreatment rate according to the study follow-up period and the use of monopolar vs bipolar (B) electrocautery in resection.
Literature search
This study adhered to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. A comprehensive literature search was performed on November 12, 2023, using Cochrane Central Register of Controlled Trials, PUBMED, and Scopus. Medical Subject Heading terms and keywords were used as follows: (prostatic hyperplasia OR BPH OR benign prostatic enlargement OR benign prostatic obstruction) AND (Prostate resection OR Prostate enucleation OR Prostate vaporization OR ablation OR monopolar transurethral OR bipolar transurethral OR MTURP OR BTURP OR plasmakinetic OR PKRP OR PKEP OR PKERP OR TURis OR photovaporization or PVP OR PVEP OR holmium OR HoLEP OR thulium OR ThuLEP OR ThuVEP OR ThuFLEP diode OR DiLEP OR BTUEP OR MTUEP OR TUNA OR Aquablation OR Rezum OR Water vapor thermal therapy). There was no date restriction. Animal and pediatric studies were excluded. This review was registered in PROSPERO (Receipt No. 482741).
Selection criteria
The Patient Intervention Comparison Outcome Study (PICOS) type model was used to frame and answer the clinical question. Population: Men who underwent a surgical procedure for BPE; intervention: Transurethral procedures; comparison: M-TURP/B-TURP; outcome: Incidence reoperation for residual/regrowth adenoma after initial surgery; and study type: Prospective randomized studies. Transurethral procedures were categorized into two groups based on the technique used (enucleation and ablation), without regard to the energy applied. The enucleation group included the use of any laser and bipolar and monopolar electrocautery. The ablation group included bipolar/monopolar vaporization and any laser vaporization technique. The transurethral resection group consisted of M and B resection procedures. The incidence of reoperation was categorized according to the time between the reoperation and original surgical procedure in early (up to 1 year), medium (1–5 years), and long-term (>5 years) outcomes.
Study screening and selection
Two separate authors screened all gathered records through Covidence Systematic Review Management®. A third senior author solved discrepancies. Studies were included based on PICOS eligibility criteria. Only prospective randomized studies were accepted. Studies with no data on reoperation rate or with no patient in each group who required reoperation were excluded. Reviews, meeting abstracts, letters to the editor, case reports, editorials, and retrospective and prospective nonrandomized studies were also excluded. The full text of the screened articles was selected if deemed relevant to the aim of this study.
Statistical analysis
Incidence of reoperation was assessed using the Cochran-Mantel-Haenszel method with the random-effect model and reported as risk ratio (RR), 95% confidence interval (CI), and p-values. Analyses were two tailed and the significance was set at p < 0.05 and a 95% CI. RR <1 indicates that the intervention decreases the risk of reoperation. A subanalysis was conducted to investigate potential differences in the incidence of reoperation after monopolar and bipolar TURP procedures. Another subanalysis was performed to evaluate how the duration of study follow-up impacted the incidence of reoperation. Study heterogeneity was assessed utilizing the I
2 value. Substantial heterogeneity was defined as an I
2 value >50%. Meta-analysis was conducted using Review Manager (RevMan) 5.4 software by Cochrane Collaboration. Pooled analysis was performed using OpenMeta[Analyst] software (
Evidence Synthesis
The initial literature search yielded 11,648 articles. Upon removing 933 duplicated studies, 10,715 studies remained for screening. Another 10,465 articles were further excluded after the title and abstract screening owing to their lack of relevance to the study's purpose. The full texts of the remaining 250 studies were assessed and 202 articles were further excluded. Finally, 48 studies were accepted and included in the review. Six studies compared Enucleation vs TURP (Table 1). Forty-one studies compared ablation vs TURP (Table 2). One study compared enucleation vs ablation vs TURP (Tables 1 and 2). The complete list of studies included is available in Supplementary Appendix S1. Figure 1 shows the 2020 PRISMA flow diagram.
