
Abstract
Purpose:
This study investigates gender-based disparities in health-related quality of life (HRQOL) outcomes among kidney stone patients and explores potential contributing factors.
Methods:
A retrospective review of medical records at the University of Rochester Medical Center was conducted on 2199 new urolithiasis patients who completed the Wisconsin Stone Quality of Life Questionnaire (WISQOL) standardized on a 0 to 100 scale. Demographic and clinical data were collected. Statistical analyses included univariate tests, chi-squared tests, and multivariate linear regression.
Results:
Of the 2199 kidney stone patients, 1085 (49.3%) were women. Women reported significantly lower quality of life (QoL) scores compared with men (71.6 vs 80.7; p < 0.001), and this persisted across all domains, including social impact (80.2 vs 86.9; p < 0.001), emotional impact (67.3 vs 77.1; p < 0.001), disease impact (67.3 vs 77.1; p < 0.001), and impact vitality (62.6 vs 72.9; p < 0.001). Female gender was identified as an independent predictor of diminished QoL scores, along with younger age, symptomatic status, number of surgeries, and presence of a psychosocial comorbidity.
Conclusions:
Our findings suggest that women with kidney stones experience lower HRQOL compared with men, even accounting for clinical and demographic factors. Although this study provides preliminary insights, additional research is needed to validate these findings in broader and more varied populations.
Introduction
The prevalence of kidney stones in the United States is ∼9%, with a notable increase over recent years. 1 This uptick can be attributed to various factors, including shifts in dietary habits, comorbid diseases, changes in social conditions, and climate changes. Kidney stones not only pose a substantial economic cost, with annual projections surpassing $10 billion, 2 but individuals affected often experience substantial burdens, such as bodily pain, disruptions in social function, and an overall decline in quality of life (QoL). 3 The growing emphasis on patient-reported disease severity has led to an expanded focus on health-related quality of life (HRQOL) assessment in urology and across medical disciplines. Integrating such insights with medical treatments for stone disease enables targeted interventions to improve patient QoL.
The Wisconsin Stone Quality of Life Questionnaire (WISQOL) is a validated kidney stone-specific tool that has been increasingly used to measure HRQOL. It encompasses multiple factors of QoL, including social functioning, emotional functioning, stone-related symptom impact, and vitality. 4 Previous studies using WISQOL have revealed significant correlations between patients in neighborhoods with high social vulnerability and lower QoL scores. 5 Moreover, factors including lower income, nonwhite race, unemployed work status, younger age, shorter duration of disease, and shorter time since stone passage have been identified as independent predictors of worse WISQOL scores. 6,7
Historically, men were twice as likely to develop kidney stones compared with women; however, the prevalence of kidney stones among women is increasing. 8 A study using a database of inpatient stays compiled from hospitals in the United States showed that female discharges for renal calculi increased by 22% over a 5 year window. 9 Gender differences in HRQOL among kidney stone patients have been well documented, with women experiencing worse outcomes compared with men. 3,10,11
However, the complexity of the relationship between gender and HRQOL in the context of kidney stones warrants further exploration. This study aims to compare reported HRQOL outcomes among men and women with kidney stones. Our primary hypothesis is to confirm prior reports that women with kidney stones experience lower HRQOL compared with men. In addition, we seek to explore whether any differences exist in the degree of invasiveness of stone surgical treatment, age, and symptomatic status.
Methods
Study design and data
This retrospective review of medical records, approved by the Institutional Review Board (IRB00008211), examined new urolithiasis patients upon their first visit to the University of Rochester Medical Center kidney stone clinic between February 2020 and November 2023, who completed a WISQOL questionnaire. Stone surgery information from May 2015 to November 2023 was also obtained. The study included nephrolithiasis patients who were 18 years or older and were proficient in English.
The primary outcome was the WISQOL score. QoL data were obtained from English versions of the validated 28-item WISQOL questionnaire on a 0 to 100 standardized scale, comprising a total HRQOL score and scores from four domains: social functioning, emotional functioning, impact of stone-related symptoms, and vitality. 12,13 Participants rated each survey question on a scale of 1 to 5, with higher scores indicating higher QoL. These questionnaires were provided through the electronic health record patient portal a week before scheduled appointments.
