
Abstract
Purpose:
To assess the effectiveness and pain intensity associated with magnetic ureteral stent removal using a retriever, without the aid of ultrasound guidance.
Methods:
We prospectively enrolled 100 patients who underwent retrograde rigid and flexible ureterorenoscopy with or without laser lithotripsy for ureteronephrolithiasis treatment from September 2021 to June 2023. These patients were assigned in two groups. Group 1 underwent the traditional ureteral stent insertion, while Group 2 underwent magnetic ureteral stent insertion. Both insertion and removal times were documented. The indwelling time for ureteral stents was 14 days. One group underwent stent removal via flexible cystoscopy using grasping forceps and the other group using just a magnetic retriever, without the aid of ultrasound guidance. The numeric pain rating scale, recommendation rate, and a standardized self-answered ureter stent symptoms questionnaire (USSQ) were obtained directly after stent removal.
Results:
Both groups presented comparable characteristics in factors such as age, body mass index, history of stone treatments, procedure type, and complication rates during and post-surgery. Time taken for ureteral stent insertion did not differ significantly between the groups (131.2 seconds for Group 1 vs 159.1 seconds for Group 2). However, the stent removal time (152.1 seconds for Group 1 vs 35.4 seconds for Group 2) and pain intensity (6 for Group 1 vs 2 for Group 2) were significantly lower for Group 2. Furthermore, five out of the six sections of the USSQ showed significantly better results for Group 2.
Conclusions:
The use of magnetic ureteral stents, as a safe and efficient alternative to conventional ureteral stents, not only eliminates the need for cystoscopy but also conserves resources and reduces patient discomfort.
Introduction
Double-J (DJ) stents, first introduced in 1978 as prosthetic device, have emerged as an indispensable urologist’s tool for treating a wide array of urologic conditions. 1 They can serve as a method for passive preoperative ureteral dilatation 2 and can also help reduce temporary postoperative blockages in the ureter caused by trauma, retained dust, clot, and stone fragments. 3 In recent years, ureteral stents have seen design, material, and covering modifications to enhance stent-related symptoms and biocompatibility. 4 Innovations also include varied stent removal methods such as strings, spiral-ending devices, and magnetic retrievers, aiming to simplify removal and reduce symptoms in outpatient settings. 5,6 Traditionally, the ureteral stents were removed using a rigid cystoscope and forceps under local anesthesia, which can be painful and risk urethral injury in men. This procedure was also associated with unavoidable sterilization costs. 7 Flexible cystoscopy with reusable or single-use endoscopes has offered an alternative but comes at a higher cost, even when using instruments with a built-in grasper. 8 Furthermore, some authors have stated that up to 64% of patients experienced bothersome periprocedural urinary symptoms during DJ stent removal using flexible devices. 9 Given the challenges and limitations of existing methods, the need for innovative solutions became more pronounced.
We report a single center observational study to assess the effectiveness and pain intensity associated with magnetic ureteral stent removal using a retriever, without the aid of ultrasound guidance.
Materials and Methods
Inclusion criteria: adult female and adult male patients, with planned retrograde rigid and flexible ureterorenoscopy (rURS and fURS) with or without laser lithotripsy for ureteronephrolithiasis treatment, who received a DJ as presenting at least 4 weeks before the procedure and where a post-interventional ureteral stent placement was indicated. Sterile urine culture.
Exclusion criteria: patients who underwent antegrade stone treatment or primary URS, as well as patients who were treated with alpha-blocker/antimuscarinic monotherapy or combination therapy of aforementioned. Patients who received a single-J catheter after the procedure.