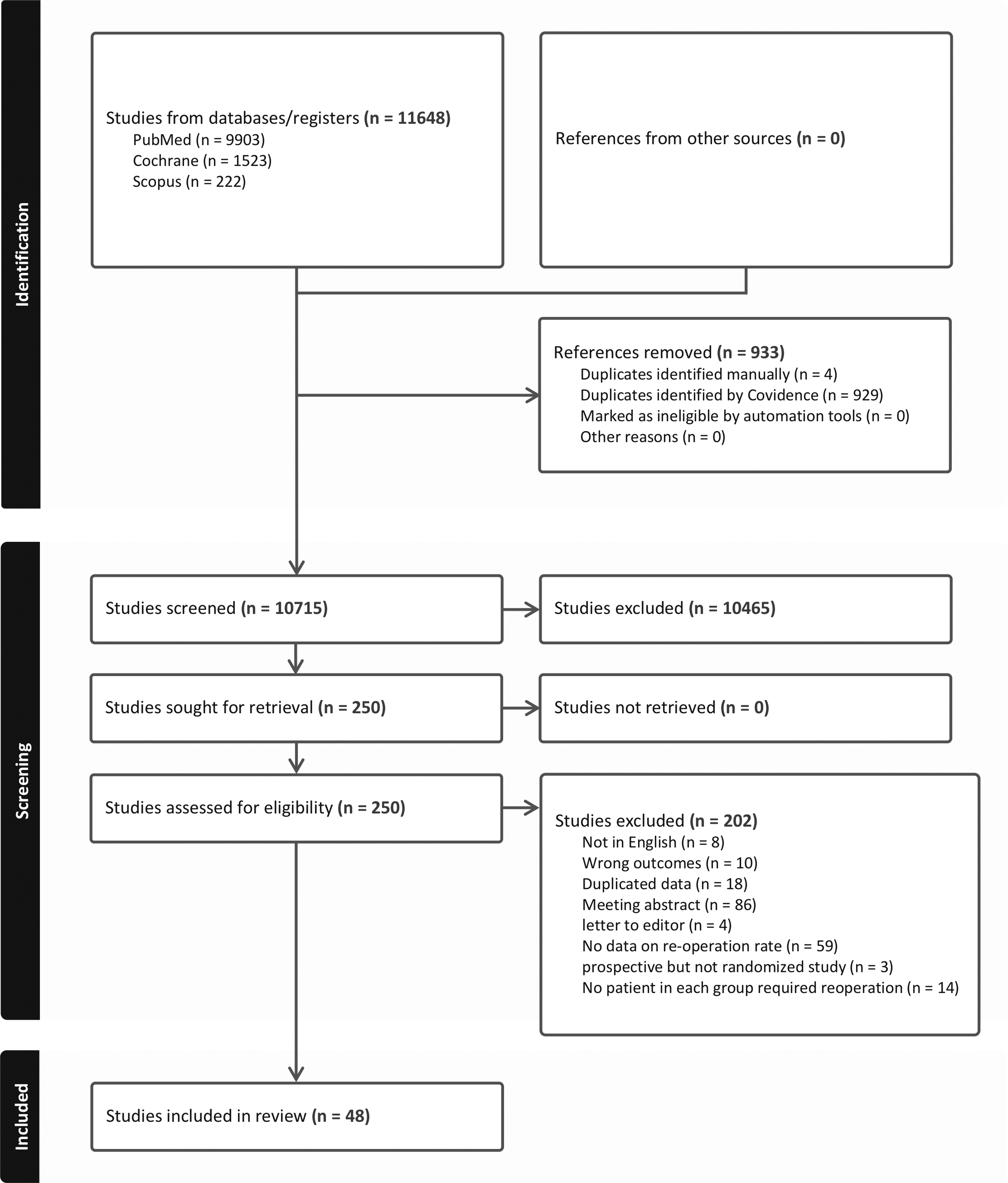
PRISMA flow diagram of the study. PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of Included Studies Comparing Transurethral Resection of the Prostate vs Enucleation
AUR = acute urinary retention; BEP = bipolar enucleation of the prostate; BPH = benign prostatic hyperplasia; GLL-PVP = green light laser photovaporization; HoLEP = holmium laser enucleation of the prostate; IPSS = international prostate symptoms score; LUTS = lower urinary tract symptoms; NA = not available; PCa = prostate cancer; PSA = prostate-specific antigen; PV = prostate volume; PVR = postvoiding residual; Qmax = maximum flow rate; QoL = quality of life; SD = standard deviation; ThuLEP = thulium laser enucleation of the prostate.
