
Abstract
Introduction and Hypothesis:
Robot-assisted radical nephroureterectomy (RANU) has emerged as a valid alternative to open or laparoscopic nephroureterectomy in recent years. However, different types of robotic platforms can limit surgical maneuvers in various ways. This study aimed to describe the surgical procedure and demonstrate RANU’s technical feasibility and safety using the Hugo robot-assisted surgery (RAS) system.
Materials and Methods:
Using the Hugo RAS system, we reported data from the first five consecutive patients who underwent RANU at Tottori University Hospital. We adjusted the docking angles of the four independent arm carts in each case and performed a complete RANU via a transperitoneal approach. We collected patients’ sociodemographic and perioperative data, including complications, and compared them retrospectively with data obtained using the da Vinci surgical system.
Results:
Arms positions were modified after the first patient to be placed all at the back of the patient. Median overall operative time was 283 minutes (203–377) and the median time using the robotic system was 187 minutes (121–277). The median estimated blood loss was 20 mL (5–155). None of the patients required a blood transfusion and none suffered postoperative complications of Clavien–Dindo grade ≥3. These outcomes were similar to those obtained with the da Vinci Xi system.
Conclusion:
This series represents the first report of RANU executed using the novel Hugo RAS system. Our proposed arm-setup will assist other surgeons and help ensure safe implementation of RANU on the Hugo platform.
Introduction
Upper urinary tract urothelial carcinoma (UTUC) is relatively rare, constituting 5–10% of urothelial carcinomas. 1,2 The European Association of Urology guidelines classify UTUC into low- and high-risk groups. Kidney-sparing management has become acceptable for patients meeting the UTUC criteria, including low-risk patients, those with lower ureteral cancer, and patients with a solitary kidney. 2 In high-risk UTUC (tumors >2 cm, high-grade cases, and cases with multiple tumors) radical nephroureterectomy (RNU) remains the gold standard. 2
Minimally invasive surgery in this field has become the norm, with a shift from open RNU to laparoscopic radical nephroureterectomy (LNU) and robot-assisted radical nephroureterectomy (RANU), with increased robot-assisted surgery (RAS). 3 In a comparison of open RNU and LNU, a systematic review has reported that LNU has a longer operative time, shorter hospital stay, and lower blood loss and transfusion rates. 4 A systematic review comparing RANU and LNU reported fewer complications and shorter hospital stays with RANU, but longer operating times. 5 RANU is safe and effective, with similar survival rates to the open approach. 6
Traditionally, the da Vinci surgical system’s Si, X, and Xi models (Intuitive Surgical Inc.) have been utilized for RANU. 6 –9 However, new surgical robots such as the hinotori surgical robot system (Medicaroid Corp.) and the da Vinci SP have now become available and be utilized in RANU. 10,11 There have been reports of the use of the Hugo RAS system (HRS) (Medtronic) in robot-assisted radical prostatectomy (RARP), partial nephrectomy, adrenalectomy, and radical cystectomy. However, there have been no detailed reports on RANU using the HRS. 12 –15
RANU is a somewhat complex procedure that involves simultaneous surgery on the upper and lower urinary tracts. The purpose of this study was to describe our initial experience with RANU using the HRS and evaluate its feasibility and safety.
Materials and Methods
Patient characteristics and management
We collected data from the first five consecutive patients who underwent RANU at Tottori University Hospital between September and November 2023 retrospectively. This study was approved by the Institutional Review Board of Tottori University Hospital (no. 22A117). All perioperative data, including the clinicopathological outcomes, were obtained from our hospital medical records. The indication for RANU in this series was clinically organ-confined high-risk UTUC. All patients underwent appropriate preoperative testing, including computed tomography of the pelvis to chest region, cystoscopy, and urinary cytology. Diagnostic ureteroscopy was also performed as needed. Perioperative complications were evaluated using the Clavien–Dindo grading system, and major complications were defined as those of Clavien–Dindo grades ≥3.