From September 2021 to June 2023, the eligible patients were prospectively evaluated and assigned into two groups at 1:1 ratio. We specifically included patients for whom anatomically inserting a 28 cm long stent was acceptable, aiming to ensure a homogeneous group without stent size variation. This decision was influenced by the fact that previously published work on this topic defined 7 Charr./28 cm as the standard stent size. Group 1, the control group, consisted of patients who underwent the conventional ureteral stent insertion, 7 Fr/28 cm DJ stent (Coloplast, Denmark). The stent was removed on day 14 using a flexible cystoscope (Richard-Wolf, Germany) with an atraumatic, 15 Fr beveled distal tip. Group 2 consisted of patients who underwent magnetic ureteral stent insertion, 7 Fr/28 cm (Urotech, Germany), which features a strategically placed 9 Fr cylindrical magnet at its bladder end fixed to the stent with a nonabsorbable thread (Fig. 1a, 1b). The stent was removed on day 14 using the 15 Fr magnetic retriever, which connects with the cylindrical magnet of the stent and comes with the ureteral stent in the package (Fig. 1c, 1d). All patients received preoperative single-shot surgical antibiotic prophylaxis with second-generation cephalosporin and the same equipment (laser device, reusable semi-rURS devices, access sheaths, single-use fURS devices, guide wires) was used. All procedures were performed or supervised by a senior surgeon.
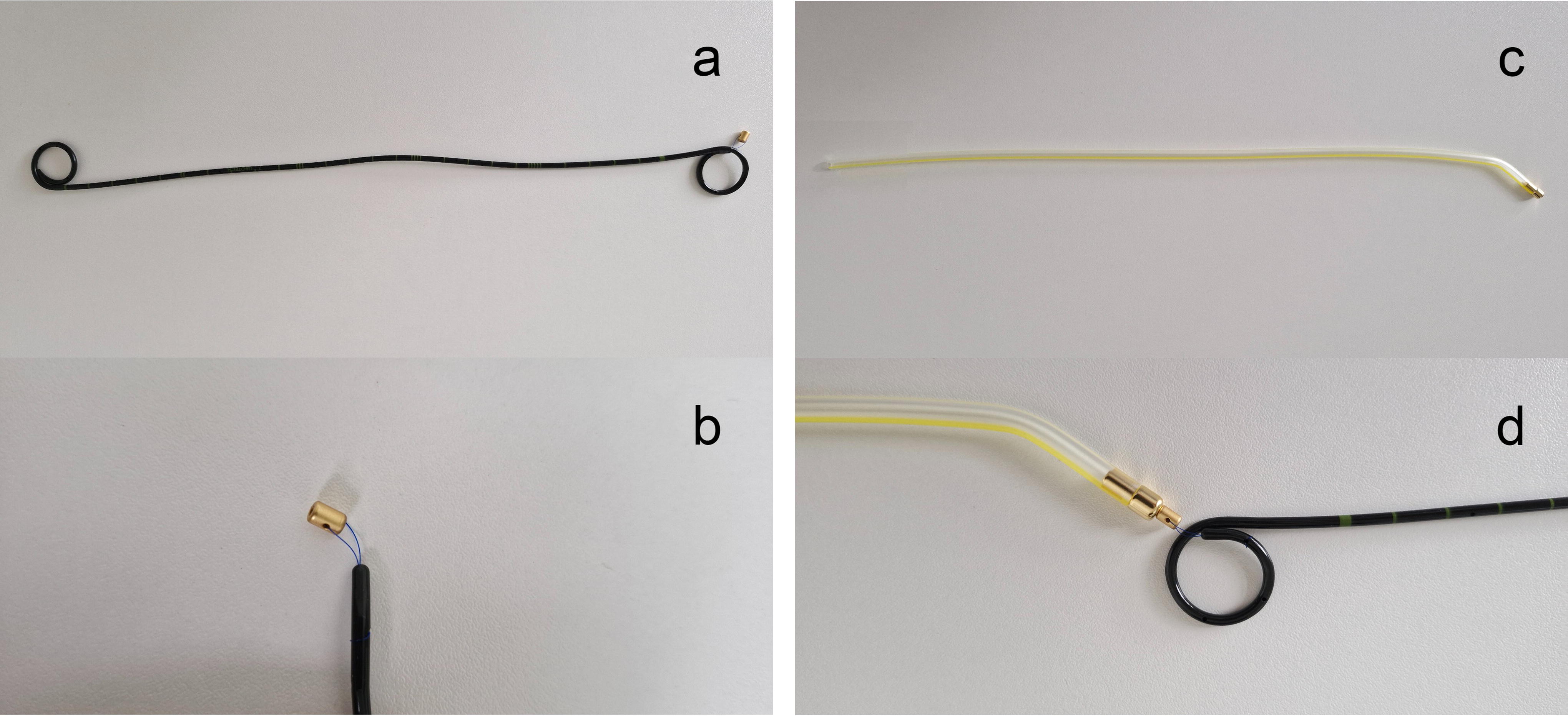
Magnetic ureteral stent and retriever.
