
Abstract
Purpose:
This study aims to report our experience in the treatment of children with retrocaval ureter (RCU) using laparoscopic ureteral reconstruction surgery.
Patients and Methods:
We retrospectively collected clinical data from 10 pediatric patients with RCU who underwent laparoscopic surgery at our hospital from April 2010 to April 2022. All patients underwent comprehensive preoperative radiological assessment and were diagnosed with RCU, subsequently undergoing laparoscopic ureteral reconstruction. Patient demographics, surgical data, and postoperative outcomes were recorded. Regular follow-ups were conducted postoperatively, evaluating clinical symptoms and radiological results.
Results:
The median age of the 10 patients was 8.8 years (range, 6–14 years). All surgeries were successfully performed laparoscopically without the need for open conversion, with an average surgical time of 153.3 minutes (range, 120–243 minutes). Intraoperative bleeding was minimal and no blood transfusions were required. No intraoperative complications were observed. The average hospital stay for the patients was 5.3 days (range, 4–7 days) and the Double-J (D-J) stent was removed 6 weeks postoperatively. Follow-up ultrasound results at 3 and 6 months postoperatively showed a reduction in renal pelvic dilatation, and all patients experienced significant relief of clinical symptoms related to flank and abdominal discomfort.
Conclusion:
Laparoscopic reconstruction for RCU demonstrates good feasibility and effectiveness in pediatric patients, offering a minimally invasive treatment option for the management of RCU in children.
Introduction
Retrocaval ureter (RCU) is a congenital anatomical anomaly characterized by aberrations in ureteral position and trajectory resulting from abnormal inferior vena cava development. During embryogenesis, the persistence of the posterior cardinal vein, integrating into the inferior vena cava, causes the ureter to follow a circuitous path behind and medially around the inferior vena cava before returning to its normal course into the bladder. Typically, this anomaly manifests on the right side owing to its distinctive pathogenesis. However, in rare instances involving atypical left-sided inferior vena cava courses or visceral inversion, RCU can occur on the left. Although clinically infrequent, compression of the right ureter passing behind the inferior vena cava can induce obstruction, leading to renal hydronephrosis and proximal ureteral dilation. 1 Clinical manifestations encompass lumbar pain, hematuria, urinary tract infections, and stones, with severe cases resulting in functional loss of the right kidney. The incidence is three times higher in males than females 2 and clinical symptoms usually become noticeable in the thirties or forties, 3 with cases in children being relatively uncommon.
Ureteral reconstruction surgery stands as the standard treatment for RCU, including open surgery, retroperitoneal laparoscopic surgery, transperitoneal laparoscopic surgery, and robot-assisted surgery. 4 Each approach presents distinct advantages and disadvantages. Although traditional perspectives favor open surgery as the standard, attention has shifted toward minimally invasive techniques. Laparoscopic ureteral reconstruction for RCU, in comparison to open surgery, offers reduced invasiveness and enhanced cosmetic benefits. 5 However, existing literature predominantly focuses on the diagnosis and minimally invasive treatment of RCU in adults with limited case numbers. This paper consolidates our center’s 12-year experience in utilizing laparoscopic reconstructive surgery to address pediatric RCU cases, demonstrating the feasibility and efficacy of this approach. Our findings aim to provide a valuable reference for the future treatment of similar cases.
Patients and Methods
Case data
Following approval from the Ethics Committee of Anhui Provincial Children’s Hospital (Approval No. 116123S21), a retrospective analysis was conducted on clinical data of pediatric patients diagnosed with RCU and undergoing laparoscopic surgery in the Department of Urology from April 2010 to April 2022. In total, 10 cases of RCU were included in the study, comprising 8 male and 2 female patients. The average age was 8.8 years (range, 6–14 years) and the mean weight was 27.8 kg (range, 20–39 kg). The primary clinical manifestations were abdominal pain in 8 patients, whereas the remaining 2 patients were asymptomatic, with right renal pelvis dilation and upper ureteral expansion incidentally discovered during ultrasound examination. Two patients exhibited microscopic hematuria.