The overall score was stratified by the subscores of social functioning, emotional functioning, impact of stone-related symptoms, and vitality. The primary outcome was also stratified by symptomatic status of patients, determined by a specific question in the WISQOL questionnaire (Q8-2), which asked about patient-reported pain or symptoms related to kidney stones within the past 4 weeks. Demographic information collected included age at the time of the visit, gender, race, ethnicity, prior stone procedures, and medical history.
Statistical analysis
Univariate analyses comprising two-sample t-tests for continuous variables and chi-squared tests for categorical variables were conducted to explore differences between men and women based on their self-reported gender identity. WISQOL total scores and subdomains were compared between genders, both overall and after stratification by symptomatic status. The number of prior stone surgeries, including ureteroscopy (URS), extracorporeal shockwave lithotripsy (SWL), and percutaneous nephrolithotomy (PCNL), were also assessed for gender differences.
Psychosocial comorbidities, defined as having a medical diagnosis of depression, chronic pain (including fibromyalgia, arthritis, or interstitial cystitis), and substance use, were also assessed. Multivariate linear regression was conducted to analyze the impact of gender on WISQOL scores adjusting for age, symptomatic status, type of surgery, number of stone surgeries, and psychosocial comorbidities. Statistical significance was defined as p < 0.05. All statistical calculations were performed using Python 3.0 (python.org).
Results
The research encompassed 2199 patients with an average age of 58.1 ± 14.9 years. One thousand eighty-five (49.3%) were women. In the analysis, women were younger (55.6 ± 15.3 vs 60.6 ± 14.1; p < 0.001). There were no significant differences in distributions of race and ethnicity between genders. Demographics are shown in Table 1.
Demographics for 2199 Patients
Mean values are presented with the corresponding ±SD. p-Values represent results of two-sided Student's t-tests for continuous and chi-squared tests for dichotomous variables.
PCNL = percutaneous nephrolithotomy; SD = standard deviation; SWL = extracorporeal shockwave lithotripsy.
Female patients underwent 1440 stone procedures, whereas male patients underwent a collective total of 1396 stone procedures. A significant difference in the distribution of URS surgeries was observed between genders (p < 0.001), as well as in SWL (p < 0.001), but not in PCNL (p = 0.218). A higher percentage of women underwent URS, whereas a greater proportion of men underwent SWL.
However, there was no significant difference in total number of surgeries received (p = 0.312) or the frequency of surgeries (p = 0.344) between men and women. There was a significant difference in presence of a psychosocial comorbidity, with a higher proportion of women being found with conditions categorized as depression, chronic pain, or substance abuse (p < 0.001). This discrepancy was consistent across each individual category (p = 0.001). Complete results are shown in Table 1.
Wisconsin Stone Quality of Life Questionnaire
Women reported significantly lower WISQOL scores compared with men across all domains, including the WISQOL total score (71.6 ± 24.8 vs 80.7 ± 20.8; p < 0.001), and in the subdomains of social impact (80.2 ± 26.8 vs 86.9 ± 21.8; p < 0.001), emotional impact (67.3 ± 30.7 vs 77.1 ± 27.3; p < 0.001), disease impact (66.1 ± 29.1 vs 78.0 ± 23.2; p < 0.001), and impact vitality (62.6 ± 34.3 vs 72.9 ± 30.0; p < 0.001) as depicted in Figure 1. This association persisted upon stratified analysis of symptomatic (56.6 ± 24.1 vs 63.7 ± 23.5; p < 0.001) and asymptomatic (85.2 ± 17.6 vs 88.7 ± 13.8; p < 0.001) patients, as illustrated in Figure 2. Additional details can be found in Supplementary Table S1.