Both procedures for stent removal were performed as endoscopy room-based outpatient procedure under local anesthesia and without antibiotic prophylaxis. For Group 1, the flexible cystoscopy was performed after applying sterile lubricant with local anesthetic and disinfecting properties (Instillagel), the distal tip of the stent was grabbed using the reusable metal grasper, and the stent was removed under vision. For Group 2, the magnet retriever was inserted in the bladder after applying sterile lubricant with local anesthetic and disinfecting properties (Instillagel), and the Tiemann device tip was rotated in the direction of the ureteral orifice of the treated side. When the connection of the magnetic parts is successful, a confirmation sound is heard and a light-tactile-feedback is felt. No additional aid of ultrasound guidance was applied. With the removal of the retractor, the connected magnetic DJ stent was also removed. Both insertion and removal times were documented using a stopwatch. The time taken for stent insertion was determined from the moment the guide wire was positioned until the DJ was disconnected from the pusher. The time for stent removal was measured from the application of the lubricant to the point when the DJ was extracted from the distal urethra. The NRS is a segmented numeric version of the visual analog scale in which a respondent selects a whole number (0, no pain–10, worst pain imaginable) that best reflects the intensity of experienced pain. Our patients were asked to indicate the numeric value on the graphically segmented scale that best described their pain intensity during the stent removal. Recommendation rate was calculated based on the answers to a hypothetical y/n question formulated as: “If you had to undergo another stone treatment and needed a postoperative ureteral stent, based on your experience, would you recommend the use of this conventional/magnetic ureteral stent?” Finally, a standardized self-answered USSQ was obtained. SPSS v23 was used for statistical analysis, descriptive statistics, and data visualization. The significance level was set at 0.05. The local ethics committee (F-2021-112) approved this study. The study was registered at www.bfarm.de, German federal institute for drugs and medical devices (DRKS00025985).
Results
A total of 100 patients were included in the analysis. As depicted in Table 1, no statistically significant differences were observed in demographics, types of surgical procedures, and intra- and postoperative complications. Similarly, when comparing the patient groups, there were no significant differences in gender, age, body mass index (BMI), or history of stone treatment. Time taken for ureteral stent insertion was shorter for Group 1, though the difference was not statistically significant (131.2 seconds for Group 1 vs 159.1 seconds for Group 2, p = 0.21) as shown in Figure 2. A comparison of ureteral stent removal time, however, showed a statistically significant difference in favor of Group 2 (152.1 seconds for Group 1 vs 35.4 seconds for Group 2, p < 0.001, Fig. 3). Furthermore, a significantly lower NRS score (6 for Group 1 vs 2 for Group 2, Fig. 4) and higher recommendation rate (32.8% for Group 1 and 94.0% for Group 2) were also documented in favor of Group 2. The statistical difference remained even when the groups were further stratified based on gender, as represented in Table 2. Finally, the USSQ comparison showed significant differences between the two groups in the “urinary symptoms,” “body pain,” “general health score,” and “work performance” sections (p < 0.001) as well as in the “sexual matters” section (p = 0.01), as demonstrated in Table 3. The only section where no differences were observed was the “additional problems” section (p = 0.06). The estimated marginal means of each section are shown in Figure 5.
Patient Characteristics
BMI = body mass index; rURS = rigid ureterorenoscopy; fURS = flexible ureterorenoscopy; UTI = urinary tract infection.
