
Abstract
Background:
Postoperative stress urinary incontinence (SUI) after Holmium Laser Enucleation of the Prostate (HoLEP) has improved with the early apical release (EAR) technique. However, some patients develop SUI despite using EAR HoLEP. The aim of this study is to investigate whether a novel classification of the external sphincter is correlated with postoperative SUI.
Methods:
The data of 98 patients who underwent EAR HoLEP for benign prostatic hyperplasia were prospectively analyzed. We propose a novel endoscopic classification of external sphincter appearance after HoLEP graded from 0 (best preserved) to 3 (most degraded). Patients were followed for 6 months postoperatively and administered validated questionnaires. A logistic regression was performed to compare moderate SUI rates at sphincter grade 3, controlling for age, obesity, catheter dependency, and grams resected at 6 weeks and 3 months.
Results:
The sphincter grades included 6 grade 0, 47 grade 1, 30 grade 2, and 15 grade 3. Patients were divided into a group without SUI (n = 51), and a group with SUI (n = 47) at 6 weeks postoperatively by International Consultation on Incontinence Questionnaire (ICIQ). Patients with reported SUI on ICIQ were more likely to have sphincter grades ≥2 at 6 weeks (p= 0.001) and 3 months (p < 0.0001). At 6 months, persistent SUI was associated with sphincter grade 3 (p < 0.0001). Logistic regression demonstrated that sphincter grade 3 was associated with clinically significant SUI at 3 months (p < 0.01).
Conclusions:
Lower sphincter grades are associated with improved return of continence after EAR HoLEP.
Introduction
Holmium laser enucleation of the prostate (HoLEP) is endorsed by the AUA guidelines as a size-independent surgery for the treatment of benign prostatic hyperplasia (BPH). 1 HoLEP has been designated as the new gold standard for BPH surgery. 2 HoLEP was originally described using a two- or three-lobe technique. 3 A limitation of the traditional technique was postoperative stress urinary incontinence (SUI), which ranged between 1.3 and 44%. 4,5 Multiple prior studies have investigated risk factors for the development of transient postoperative SUI, which include prostate size >100 g, catheter dependence, obesity, and age. 6 –8 Recently, early apical release (EAR) techniques have emerged, demonstrating improved continence rates in the first three months postoperatively. 9,10
Despite the advantages of EAR HoLEP, some patients still experience transient SUI. The aim of this study was to correlate the preservation of the prostatic apex with SUI rates. We prospectively evaluated the prostate apex appearance after EAR HoLEP. As a result of these observations, we established a novel classification system of external sphincter preservation following HoLEP. When this study was designed and written, no external sphincter classification of endoscopic injury was available.
Materials and Methods
Patients and surgical procedure
Ninety-eight patients who had HoLEP for BPH between April 2023 and October 2023 were recorded prospectively. All HoLEPs featured trainee involvement with attending physician supervision. EAR was performed by senior residents, fellows, and attending consultants. Patients with a history of prostate cancer, bladder cancer, undergoing holmium laser ablation of prostate, and median lobe-only holmium laser enucleation were excluded. All included patients had sterile urine cultures before surgery. The demographic characteristics of the patients, including age, body mass index (BMI), medical history, uroflow, and prostate volume were recorded (Table 1). All patients underwent EAR HoLEP as described previously. 10
Baseline Characteristics
t-test.
Chi-squared test.
Mean ICIQ was 0.76 in the no postop SUI, and 1.45 with postop SUI group, but not accounted for by SUI.
SUI defined by any ICIQ >0 and SUI type incontinence at 6 weeks.
Bold values denote statistical significance.
AUASS, AUA Symptom Score; AUASS QoL, AUA Symptom Score Quality of Life; SHIM, Sexual Health Inventory for Men Questionnaire; ICIQ, International Consultation on Incontinence Questionnaire Short Form; IQR, Interquartile Range.
Sphincter grading classification system and postoperative follow-up
At the conclusion of the surgery before catheter placement, multiple high-resolution photographs were obtained visualizing the prostatic apical dissection. Four grades of apical appearance following HoLEP were defined based on external sphincter anatomy. According to this grading system, grade 0 demonstrates unblemished mucosa, grade 1 is urethral sphincter mucosal denudation without violation or tear of the layer, grade 2 is a lateral tear distal to the apical cut edge with mucosal layer violation, and grade 3 is an anterior tear with mucosal layer violation (Figs. 1 and 2). The external sphincter complex travels distally from the mid prostate anteriorly and forms a horseshoe distal to the verumontanum (Fig. 2). Any violation of the mucosal layer at the apical portion of HoLEP dissection introduces the risk of temporary incontinence. Deep lateral mucosal tears into the bulbar urethra may impact the external sphincter complex. The anterior portion of the sphincter complex, would be most concerning for deleterious impact on continence. The longitudinal fibers of the sphincter run closest to the prostatic urethra anteriorly near the apex. Grades were assigned after review of the photographs by an initial grader with 2 additional blinded endourologists. The final grade was designated by the highest (worst) sphincter score among the graders.