Characteristics of Included Studies Comparing Transurethral Resection of the Prostate vs Ablation
ASA = American Society of Anesthesiologists; B = bipolar; BLUES = British Laser Urological Evaluation Society; BOO = bladder outflow obstruction; BPE = benign prostatic enlargement; BPO = benign prostatic obstruction; CLP = contact laser prostatectomy; DRE = digital rectal examination; ELAP = endoscopic laser ablation of the prostate; GLL-PVP = green light laser photovaporization of the prostate; ILC = interstitial laser coagulation; M = monopolar; ND-YAG = neodymium-yttrium-aluminum-garnet; PVRU = ; TRUS = transurectal ultrasound; TUNA = transurethral needle ablation; TUVP = transurethral vaporization; UDS = urodynamic study; UTI = urinary tract infection.
Study quality assessment
There were 457 patients in enucleation, 2259 in ablation, and 2517 in the TURP group.
Supplementary Figure S1 shows the details of quality assessment for studies comparing enucleation vs TURP. Four studies showed some concerns about the overall risk of bias. One study showed a high overall risk of bias and the remaining two studies had a low overall risk of bias. The most frequent reason for bias was attributable to deviation from intended interventions, followed by bias arising from the randomization process. Supplementary Figure S2 demonstrates the details of quality assessment for studies comparing ablation vs TURP. Seventeen studies showed a low overall risk of bias. Twenty-one studies showed some concerns regarding the overall risk of bias and the remaining ones had a high overall risk of bias. The most frequent reason for bias was bias from the randomized process, followed by bias attributable to deviation from intended interventions.
Incidence of reoperation after M-TURP
The pooled incidence of reoperation in patients who underwent M-TURP ranged from 1.5% to 3.0%, with a pooled rate of 2.3% (Supplementary Fig. S3).
Incidence of reoperation after B-TURP
The pooled incidence of reoperation in patients who underwent B-TURP ranged from 0.9% to 7.8%, with a pooled rate of 4.3% (Supplementary Fig. S4).
Incidence of reoperation after ablation
The pooled incidence of reoperation in patients who underwent ablation ranged from 4.7% to 7.8%, with a pooled rate of 6.2% (Supplementary Fig. S5).
Incidence of reoperation after enucleation
The pooled incidence of reoperation in patients who underwent enucleation ranged from 0% to 1.5%, with a pooled rate of 0.7% (Supplementary Fig. S6).
Reoperation rate: Enucleation vs TURP
Meta-analysis for 7 studies (457 enucleation and 444 TURP cases) showed that the incidence of reoperation was significantly lower in the enucleation group (RR 0.28, 95% CI 0.10–0.81, p = 0.02) (Fig. 2). There was no significant heterogeneity among the studies (I 2 0%). Subanalysis demonstrated that the difference in reoperation rate was significantly lower in the enucleation group only in studies with follow-up between 1 and 3 years (RR 0.18, 95% CI 0.04–0.85, p = 0.03).

Forrest plot of reoperation in studies comparing enucleation vs TURP according to follow-up period. TURP = transurethral resection of the prostate.
A further subanalysis showed that the incidence of reoperation was similar between M-TURP and enucleation (RR 0.43, 95% CI 0.10–1.80, p = 0.25) and significantly lower in the enucleation compared with the B-TURP group (RR 0.14, 95% CI 0.03–0.77, p = 0.02) (Fig. 3).