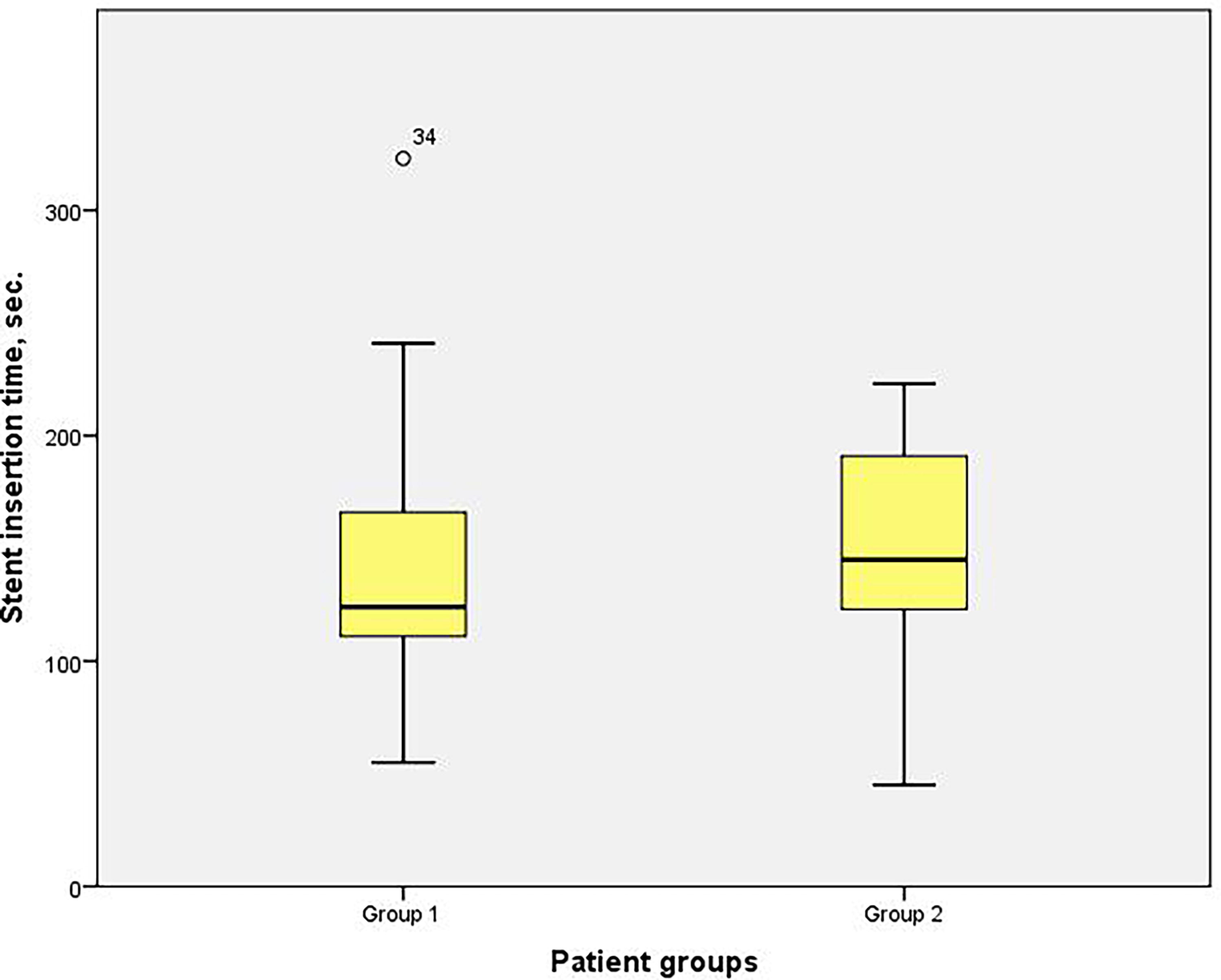
Stent insertion time.