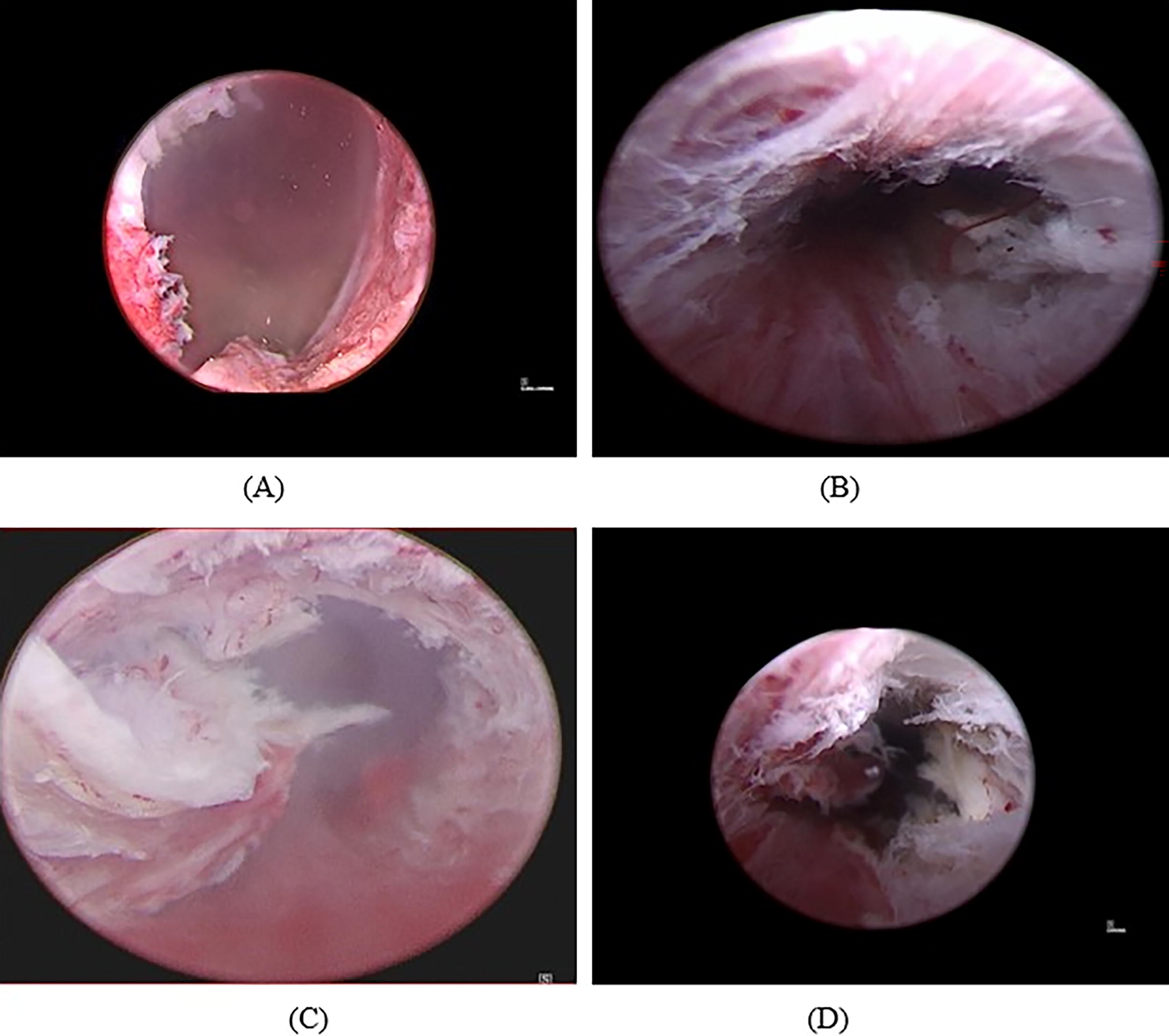
This represents a sample of the different sphincter grades seen at the aftermath of EAR HoLEPs.

This represents an outline of the external urethral sphincter on cross-sectional imaging and endoscopically before and after HoLEP.