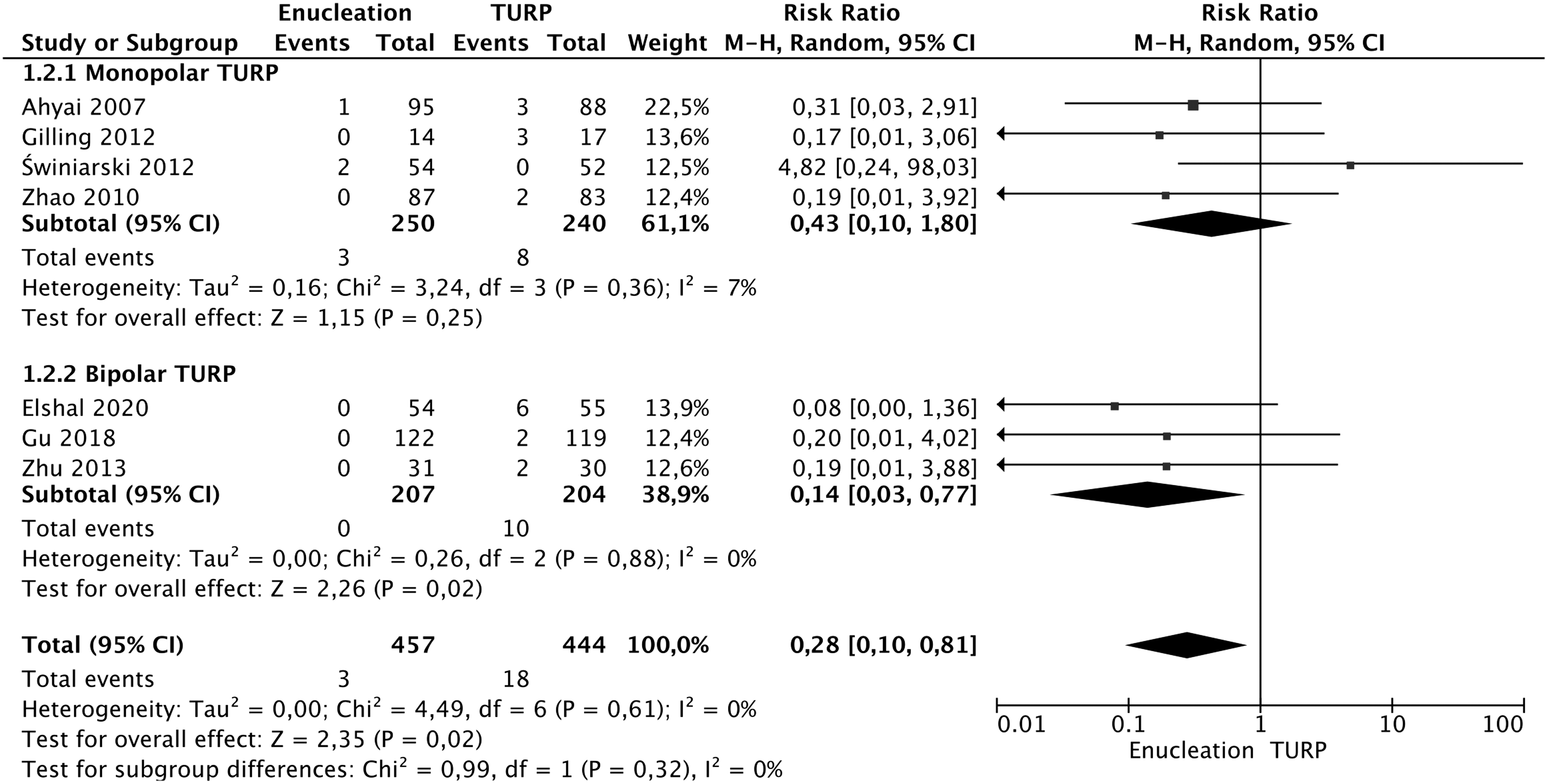
Forrest plot of reoperation in studies comparing enucleation vs TURP, subgroup analysis for monopolar and bipolar TURP.
Reoperation rate: Ablation vs TURP
Meta-analysis for 43 studies (2596 ablation and 2499 TURP cases) showed that the incidence of reoperation was significantly higher in the ablation group (RR 1.81, 95% CI 1.33–2.47, p = 0.0002) (Fig. 4). Study heterogeneity was low (I 2 17%). Subanalysis demonstrated that the difference in reoperation rate was significantly higher in the ablation group in studies with mid-term follow-up (1–3 years, odds ratio (OR) 2.20 95% CI 1.1–4.37, p = 0.02; 3–5 years, OR 1.84 95% CI 1.18–2.88, p = 0.008), but not in studies with short and longer than 5 years of follow-up. A further subanalysis showed that the incidence of reoperation was similar between B-TURP and ablation (RR 0.68, 95% CI 0.34–1.37, p = 0.28) and significantly higher in the ablation compared with the M-TURP group (RR 1.91, 95% CI 1.44–2.54, p < 0.0001) (Fig. 5).