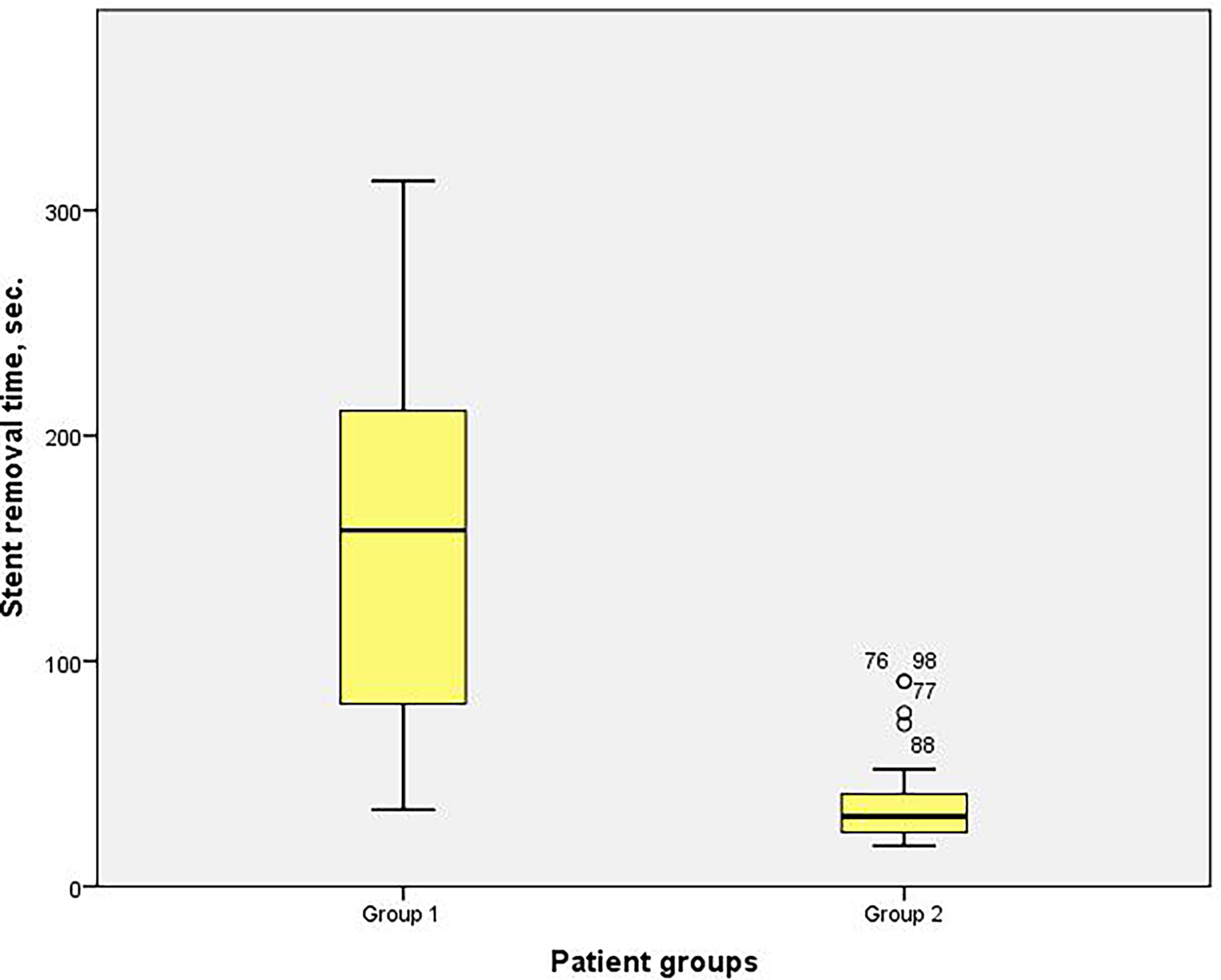
Stent removal time.

Numeric pain rating scale, distribution among groups.
Stent Insertion- and Removal Time, Pain Scale and Recommendation Rate
NRS = numeric pain rating scale.