Patients were followed for at least 6 months postoperatively. Patients were administered validated questionnaires, including American Urological Association Symptom Score (AUASS), American Urological Association Quality of Life Index (AUASS QoL), International Consultation on Incontinence Questionnaire Short Form (ICIQ), and incontinence type. Additionally, total pads per day and postoperative complications were recorded. Moderate SUI was defined by ICIQ ≥8 based on the definition Soto-González et al. described in a postprostatectomy cohort. 11 Stress urinary incontinence was defined by patient report and selection of any stress incontinence option on question 6 of the ICIQ.
Statistical analysis
Statistical analysis was performed with SPSS (version 29.0, Chicago, IL). Continuous variables are expressed as mean (Standard Deviation) or median [interquartile range], and categorical variables are presented as absolute numbers and percentages. The t-tests and chi-squared analyses were used to evaluate continuous and categorical variables, respectively. A logistic regression model was used to assess the statistical significance of a grade 3 injury on the development of moderate postoperative SUI at 6 weeks and 3 months in a multivariable setting. Moderate SUI was defined as patients with SUI and ICIQ ≥8. 11 Prostate size of 120 g and age greater than 65 were used as categorical variables controlled in the regression model due to prior publication as independent risk factors for postoperative SUI. 4,7 Obesity and catheter dependence were controlled in the logistic regression as well. Results were considered significant at p < 0.05.
Results
The patients were divided into two groups as patients without SUI (n = 51) and with SUI (n = 47) as determined by ICIQ at 6 weeks. Baseline preoperative data demonstrated no significant differences between either groups (Table 1). The sphincter grades included 6 grade 0, 47 grade 1, 30 grade 2, and 15 grade 3.
At 6 weeks postoperatively, patients with SUI had higher AUASS (p = 0.016) and used more pads per day (p < 0.001). The SUI cohort had higher sphincter grades and were more likely to have a grade 2 or higher sphincter score (Table 2, p = 0.001). There was no difference in postoperative adverse events between groups (Table 2, p = 0.302).
Perioperative and Postoperative Outcomes
t-test.
Chi-squared test.
Bold values denote statistical significance.
AUASS, AUA Symptom Score; AUASS QoL, AUA Symptom Score Quality of Life; SHIM, Sexual Health Inventory for Men Questionnaire; ICIQ, International Consultation on Incontinence Questionnaire Short Form; IQR, Interquartile Range.
By 3 months postoperatively, 22 of the 47 patients with SUI at 6 weeks had full recovery of continence. The 25 patients with persistent SUI were more likely to have sphincter grade 3 (Table 3, p < 0.0001). Logistic regression demonstrated that after controlling for age, obesity, catheter dependence, and prostate volume, a grade 0–2 sphincter has a 42% risk reduction of developing clinically significant SUI at 3 months (Table 4). At 6 months postoperatively, of the 14 patients with SUI, 11 (78%) had a grade 3 sphincter (Table 3, p < 0.0001).
Sphincter Grades and Stress Incontinence at 3 and 6 Months
Chi-Squared Test.
At 3 and 6 months, a higher sphincter grade is associated with an increased risk of postoperative stress urinary incontinence.
Logistic regression performed controlling for age >65 age, obesity, catheter dependence, and prostate volume >120cc at 3 months. Clinically significant SUI was defined by ICIQ ≥8 and SUI-type incontinence. Patients with grades 0–2 sphincter had a 42% risk reduction of developing clinically significant SUI at 3 months. Bold values denote statistical significance.
The inter-rater agreement percentage was calculated at 93%. Of the 8 patients with discordance in evaluation, 50% were disagreements between 0 and 1.
Discussion
HoLEP is considered a versatile BPH surgery due to its minimally invasive nature, size independence, and few contraindications. 1 Despite these advantages, transient SUI represents a common aftereffect. 4,5 EAR techniques have been proposed as a solution to mitigate the risk of developing postoperative SUI. 10,12,13 Despite the adoption of EAR technique for all HoLEPs performed at our institution, some patients still experience postoperative SUI. Prior studies have investigated the classical trilobar HoLEP technique and identified several risk factors for the development of transient SUI, which include prostate size >100 g, catheter dependence, obesity, and age. 6 –8 In a subgroup analysis of prior data, which utilized EAR HoLEP, SUI was not associated with age, prostate size, or medical comorbidities. 10 We sought to evaluate whether the graded appearance of the prostatic apex after EAR HoLEP, defined as sphincter grades 0–3, could predict postoperative SUI.