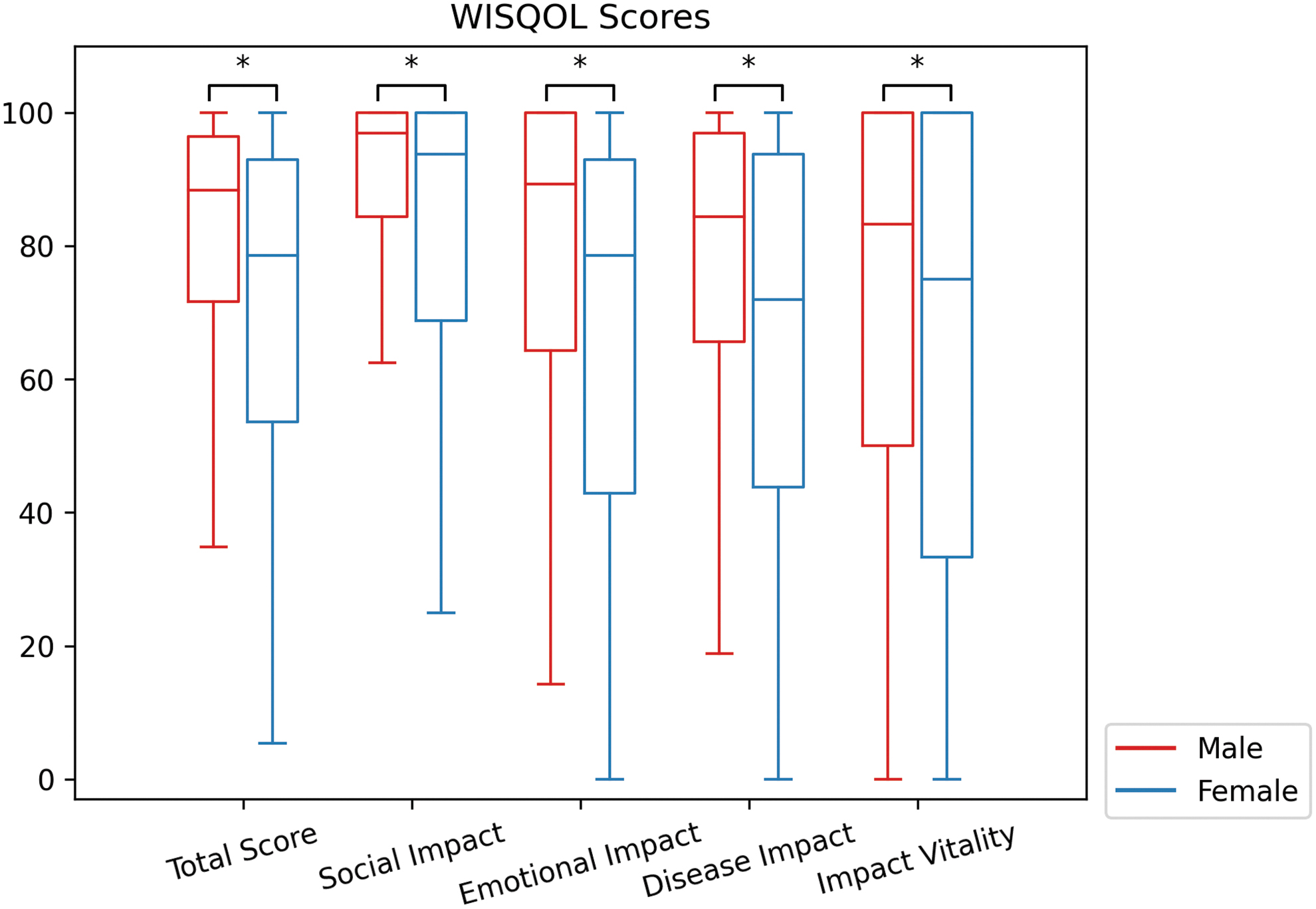
WISQOL scores between men (n = 1114) and women (n = 1085); scores are standardized from 0 to 100. Each box represents the IQR of scores for a cohort, with the median score denoted by the central line. Whiskers extend to the furthest scores within 1.5 IQR of the lower and upper quartiles. All p-values <0.001 with t-test. IQR = interquartile range; WISQOL = Wisconsin Stone Quality of Life Questionnaire.