USSQ Components
USSQ = ureter stent symptoms questionnaire; IQR = interquartile range; SD = standard deviation.

USSQ components. USSQ = ureter stent symptoms questionnaire.
Discussion
Although ureteral stents have been widely used in endoscopic urology since their introduction a couple of decades ago, the exact timing of postoperative removal remains ambiguous. A ureteral stent, being a foreign body, is a potential source of infection and should be removed in a timely manner. While clinical practice typically sees removal within 3 to 30 days, 2,9,10 we opted for the median time. Thus, for logistical purposes and structured follow-up, we set the indwelling stent time at 14 days. Despite numerous technical advancements, a significant proportion of patients continue to experience stent-related symptoms. 9 The traditional method for stent retrieval involves using the widely available reusable rigid cystoscopes and grasping forceps, which can be painful, risk urethral injury in men, and comes with unavoidable sterilization costs. 7 Flexible cystoscopy with reusable or single-use endoscopes has offered an alternative but comes at a higher cost, even when using instruments with a built-in grasper. 8 The escalating cost of these instruments limits their availability in many parts of the world. 2 The stent removal procedure is perceived as highly uncomfortable, particularly as general anesthesia is increasingly omitted in the outpatient setting to conserve cost-intensive operating resources. 11 A potential alternative is employing non-endoscopic techniques for stent removal under local anesthesia, which would not strain operating room resources and several such methods have been detailed. Extraction strings, wire loops, crochet hook—such as retrievers and spiral devices have been examined but to date not widely used. 2,12
While the concept of a magnetic ureteral stent first surfaced in the 1990s, the recent development of stents with a magnetic tip at the distal end represents a pivotal leap forward in endourology. Although several studies compared magnetic stent removal time with cystoscopic stent removal time, 9,13 the literature on the stent insertion time is scarce. We found that the insertion time of magnetic stents was slightly longer, but not statistically significant (p = 0.21) in both female and male patients. This likely stems from the requirement to accurately position the guide wire through the hole in the stent’s magnetic tip. Furthermore, we report stent removal time significantly shorter for Group 2 in both female and male patients (152.1 seconds for Group 1 vs 35.4 seconds for Group 2, p < 0.001). Some authors reported similar findings, however only for male patients and not stratified by gender. 2,13 Others have reported high stent removal success rates for magnetic stents, varying from 86% to 96%. 14,15 We reported a removal success rate of 100% for both groups, with prostate size, presence of prostate middle lobe and patient discomfort being named as the main reasons for prolonged removal time. Even with ultrasound guidance, the magnetic stent removal procedure without prior preparation can take between 1 and 4 minutes in adults 2 and between 1 and 10 minutes in children. 16 We chose not to use ultrasound during magnetic stent removal to assess the potential for the procedure to be performed by nonmedical personnel in the future. Although we showed that stent removal without ultrasound guidance is feasible with very high success rates, the stent removal in our study was indeed carried out by our residents. All procedures of stent removal using the magnetic device were successful. We have encountered problems in six male patients with intravesical prostate middle lobe (removal time >70 seconds). The retractor necessitated reciprocating movements both longitudinally and laterally, requiring adjustments in both clockwise and counterclockwise directions until the connection was established.
Some authors demonstrated that the mean time for blind magnetic stent removal, including preparation and the procedure itself, was 9.55 minutes. 13 We cannot draw parallels with these findings as we did not separately document the preparation time. Regarding both preparation and turnaround time, commonly defined as the overall time needed to clean and prepare the examination room for the subsequent procedure, we believe that the time discrepancy between the two procedures (cystoscopy vs magnetic retractor) is evident.
Moreover, our findings indicate that the removal of magnetic stents is considerably quicker and less discomforting to patients compared with the traditional stent removal via cystoscopy, as stated by some authors. 9 The drawback, however, is that MRI imaging must be avoided during the stent indwelling time and this should be communicated clearly to patients before the procedure and potential insertion of a magnetic stent. A negative correlation between NRS and recommendation rate for conventional DJ stents was also observed.