Preoperative management
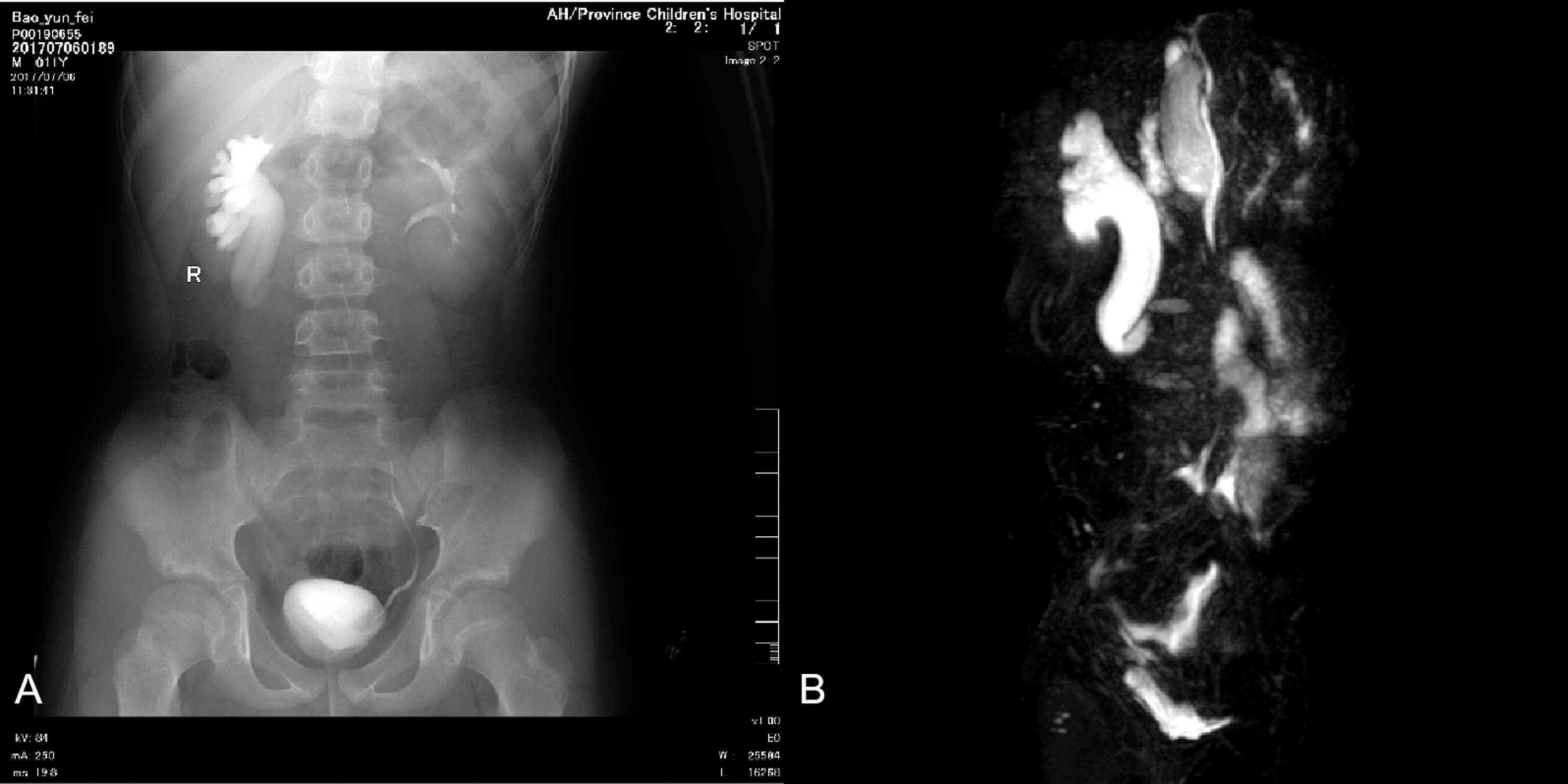
All patients underwent preoperative renal, ureteral, and bladder ultrasonography, intravenous urography (IVU), and magnetic resonance imaging (MRI) assessment. Radiological examinations revealed right renal pelvis dilation and proximal ureteral expansion in all patients, displaying the characteristic “fishhook” deformity of the ureter, with displacement from the outer to inner side of the inferior vena cava (Fig. 1A, B). According to the classification proposed by Bateson and Atkinson, all patients exhibited Type I RCU. 6
Surgical management
After induction of general anesthesia through an endotracheal tube, a Foley catheter was placed into the bladder and clamped. None of the patients underwent retrograde ureteropyelography or retrograde insertion of a D-J stent. Two surgeons performed laparoscopic ureteral reconstruction through a transperitoneal approach, with all procedures involving ureterostomy, including excision of the compressed and obstructed segment of the ureter. Three trocars were used during the surgery: a 5-millimeter trocar for a 30° optical scope was placed at the left margin of the umbilicus. Two additional trocars of 3 mm and 5 mm were placed, one along the midline below the level of the umbilicus by about 2 cm and the other 3 cm above the umbilicus. After mobilizing the entire ascending colon to expose the right renal pelvis (Fig. 2A), the right ureter was adequately freed and exposed using an ultrasonic scalpel (Fig. 2B). The proximal ureter was transected before passing behind the inferior vena cava (Fig. 2C), and in three cases with significantly narrowed ureters, the affected segments were excised (Fig. 2D). The repositioned ureter was placed in front of the inferior vena cava and sutured intermittently with 5-0 absorbable sutures. After completing the anastomosis of the anterior wall of the ureter, the posterior wall of the ureter was exposed. A novel technique was employed here to place the D-J stent, with a 5-millimeter suction catheter containing a wire and push rod used to insert the D-J stent into the abdominal cavity through the 5-mm trocar on the right side. The distal end of the D-J stent entered the bladder through the anastomotic opening of the ureter (Fig. 2E), and by pressing the bladder area, urine reflux was observed, confirming the entry of the distal end of the D-J stent into the bladder and the proximal end entering the renal pelvis. The clamped ureteral catheter was then opened. The posterior wall of the ureter was further intermittently sutured with 5-0 absorbable sutures (Fig. 2F). All patients had a laparoscopic drain placed and removed 2–3 days postoperatively.

Results
In our study, all surgeries were successfully completed laparoscopically without the need for conversion to open surgery. The average surgical duration was 153.3 minutes (range, 120–243 minutes). Intraoperative blood loss was minimal and not quantifiable, with no patients requiring blood transfusion, and no observed intraoperative complications. Seven patients underwent ureteral anastomosis without excision of any renal pelvis–ureteral junction segment. In the remaining three patients, the RCU appeared narrowed, and ureteral reconstruction was performed after excising the narrowed segment.
All patients experienced smooth recoveries, with an average hospital stay of 5.3 days (range, 4–7 days). Before discharge, urinary catheters and laparoscopic drains were removed. Six weeks after surgery, the D-J stent was removed cystoscopically. During the period with the D-J stent, amoxicillin was administered orally before bedtime to prevent urinary tract infections. All patients underwent ultrasound examinations at 3 and 6 months postoperatively, with additional IVU if necessary. The obtained ultrasound results revealed unobstructed anastomosis, significant improvement in ureteral obstruction, and notable reduction in renal hydronephrosis. Children who experienced preoperative lumbar abdominal discomfort and microscopic hematuria showed complete symptom relief postoperatively. Pathological examination of the excised segments of the RCU with stenosis showed signs of fibrosis and nonspecific inflammation. In one case, a child who underwent resection of the stenotic segment of the ureter was found to have ureteral polyps on postoperative pathology, and this surgery took about 4 hours primarily owing to unclear visibility, bleeding, and challenging suturing. Table 1 summarizes the general information and perioperative data of the patients.