Study endpoints
This study aimed to demonstrate the feasibility and safety of RANU with the HRS. We also aimed to describe its use in this procedure, with an explanation of the surgical setup, including port and cart placement and docking angles. The patients’ characteristics and intraoperative and postoperative outcomes were evaluated. We used the chi-square and Mann–Whitney U tests to compare their outcomes with the 21 cases performed using our hospital’s da Vinci surgical system. All data were analyzed using the Windows R software (version 4.3.1), and p < 0.05 was statistically significant.
Patient positioning, port placement, and docking procedure
For the procedure, each patient was placed in a 70°–80° semilateral position, mild jackknife position with table flexion, with the upper extremity on the affected side placed dorsal to the midaxillary line. For the bladder direction stage, the patient was placed at 10°–15° and in the Trendelenburg tilt to prevent the bowel from interfering with the surgical field.
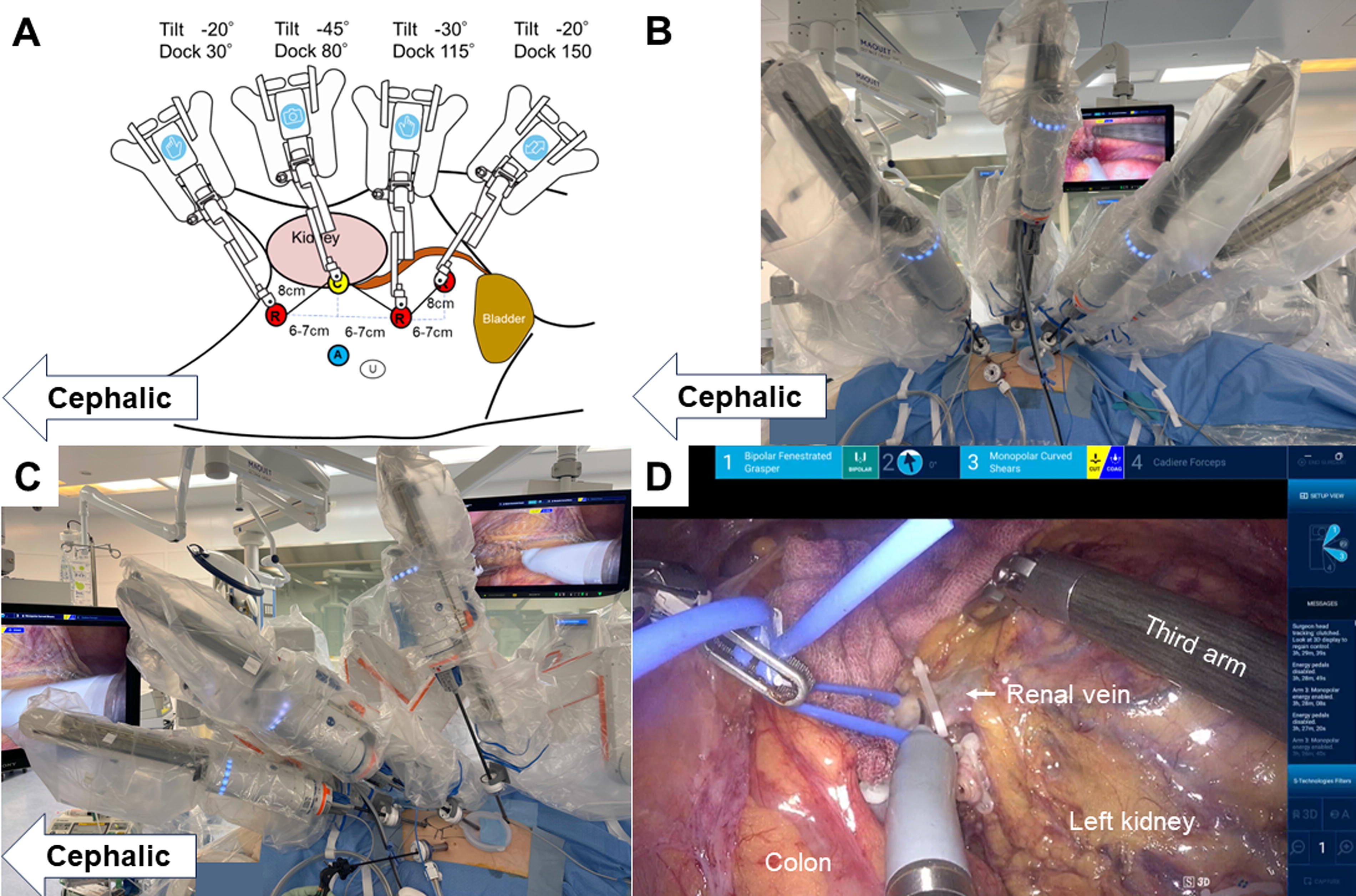
Because there have been no previous reports on RANU using the HRS, the port placement and docking were determined using a report on partial nephrectomy by Gallioli et al. 16 We validated port placement for this procedure using a dry box (Fig. 1A and B) and confirmed that the tips of the forceps could reach the required location and move within it. Figure 1C shows the robot arms’ port placement and docking angles in the first case. The 12-mm port for the surgical assistant was placed above the umbilicus, at approximately the same level as the camera