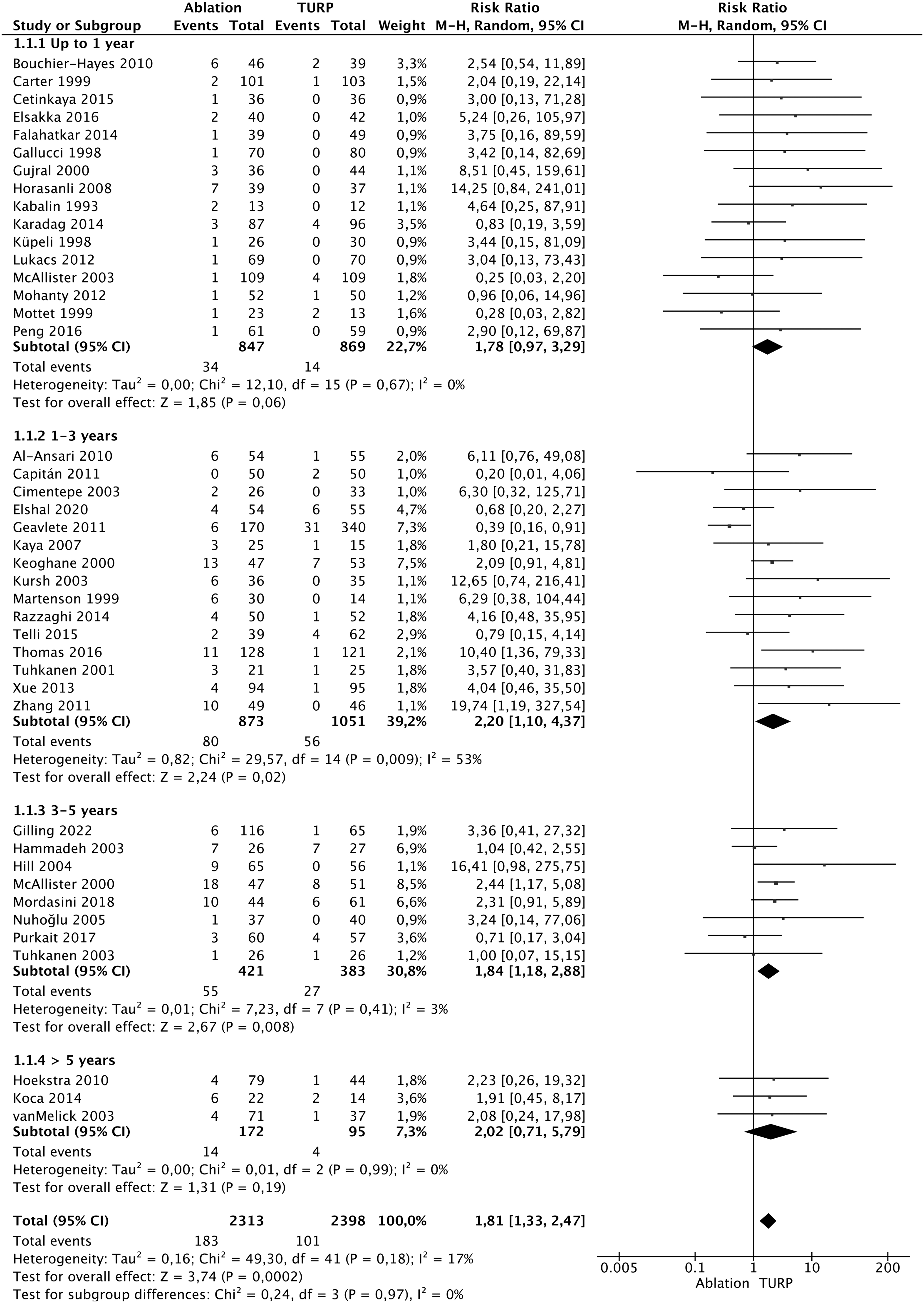
Forrest plot of reoperation in studies comparing ablation vs TURP according to follow-up period.

Forrest plot of reoperation in studies comparing ablation vs TURP, subgroup analysis for monopolar and bipolar TURP.
Discussion
From patients' and surgeons' perspective in the modern era, any BPE intervention should have minimal morbidity, improve symptoms and quality of life, and withstand the test of time, which is ideal to provide a lifetime solution. Despite data showing that improvements of LUTS and micturition parameters are sustained for over 10 years, 6 a second prostatic operation after TURP has been reported at a constant annual rate of ∼1% to 2%, with a reoperation rate for BPE of between 8.3% 7 and 12.0% 8 at 8 years after primary TURP.