Traxer and Thomas described a grading system to evaluate injuries that occur during ureteral access sheath placement. 14 Ureteral injuries were graded into 5 groups (grades 0–4) according to the involved layer. The sphincter grading system was modeled after the ureteral injury system with the incorporation of local anatomical principles.
The main continence control in men comes from the internal urethral sphincter, which is disrupted during tissue debulking BPH surgery. 15 The external urinary sphincter is the remaining continence mechanism after tissue debulking BPH surgery. There have been anatomical and histological studies to evaluate the external urinary sphincter, which helped guide our grading system. The rhabdosphincter has been defined as a vertical muscle lateral and ventral to the prostate and membranous urethra extending from the perineal body toward the bladder neck. The caudal fibers of the rhabdosphincter are arranged in an omega shape ventral and lateral to the urethra. The perineal body region is where the two limbs of the rhabdosphincter insert after traveling around the urethra. 16 In adult men, the rhabdosphincter muscle loses the striated muscle present in youth and is replaced by connective tissue and nonstriated muscle. 16 Therefore, a lateral tear distal to the prostate apex was defined as a grade 2 sphincter, and a grade 3 sphincter was defined as distal, anterior tears. For the external sphincter to adequately compress the urethra to prevent fluid leakage, the force of the sphincter contraction needs to transmute through some anterior BPH and connective tissue and create a water-tight seal from circumferentially intact mucosa. We believe this creates the coaptation and seal from the verumontanum extending distally. To spare this, it can be helpful to maintain a very small amount of adenoma anteriorly at the apex. There are some techniques which demonstrate this sparing anteriorly, but this must be tempered by the need to mitigate leaving behind extensive nodularity, which could cause obstruction in the future. Furthermore, when challenged by multinodularity, these techniques, which spare anterior tissue apically, can leave a significant amount of BPH behind. The most severe incontinence in patients was seen in grade 3 injuries, which involves anterior and distal tears at the apex, which may involve the “omega-shaped” portion of the rhabdosphincter. To our knowledge, this is a novel endoscopic grading system created to evaluate the external urethral sphincter after transurethral surgery.
We suspect that early apical release promotes continence through several mechanisms, including the preservation of a water tight seal of the mucosa around the sphincter, and decreasing damage to the external sphincter complex by limiting traction injury with early mucosal detachment. High-grade injuries can occur with poor technique, challenging surgical planes, increased apical vascularity with severe hematuria, and apical multinodularity.
Transient SUI rates after simple prostatectomy and transurethral resection of the prostate (TURP) are lower than HoLEP. 17,18 By 12 months, the follow-up results are comparable. HoLEP is associated with shorter catheterization times, hospital stay, and lower costs than both TURP or simple prostatectomy. 17,18 While the results from this study show a high overall transient incontinence rate, this was because the presence of SUI was based on ICIQ rather than patient-reported yes or no, pads per day, or pad weight. There can be a discordance between ICIQ report and incontinence urine volume by pad weight. 11 Patients with SUI at 3 months had a median pad use of 1 pad per day and had overall equivalent AUASS QoL scores between groups. EAR does improve SUI rates and severity. 10 This study demonstrates higher reported SUI rates due to the introduction of trainees to the relatively novel EAR technique. We have since started to shift to minimizing blunt technique at the apex until sufficient laser-induced mucosal detachment has occurred, which has reduced traction injuries. Additionally, we have implemented a higher tolerance for intentionally sparing a very small amount of adenoma anteriorly at the apex based on the results from this study, which has anecdotally yielded further improved continence after surgery.
One of the major limitations of this study is the grading system validation by 3 urologists at a single institution. We anticipate a future validation study with multicenter inter-rater assessment of this novel grading system. The surgical procedures were performed by different surgeons with trainee support of varying experience levels. Multicenter studies with a larger cohort of patients would ultimately show the value of this grading system, with the potential for adaption to other transurethral BPH surgeries. Our study is valuable because it is an initial study demonstrating the possibility of employing a grading system at the prostatic apex with the application of potentially predicting SUI outcomes.
Conclusion
The sphincter grading system can be used for standardized reporting of external sphincter appearance after transurethral procedures. Lower sphincter grades are associated with a faster return of continence after HoLEP.
Footnotes
Acknowledgments
The authors thank to to Justin Campagna, Jeffrey Stagg, and Nathaneal Oswald for their constructive feedback and collaboration, which were an invaluable asset to this project.
Authors’ Contributions
D.J.H.: Project development, data collection, data analysis, and article writing. C.B.: Data collection and data analysis. M.C.: Data analysis. M.N.: Data Analysis. M.R.H.: Article writing. S.M.C.: Project development and article writing.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.