port. Devices such as the Lap-Protector (Hakko Co., Ltd.) were initially used to allow the addition of assistant ports, if needed. They also facilitate the smooth removal of excised tissue. Although the first RANU case was completed safely, manipulation of the robotic forceps in the renal area was extremely difficult owing to the operational limitations of the arm (Fig. 1D). We kept the same port placement for the following cases but moved the third arm unit to the patient’s dorsal side. In addition, we adjusted the docking angles to accommodate the four arm carts. To minimize contact between adjacent arms, we adjusted arm tilts to create a height differential. Figure 2 shows the port placement and docking procedure for left-sided RANU and Figure 3 shows the procedure for right-sided RANU. The distance between the ports for each robotic arm was at least 8 cm, and the distance along the body’s long axis between each port was maintained at a minimum of 6–7 cm.

Preoperative simulation of robot-assisted radical nephroureterectomy using the Hugo RAS system using a dry box.
The port placement and docking angles of the robotic arms in left-sided robot-assisted radical nephroureterectomy using the Hugo RAS system at our institution after the first case.
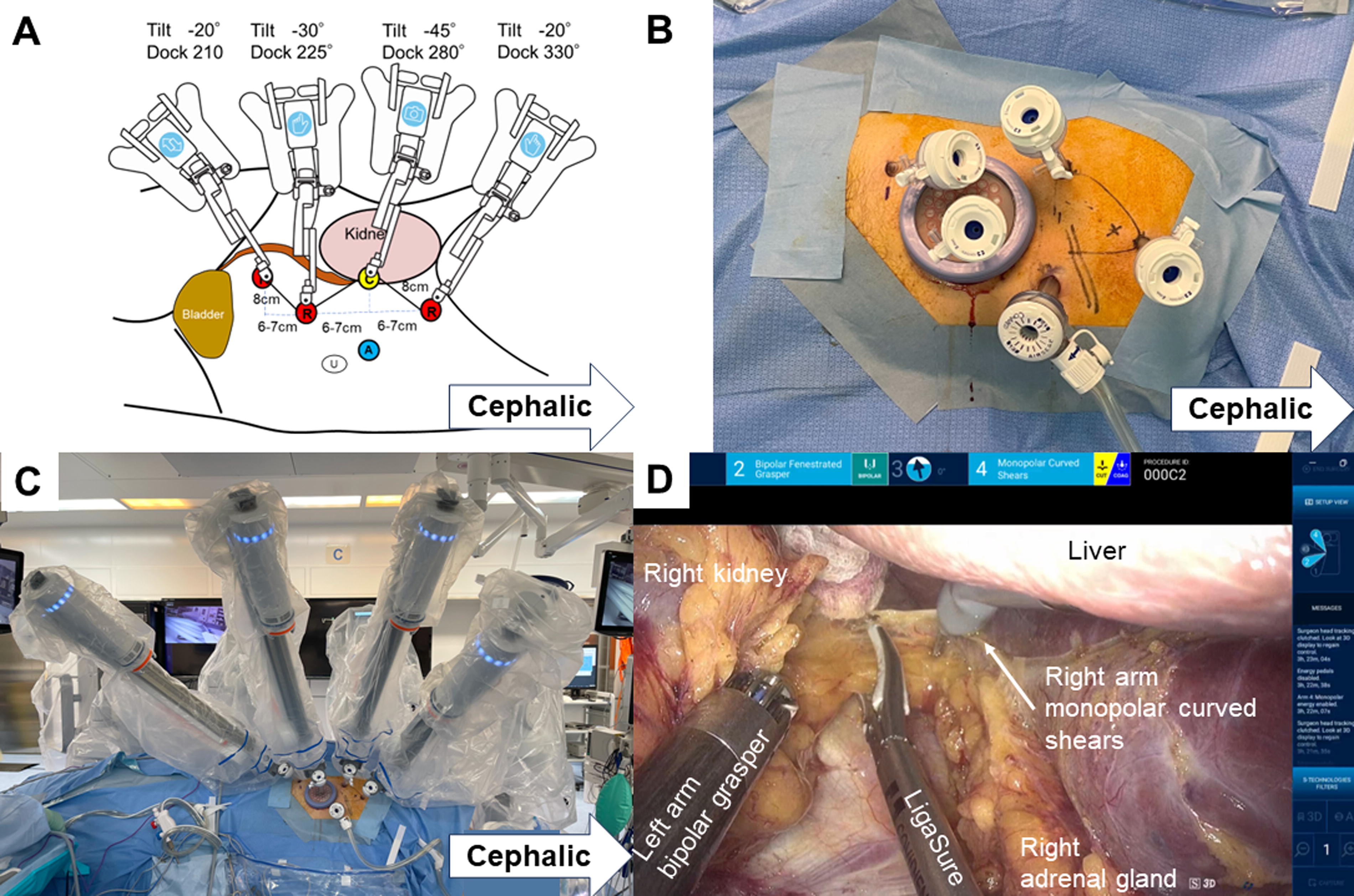
The port placement and docking angle of the robotic arms during right-sided robot-assisted radical nephroureterectomy using the Hugo RAS system at our institution after the first case.
Surgical technique