General Information and Perioperative Data of the Patients
F = female patient; M = male patient; RCU = retrocaval ureter.
Discussion
RCU, also known as circumcaval ureter or preureteral vena cava, was initially documented by Hochstetter in 1893 as a rare congenital anomaly resulting from inferior vena cava underdevelopment. 1 –8 Bateson and Atkinson 6 classified RCU into two types based on imaging studies. Type I, the more prevalent form, exhibits a characteristic S-shaped or fishhook deformity of the ureter (Fig. 1A, B), often leading to moderate-to-severe hydronephrosis. Conversely, Type II is a less common variant characterized by a sickle-shaped ureteral curve, infrequently causing ureteral obstruction. For patients with mild hydronephrosis and no evident clinical symptoms, follow-up observation is recommended. 7 Surgical intervention, however, becomes necessary when patients exhibit symptoms such as lumbar abdominal discomfort or worsening hydronephrosis impacting renal function. 8,9
Imaging plays a pivotal role in diagnosing RCU, and confirmation can be achieved through IVU and retrograde urethrography, with some scholars advocating the use of helical computed tomography (CT) or MRI. 9 –11 Radiologists prefer static magnetic resonance urography (MRU) for RCU identification. 11,12 Dillon et al. proposed MRI as a well-suited modality for suspected RCU evaluation, 13 emphasizing its superiority over CT owing to its radiation-free nature and ability to delineate the anatomical relationship between the inferior vena cava and the right ureter. 8,11 –13 However, Chen et al. argued that computed tomography urography (CTU) should be the preferred diagnostic method for RCU as it accurately depicts the anatomical relationship between the inferior vena cava and the ureter being noninvasive. 9 In our institution, ultrasound is often insufficient for RCU diagnosis, detecting only renal pelvis dilation and proximal ureteral expansion. Despite its limitations, ultrasound is a cost-effective and easily implementable initial screening tool for symptomatic children, such as those presenting with lumbar abdominal discomfort, with further investigation using IVU or MRI warranted if RCU is suspected. Both IVU and MRI examinations can demonstrate the characteristic “fish hook” deformity in patients with RCU, which is beneficial for making a definitive diagnosis.
Pyeloplasty and ureterostomy represent established surgical modalities for addressing RCU, with open surgery historically favored as the primary method. 2 However, the past decade has witnessed the evolution of minimally invasive surgical techniques and associated technologies, culminating in the emergence of laparoscopic surgery as a viable option for RCU treatment. 14 Laparoscopic surgery, as a minimally invasive approach for pediatric RCU, offers notable advantages in delivering personalized, safe, and effective treatment. 4,5,8 In comparison to traditional open surgery, it features smaller incisions, favorable aesthetics, diminished postoperative pain, and facilitates prompt discharge and recovery in children. 4,5,9 The laparoscopic repertoire for RCU encompasses transperitoneal approaches, 1,4,5,10 retroperitoneal approaches, 9,15 and robot-assisted ureteral reconstruction, 5,16 each with its unique merits and demerits, often contingent on the surgeon’s preferences and experience. 17
The transperitoneal approach, owing to a larger operating space, enhanced ureteral exposure, a more familiar anatomical structure, and a less steep learning curve, is often considered time-efficient and comparatively easier than the retroperitoneal approach. 1,2,18 Conversely, some researchers posit that the retroperitoneal approach holds advantages over the transperitoneal method because of minimal dissection, reduced impact on gastrointestinal function, and expedited direct access to the renal pelvis and ureter without intruding into the peritoneal cavity. 9,19 Notably, robot-assisted surgery maintains stable advantages over traditional laparoscopic surgery, furnishing an excellent three-dimensional view of the surgical field, increased manual dexterity, and improved intraoperative suturing and knotting capabilities. 9,20 Furthermore, robot-assisted ureteral reconstruction is deemed technically easier, safer, and faster, with abbreviated surgical times. 5,16 However, the cost associated with robot-assisted surgery poses a challenge, particularly for parents in economically underdeveloped provinces such as Anhui. In addition, this technique demands heightened surgical expertise and entails a steep learning curve. 5 Consequently, the selection of the surgical approach necessitates a judicious balance, considering the patient’s specific circumstances and the availability of medical resources. Drawing from our single-center experience, we express a preference for the transperitoneal approach owing to its provision of a conducive working space and clear surgical visibility for precise intracorporeal suturing, facilitating a more meticulous observation of ureteral anatomy anomalies.