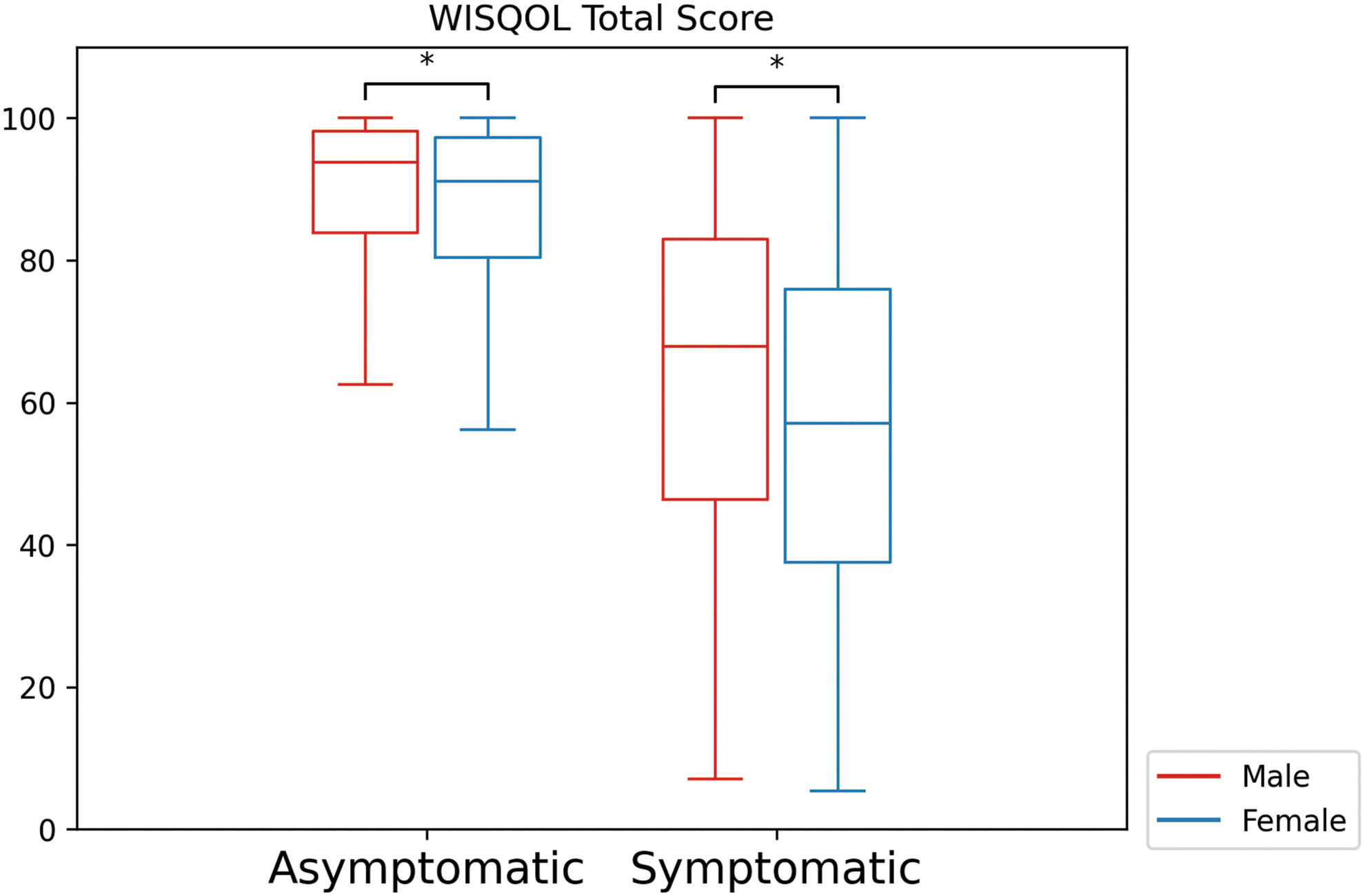
WISQOL total score between men (A: n = 697, S: n = 267) and women (A: n = 502, S: n = 399); scores are standardized from 0 to 100. Each box represents the IQR of scores for a cohort, with the median score denoted by the central line. Whiskers extend to the furthest scores within 1.5 IQR of the lower and upper quartiles. All p-values <0.001 with t-test.
Multivariate analysis
In the multivariate analysis, female gender emerged as an independent predictor of reduced WISQOL scores, showing a 3-point decline compared with male gender (β = −3.22; p < 0.001). In addition, age at encounter independently predicted improved WISQOL scores, indicating an ∼1-point increase for every 10 years older the subject was at their initial visit (β = 1.3 points/10 years; p = 0.001). Symptomatic status was indicative of lower scores, with symptomatic individuals experiencing a 26-point decrease in WISQOL score (β = −25.63; p < 0.001).
We examined various surgical procedures categorized by invasiveness, assigning PCNL a value of 3, URS a value of 2, SWL a value of 1, and no surgery a value of 0; however, the type of surgery was not found to be a predictor of WISQOL scores. The number of surgeries was an independent predictor of lower WISQOL scores, with a 1-point decrease for each additional surgery (β = −0.60; p = 0.001).