RANU was performed with the HRS operating a fenestrated bipolar grasper (with the left arm) and monopolar curved shears, or a large needle driver (with the right arm), and Cadiere forceps (with the third arm). All procedures were performed by a surgeon experienced in both LNU and RANU (S.M.) and all members of the surgical team received official training from Medtronic. All surgeries were performed using a transperitoneal approach, following the steps reported by Morizane et al. 9 for RANU using the da Vinci Xi system. We started with the nephrectomy portion (Fig. 2B). We dissected the colon at the White line of Toldt from the anterior renal surface. We approached the renal hilum along the gonadal vein. The renal artery and vein were dissected and divided separately using Hem-O-Lok clips. Then, the distal ureter was dissected toward the bladder (Fig. 2C). After injecting 100 mL of air through the urethral catheter, the bladder mucosa was cut at the ventral direction near the ureterovesical junction. The bladder cuff, including the ureteral orifice, was excised. A 3-0 absorbable barbed suture through the bladder wall including the mucosa was used to prevent slipping the bladder mucosa. After complete resection of the ureter, the removed kidney and ureter were placed in a retrieval bag. The bladder was then closed in two layers with running absorbable sutures. If a lymphadenectomy was necessary, it was performed after the RANU was complete. There were two major differences from RANU as previously reported using the da Vinci system 9 : (1) The robotic vessel sealing system could not be used; (2) Multiple targeting procedures were not required. The forceps and camera positions were not significantly changed.