The decision to remove or retain the retrocaval segment of the ureter has been a matter of debate, lacking a current consensus. In the published literature, most surgeons lean toward retaining the ureter, especially in patients undergoing pyeloureterostomy and pyelopyelostomy. 5 On the other hand, retrocaval ureteral resection is primarily carried out in ureteroureterostomy procedures. 9 In our series, we opted for ureteral resection in three patients because of significant narrowing observed under laparoscopic magnification, and pathological results confirmed marked stenosis, indicating signs of fibrosis and nonspecific inflammation in RCU. Notably, we identified a case of ureteral polyps in a patient with RCU who underwent ureteral resection. The polyps were discovered postoperatively through pathology examination of the excised ureteral segment. This patient underwent a 4-hour reconstructive surgery primarily owing to unclear visibility and bleeding, making suturing challenging.
The placement of the D-J stent presents another challenge in laparoscopic surgery for RCU. Some surgeons employ preoperative cystoscopy to retrogradely place the D-J stent. 21 However, this cystoscopy-guided catheterization procedure, coupled with changes in patient position, often extends the surgical time, and the preplaced ureteral stent or guidewire may interfere with the transection and anastomosis of the ureter. In our approach, we introduced a novel technique for D-J stent placement, utilizing a D-J stent with a guide wire and push rod inserted into a 5-mm suction metal rod. This assembly was then introduced into the abdominal cavity through the 5-mm trocar on the right side. The distal end of the D-J stent entered the bladder through the ureteral anastomosis site (Fig. 2E), and urine reflux was observed upon pressing the bladder area, confirming proper stent placement. This technique mitigates the complications associated with cystoscopy examination and retrograde catheter placement, contributing to a reduction in surgical time. We recommend this approach for its expeditious, safe, and straightforward execution.
This study has several limitations. First, our sample size is relatively small, which may limit the generalizability of our findings. Second, the average length of hospital stay in our region is longer compared to Western countries. 8 This is partly due to our clinical practice of placing both a D-J stent and a laparoscopic drain to ensure proper drainage as we have encountered anastomotic leakage in the past. This precautionary measure prolongs the hospital stay. In future studies, we aim to adopt improved techniques to reduce the length of hospital stay. In addition, our health care system necessitates a series of preoperative examinations after hospitalization, further extending the hospital duration. Furthermore, our study is limited by the retrospective nature of the data collection, and the lack of long-term follow-up data may affect the assessment of the procedure’s long-term efficacy and outcomes. Future research with larger sample sizes, shorter hospital stays, and longer follow-up periods is needed to validate and expand upon our findings.
Conclusion
Reconstruction of RCU through the transperitoneal approach demonstrates good feasibility and effectiveness in pediatric patients, offering a more extensive operating space, better ureteral exposure, a more familiar anatomical structure, and an easier learning curve. This minimally invasive treatment provides an effective option for the treatment of RCU in children. Placing a D-J stent through a 5-mm suction metal rod during surgery is a feasible and efficient alternative. However, due to the limited number of cases, larger-scale, long-term follow-up studies are still needed to further verify the safety and effectiveness of laparoscopic reconstruction of RCU through the transperitoneal approach.
Footnotes
Authors’ Contributions
C.K.M.: Project development, data management, data analysis, and article writing. T.Z.: Project development, data collection, article review, and editing. Y.S.C.: Data collection and data analysis.
Author Disclosure Statement
All authors declare no competing interests.
Funding Information
This work did not receive any funding.