In addition, the cost of disposable materials per procedure remains a top concern for many hospitals. When comparing the cost of disposable materials per cystoscopy, estimated at around $22, 17 with the cost of disposable materials associated with magnetic stent removal, namely, a sterile lubricant with anesthetic and disinfectant properties priced at roughly $2, the disparity is substantial. Same authors have stated that depending on the annual procedure volume and the range of available cystoscopes, the total cost per cystoscopic DJ removal fluctuates between $243 and $420, 17 with capital purchase cost accounting for most of the variation. These results from an American center are similar to results published from a European center, where the total cost, urologist and nurse included; per DJ removal, using a single-use cystoscope with an integrated grasper, was €361. 18 In high-volume endourology centers, the total cost per procedure can be reduced when utilizing single-use flexible cystoscopes with integrated graspers. It has been estimated by some researchers that the cost benefit favors reusable cystoscopes after a break-even point of 704 stent removals annually. 19
Unfortunately, we were not able to carry out a comprehensive analysis of the total cost per procedure using reusable flexible cystoscopies and graspers owing to lack of data for variables such as the exact time spent during tasks performed by both nurses and urologists. Nevertheless, we managed to estimate the cost of disposable materials for this procedure at approximately €15. In addition, the costs for decontamination and sterilization of cystoscopes and graspers, excluding transport, were estimated at roughly €36 and €22, respectively.
While the initial investment for the magnetic DJ catheter is estimated to be roughly 50% higher than that of a conventional DJ (33€) catheter, the costs are offset by the inclusion of the magnetic stent retriever in the package and the elimination of additional expenses for high-priced cystoscopic stent removal. Finally, when comparing the USSQ sections, we found significant differences between the two groups in the “urinary symptoms,” “body pain,” “general health score,” and “work performance” sections (p < 0.001) as well as in the “sexual matters” section (p = 0.01), favoring the magnetic stents. Unlike some authors, 13 we did not observe increased instances of lower abdominal pain or bladder irritation in patients with magnetic stents. While the diameter of the stent is the focal point in most research, its length frequently goes unmentioned. 9,13,14 We reported no discrepancies in either stent length or diameter across all patients, irrespective of size or gender. Thus, if stent length or diameter were to irritate the bladder and therefore influence the USSQ results, it would affect both groups equally.
We recognize the limitations of our study, including its single-center nature, small sample size, lack of data on ethnicity, and absence of randomization. In real-world contexts with diverse health profiles, strict randomization can lead to unrepresentative or ambiguous groups, considering the sample size. Therefore, we used careful matching and stratification to balance key confounding variables, minimizing potential bias in our findings. As a result, we observed no statistically significant differences between the groups in demographics, surgical procedure types, complication rates, BMI, or history of stone treatment. The observed power of 0.91 is adequate to identify a genuine difference or effect present in this study population.
Being among the first hospitals in northwest Baden-Württemberg to introduce magnetic stents, a significant portion of our patients has a clear preference towards certain stent types, potentially limiting their study participation if their preferred choice is not met.
Conclusions
The utilization of magnetic ureteral stents has emerged as a reliable and effective alternative to traditional ureteral stents. One of the primary benefits of this approach is the elimination of the necessity for cystoscopy, a procedure that can be both resource-intensive and uncomfortable for patients. In addition, adopting magnetic stents conserves valuable medical resources, potentially reducing costs. Moreover, patients benefit from decreased discomfort and potential risks associated with more invasive procedures.
Footnotes
Acknowledgments
The authors would hereby like to thank Doris Busch and Anita Lein for the material cost analysis.
Authors‧ Contributions
S.M.: conceptualization, formal analysis, methodology, project administration, supervision, visualization, writing—original draft preparation, writing—review and editing. W.L.: project administration, investigation, writing—review and editing. W.T.: data curation, investigation. M.J.: data curation, investigation. S.B.: data curation, investigation.
Author Disclosure Statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.
Funding Information
No funds or grants were received for this project.