Results
Table 1 shows the individual perioperative characteristics of the five patients treated with RANU using the HRS. The median age was 78 (68–82) years and the median body mass index was 25.0 (18.4–25.5) kg/m2. All surgeries were performed without rollout, redocking, or open conversion. The median operative time was 283 (203–377) min and the median time using the robotic system was 187 (121–277) min. The median estimated blood loss was 20 (5–155) mL, and none of the patients received blood transfusion. The median resected tumor weight was 275 (245–930) g, and the histology was urothelial carcinoma with negative surgical margins in all cases. Lymph node (LN) dissection of the aortocaval, paracaval, and common iliac area was performed in only one patient and 38 LNs were removed. The median duration of bladder catheterization was 8 (7–11) days, and the median length of hospital stay after surgery was 13 (9–17) days. No patient suffered any postoperative complications of Clavien–Dindo grade ≥3. Aside from the tumor location and frequency of lymph node dissection (LND), there were no significant differences in perioperative outcomes relative to the da Vinci Xi cases (Table 2).
Individual Preoperative, Intraoperative, and Postoperative Characteristics of Five Patients Treated with Robot-Assisted Nephroureterectomy Using the Hugo RAS System
Corresponding to Clavien-Dindo grade
CCI = Charlson comorbidity index; LOS = length of hospital stay; RAS = robot-assisted surgery; TNM = Tumor-node metastasis.
Comparison of Perioperative Outcomes of Robot-Assisted Nephroureterectomy with da Vinci and Hugo at Our Institution
Corresponding to Clavien-Dindo grade
Cis = carcinoma in situ; NA = not available.
In some locations on the upper pole of the kidney, handling of the forceps was a little more difficult than with the da Vinci system owing to arm movement limitations (Fig. 4A, Supplementary Video S1). However, by working in collaboration with the assistant’s LigaSure, these problems were easily resolved think (Fig. 4B). This LigaSure application, used effectively, was a particular advantage during right-sided RANU because it precluded the need for an additional assistant port to hold up the liver (Fig. 3D, Supplementary Video S2). The third arm, inserted through the most foot-side port, toward