The presence of a psychosocial comorbidity also independently predicted lower WISQOL scores, with an 8-point decrease for the presence of a diagnosis (β = −8.10; p < 0.001). Although race and ethnicity were initially included in the multivariate analysis, they were excluded in the final model because of a lack of statistical significance. Complete results are presented in Table 2.
Multivariate Linear Regression for Predictors of Health-Related Quality of Life
CI = confidence interval.
Discussions
This study investigated gender disparities in HRQOL outcomes among kidney stone formers, utilizing the WISQOL. The findings revealed significant differences in HRQOL scores between men and women, with women consistently reporting lower scores across all domains.
The multivariate analysis identified female gender as an independent predictor of diminished WISQOL scores even after adjusting for age, symptomatic status, surgery type, surgery count, and presence of psychosocial comorbidities. The influence of age-related factors on HRQOL outcomes, as highlighted by the association with age at encounter with WISQOL scores, aligns with previous research. 5,11 Symptomatic status also remained a significant predictor of lower scores, emphasizing the need for gender-specific considerations in treatment and support strategies.
A notable aspect of our study was the exploration of stone procedures and their potential contribution to gender-based differences in HRQOL. Although the total number of surgeries did not differ significantly between genders, the distribution of specific procedures such as URS and SWL exhibited gender-related differences. The increased rate of an invasive procedure such as URS among female patients may be thought to be contributing factor to the worse WISQOL scores reported by women.
However, changes in surgical type were not responsible for differences in WISQOL score, suggesting that gender maintains an independent association with diminished QoL, which is not entirely accounted for by the specific type of surgery performed. The higher rates of depression, chronic pain, and substance abuse seen in women have been well studied and could be possible contributing factors to lower QoL scores in women. 14,15 However, our multivariate analysis showed a significant difference in QoL scores between men and women even when taking psychosocial factors into account.
The results of this study align with previous research indicating that women with kidney stones have decreased QoL compared with men with kidney stones. 3,10,11 Women were also found to be more likely to be readmitted to the emergency department and experience urinary sepsis post-URS. 16,17 The reasons behind this gender disparity remains complex and warrants further exploration, but these health differences are thought to be caused by a combination of social and biologic factors. Disparities in QoL between genders have been documented in other disease processes as well.
In colorectal cancer patients, women were shown to have lower HRQOL compared with men, particularly in physical and social functioning. 18,19 Among HIV patients, women reported significantly worse HRQOL in several domains. 20,21 The interactions between gender and diseases may result in different approaches to prevention, treatment, and coping with illness. 22
Several potential limitations warrant consideration in this study examining gender disparities in QoL outcomes among kidney stone formers. The retrospective design may hinder the establishment of causal relationships between gender and HRQOL. The collection of HRQOL data through the WISQOL at various phases of the patients' health care journey introduces increased variability. Survey-based data may introduce recall bias, affecting the accuracy of reported QoL scores.
The electronic distribution of the survey may introduce selection bias caused by potentially differential access to electronic surveys across levels of gender, age, education, and social support. The study's generalizability is limited to populations similar to the kidney stone clinic at the University of Rochester Medical Center since this is a single-center study. Moreover, the sample primarily comprised English-speaking patients, and the representation of diverse gender groups in the catchment area may be limited.
It is important to acknowledge that this study, conducted within a single institution and focusing on a specific cohort of kidney stone patients based on gender, provides initial insights. These findings highlight the gender disparities in HRQOL among kidney stone patients. However, further validation in larger and more diverse populations is warranted to enhance the robustness and general applicability of these insights.
Conclusions
The findings suggest that women with kidney stones experience lower HRQOL compared with men across all domains. This discrepancy persists even when patients report being asymptomatic. The exploration of stone procedures further elaborated on potential contributors to gender-based differences in HRQOL. By recognizing the unique challenges and concerns faced by men and women with kidney stones, health care professionals can optimize patient care and improve overall HRQOL for individuals with kidney stones.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: study conception and design by S.O.Q. and R.K.J.; data collection by D.Y.S. and S.O.Q.; analysis and interpretation of results by D.Y.S. and C.C.; draft article preparation by D.Y.S., C.C., and V.S.; all authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.