Holmium laser enucleation of the prostate (HoLEP), Thulium laser enucleation of the prostate (ThuLEP), green light laser photovaporization of the prostate (GLL-PVP), and B-TURP demonstrated a shorter hospital stay and fewer early complications compared to M-TURP. 4,6,9 However, to replace traditional TURP as the new gold standard surgical treatment, these new procedures should also demonstrate durable outcomes in terms of the need for reoperation. This is clearly demonstrated by Eredics and colleagues who showed that 85% of their cohort survived for 8 years after TURP and even within the 70 to 79 year cohort, the 8-year survival was nearly 75%. 7
To the best of our knowledge, our review is the first study that assessed and compared the reoperation rate for BPE intervention in randomized trials comparing TURP vis a vis enucleation and ablation.
Although enucleation techniques may have a steep learning curve varying from 30 cases for ThuLEP 10 to 50 for HoLEP 11 and bipolar enucleation, 12 in our study, enucleation had the lowest rate of reoperation, despite the learning curve being able to very well influence the data for reoperation. Indeed, the learning curve may partially explain why reoperation is possible despite enucleation should be, in theory, a better anatomically designed procedure by dissecting and separating adenoma from the peripheral zone. Once the learning curve is mounted, enucleation could offer a more “radical” and complete adenoma removal vis a vis TURP, and hence this could account for the better results compared to TURP in our study.
This hypothesis is supported by Elzayat and Elhilali who showed that the reoperation rate in their HoLEP series of 118 patients with a mean follow-up of 49.4 months was 4.2%, but the retreatment rate in the first 50 cases was higher compared with the following 68 cases (8% vs 1.4%, respectively). 13 Another reason for the persistence or recurrence of adenoma after enucleation might be attributed to the multinodular nature of benign prostatic hyperplasia. This involves the potential regrowth of a few subcapsular nodules not completely enucleated, subsequently leading to regrowth and recurrent obstruction. The latter can occur also in small-volume prostates where a less distinct or clear plane of enucleation might not always be as apparent as in larger glands. 14
It is common evidence that sometimes, urologists need to stop TURP, particularly in patients with large volume prostate. This is frequently associated with intraoperative bleeding-related poor vision or prolonged surgery with the fear of transurethral resection syndrome. Actually, during enucleation, major vessels are accessed only once at the level of the surgical capsule, which is reached early and then followed through. In contrast, these same vessels are opened and reopened multiple times until reaching the surgical capsule in TURP. At this juncture, final coagulation can be completed. Theoretically, this disparity could result in more significant bleeding and a greater amount of tissue left behind if vision is compromised, particularly in larger glands. 9
As a consequence, obstructing adenoma can be left inside, leading to early reoperation. In a study of more than 3500 single-surgeon M-TURP, Tasc et al. performed early re-TURP in almost 1% of their patients because of recurrent postoperative recatheterization. 15 The persistence of obstructing residual adenoma can explain our results of a significantly lower rate of reoperation between 1 and 3 years after enucleation compared with TURP.
However, there was no difference in reoperation rate behind 3 years of follow-up and this might be related to fewer studies and patients. Another important argument in favor of the role of residual obstructing adenoma after inadequate resection is demonstrated in the study by Aagaard et al. 16 They found that the reoperation rate at an 8-year follow-up after minimal prostate resection was 23%, whereas for “radical” resection, it stood at 7%. Therefore, this difference could be linked to the extent of resection performed and an incomplete resection should be suspected when patients require restarting medical therapy in the early postoperative period since this has been recognized as a risk factor for secondary TURP. 17 As a consequence, urologists performing TURP should always pursue a complete adenoma removal, whenever feasible, to avoid reoperation.