the bladder, provided good traction on the peritoneum and bladder, making it very easy to detach the ureter from the surrounding organs and suture the bladder (Fig. 4C and D). Supporting Supplementary Video S3 demonstrates bladder cuff excision for a left RANU and its suturing. The patients were not repositioned and the port placements remained unchanged. In the third case, the robot stopped working while dissecting the distal ureter toward the bladder. This wasted ∼49 minutes as the HRS had to be restarted.
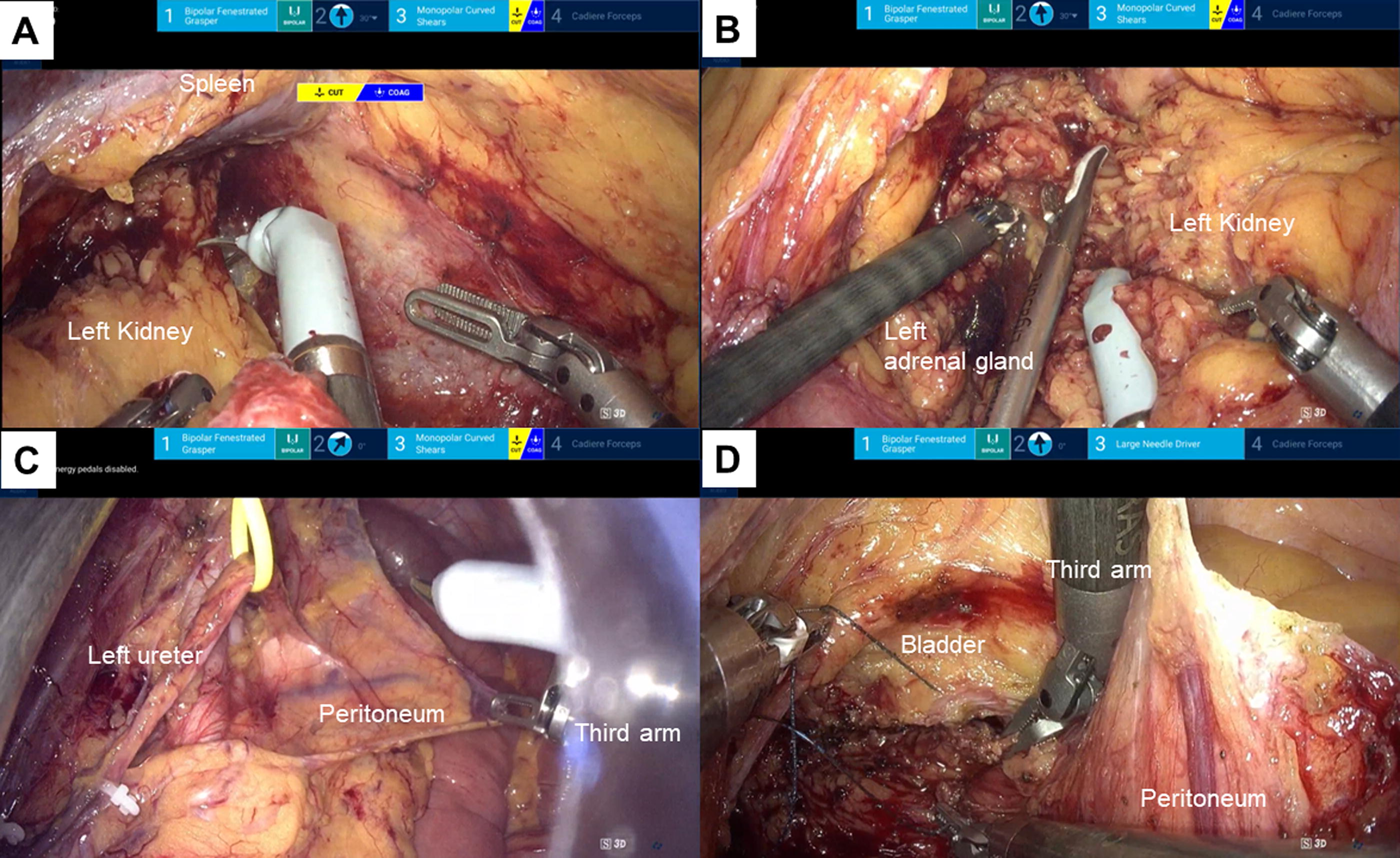
Images of robot-assisted radical nephroureterectomy using the Hugo RAS system.
Discussion
In this study, we demonstrated the feasibility and safety of RANU using the HRS. We described the optimal docking method for arm carts and details of the surgical procedure and challenges. The RANU using this system was performed without rollout, redocking, or repositioning. Although previous studies have reported the use of HRS, to the best of our knowledge, this is the first report on RANU using the HRS.
12
–15,17
The HRS differs somewhat from the hinotori and conventional da Vinci surgical systems. The most notable differences in the HRS are independent arm carts, open surgeon consoles, and rotation multiplier function
Comparison of da Vinci Surgical System and Hugo Robot-Assisted Surgery System
The independent and flexible arm carts make it easy to increase the number of arms to suit the surgical technique and patient physique or to select an unconventional port arrangement as needed. In RANU, it is important to identify the port placement that accommodates the widest range of surgical field. We have described two different arm cart docking methods, and docking the three or four arm carts from the dorsal side appears to provide the best range of motion for the forceps in RANU using the HRS. As tilt and dock are adjustable, some patient-specific modifications are acceptable. However, each tilt’s forceps range of motion is fixed (Fig. 5). In the first case, arm 3 was positioned from the abdominal side, restricting the forceps movement. Positioning arm 3 on the dorsal side for subsequent cases significantly improved the range of motion. Therefore, the target organ and range of motion should be considered before setting up the arm cart.
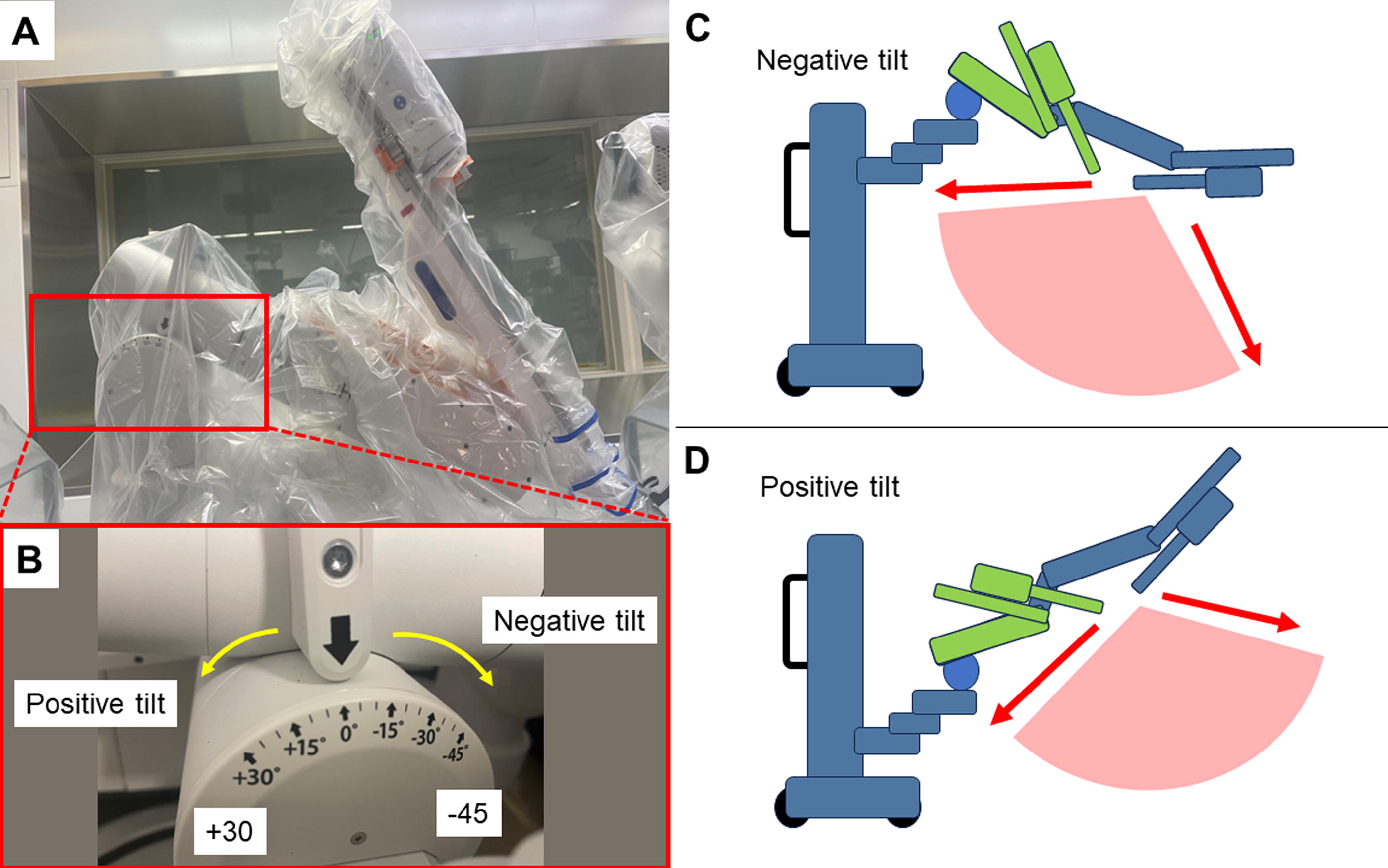
The Tilt Function of the Hugo RAS System.