Another important finding of our study was the significantly higher reoperation rate after Ablation procedures compared with M-TURP. In a recent meta-analysis, TURP demonstrated a more substantial improvement in micturition parameters compared to GLL-PVP over a 5-year period. 4 These findings indicate that, although GLL-PVP is highly effective initially, its efficacy probably diminishes over time. The relatively lower reduction of prostatic adenoma by GLL-PVP might elucidate its declining effectiveness in micturition over the long term. Furthermore, this evidence converts to a higher incidence of reoperation owing to the persistence or regrowth of prostatic adenoma (RR 0.64, 95% CI 0.41–0.99). 4
Therefore, this difference in reoperation rate could potentially be linked to inadequate energy delivery during the procedure, leading to incomplete tissue removal, possibly attributable to the surgeon's early learning curve, or ineffective tissue ablation by low-performance lasers employed in the late 1990s and early 2000s. In fact, the reoperation rate over 30 months of follow-up after 80 W PVP was high at 6.8%, but the authors of this study argued that redo surgery was also related to their learning curve since the reoperation rate decreased from 10% to 0%–5% after each surgeon's initial and subsequent 30 cases, 18 thus indicating once again the important role of experience in minimizing subsequent reintervention for adenoma regrowth owing to residual tissue. The hypothesis of incomplete tissue ablation is also supported by our results of a pooled rate of reoperation after ablation of 6.2%, much higher than enucleation and both M-TURP and B-TURP.
Moreover, reoperation after GLL-PVP is also influenced by prostate volume, as demonstrated by Kim et al. 19 The authors showed that even using a high-performance laser (i.e., 120 W), patients requiring reoperation had a significantly larger prostate volume (74.2 g vs 53.0 g), longer lasing time (45.8 minutes vs 36.5 minutes), and greater mean total energy use (219.3 kJ vs 153.6 kJ). However, when a “radical” tissue ablation is performed, such as in Aquablation, freedom from a secondary BPO surgical treatment was 96.3% at 5-year follow-up in men with a prostate volume between 80 and 150 mL, 20 and the reoperation rate was similar to TURP in a randomized study. 21 Hence, as for TURP, it becomes imperative to thoroughly and effectively ablate the prostate tissue to ensure the continual patency of the prostatic cavity, especially in patients with a larger prostate.
The surgical procedure itself is not the sole factor associated with reoperation. Some patient-related factors need to be taken into consideration. Interestingly, data support that the risk of repeat TURP increases with age. 7,22 In fact, Eredics et al. demonstrated a higher re-TURP rate in men 80 years of age and older compared with younger men. 7 The authors speculated that the elevated occurrence of detrusor overactivity, detrusor underactivity, and a reduced frequency of bladder outflow obstruction in the elderly could contribute to a less satisfactory outcome. 23 This might have subsequently led to secondary interventions, potentially explaining these differences.
This study has some limitations. First, the absence of commonly reported data on the learning curve of the involved surgeons could have introduced bias in the reoperation rate. Achieving a truly unbiased comparison among procedures remains quite challenging under these circumstances. Second, postoperative urodynamics was not routinely performed by most of the included studies and the incidence of truly persistent/de novo bladder outlet obstruction cannot be assessed. Third, no data were reported on the outcomes of patients who required reoperation to elucidate the outcomes of the secondary surgery, particularly to understand its true value in those suffering from persistent/recurrent LUTS after primary bladder outlet relief.
No study included in our review reported data on cost-analysis outcomes, and hence no conclusion can be drawn for which procedure is more cost-effective. However, studies focusing on this subject showed inhomogeneous results, some supporting enucleation, 24 whereas some favoring TURP 25 or minimally invasive procedure 26 as the most cost-effective procedure. Finally, no information could be collected on what potential surgical intraoperative technique was used for both groups to make any affirmation on which technique is better for TURP or enucleation, respectively.
Conclusions
In this study, we compared transurethral enucleation and ablation procedures against TURP to estimate the incidence of retreatment for residual/regrowth adenoma after surgery. We found that ablation has the highest rate of reoperation, followed by B-TURP and M-TURP, whereas enucleation has the lowest. Comparing all procedures, ablation shows a significantly higher reoperation rate compared to TURP in early and mid-term but not in long-term follow-up. Conversely, enucleation demonstrates a lower retreatment rate between 1 and 3 years. Our findings can provide urologists with valuable insights to counsel their patients regarding the reoperation rate for residual/regrowth adenoma based on the surgical intervention offered.
Footnotes
Authors' Contributions
Conception and design: D.C., J.Y.-C.T., and V.G. Acquisition of data: D.C., P.T., G.C., A.C., A.R., C.N., L.P., S.S., and V.D.S. Statistics: D.C. Drafting of the article: D.C. Critical revision for important intellectual content: J.Y.-C.T., L.C., B.K.S., and V.G. Supervision: A.B.G. All authors participated in article writing, review, and approval of the final version of the article for submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.