The open surgeon’s console of the HRS is a feature not available in conventional surgical-assist robots. The console surgeon performs the robotic surgery wearing specially designed 3D glasses. A safety mechanism in the head-tracking system prevents unexpected accidents by stopping an arm’s movement when the surgeon is not looking at the monitor. Even those surgeons accustomed to immersive consoles can easily adapt to open console systems after only a few simulator training sessions. An open console is thought to facilitate communication between the surgical team in the operating room. 14,18 Unfortunately, we could not determine whether communication among staff was better with this system than with other surgical-assist robots because the HRS does not have microphones and speakers.
The rotation multiplier function of the hand of the robotic forceps is a novel and unique feature. The HRS enables computer-controlled adjustment of the degree of rotation of the hand joint portion of the robotic forceps, with three options: normal, 1.5×, or 2×. We believe this advantage is most apparent in vesicourethral anastomosis during RARP and bladder closure during RANU. We compared the two models by measuring the time from dissecting the lower ureter to completing the bladder repair with bladder cuff excision. We found no significant difference in time (p = 0.118). The rotational function of the HRS may be an advantage despite the somewhat challenging nature of bladder cuff excision and repair.
The HRS has only been on the market for one year in Japan, and we feel that the experience is still growing compared with the da Vinci surgical system. For example, there is a much smaller variety of robotic forceps, it lacks forceps with strong grasping power and does not have a robotic vessel sealing system. 18 However, forceps with a strong grasp are unnecessary for RANU, and Cadiere forceps are sufficient as a retractor arm. For the unimplemented vessel sealing system, a fenestrated bipolar grasper or monopolar curved shears may be sufficient. However, it is unfortunate that a foot pedal specific to LigaSure is unavailable now. As shown in Figure 3D, one port for the retractor arm can be reduced by dissection with the robotic left arm forceps and cutting of tissue with the assistant’s LigaSure. At the same time, the console surgeon elevates the liver with the robotic right arm forceps.
LND is an important part of RANU; owing to the very small sample size in this study LND was performed in only one case. However, the aortocaval, paracaval, and common iliac LNs were dissected, and 38 LNs were removed. Our findings suggest that RANU using the HRS, including LND, may be performed easily and safely comparable to those of the da Vinci system. In the third case in this study, a communication error occurred in the HRS, and operative time was wasted to restart the system. Although the error was recoverable in this case, the possibility of nonrecoverable errors has been reported even in conventional surgical systems, 19 and it is essential to remember that the robotic surgery may be impossible to continue when performing any kind of RAS. However, further improvements are required. The relatively long and thick instrument track and instrument drive unit can interfere a little with manipulating the robotic forceps. Nevertheless, the system’s four independent arm carts and well-crafted tilt function that can be freely set counterbalance these disadvantages.
This proof-of-concept and feasibility study demonstrated that HRS can safely perform RANU. Although the left-sided RANU allows for greater cephalic surgical manipulation, we used a symmetrical and identical setup for both sides. There was no significant difference in console time between the left and right sides (p = 0.80). However, our small study cohort limits our findings, and further studies are needed to optimize port placement and affirm the validity of our findings. One case in this study experienced a system error. Although this is a major limitation, restarting the robot solved the problem and the issue was communicated to the manufacturers. In addition, the high cost of robotic surgery remains an issue.
Conclusion
This is the first report describing RANU using the HRS, and the surgical setup described here may be a useful reference standard. Although RANU using this system can currently be performed without major problems, we expect that further improvements will soon be made to the arm cart, including the instrument track and instrument drive unit and the implementation of energy devices.
Footnotes
Acknowledgments
The authors thank the medical engineering, nursing, and anesthesia staff at the Tottori University Hospital.
Authors’ Contributions
S.M.: Wrote the main article text and prepared figures and performed the data analysis. H.Y., R.S., R.N., Y.K., and N.Y.: Performed perioperative management and data collection. A.H., K.H., M.H., and K.G.: Reviewed and edited. A.T.: Review and supervised.
Author Disclosure Statement
N.Y. has received a grant from Medtronic, but it is not directly related to this article.
Funding Information
No funding was received for conducting this study.
Supplementary Material
Supplementary Video S1
Supplementary Video S2
Supplementary Video S3
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.