
Abstract
Indications:
Transurethral ultrasound ablation (TULSA) is used for treating localized prostate cancer and benign prostatic hyperplasia (BPH). It’s particularly suitable for patients with low to intermediate risk, uni- and multifocal organ-confined prostate carcinomas, symptomatic obstructive BPH coinciding with prostate cancer, and postradiation therapy recurrences.
Technique:
The TULSA procedure involves meticulous preoperative preparation, precise surgical steps, and comprehensive postoperative care. Treatment is performed under magnetic resonance imaging (MRI) guidance using specialized MRI-compatible instruments, including a transurethrally inserted ultrasound applicator and an endorectal cooling device. Ablation is conducted through robot-driven rotation of the applicator, with real-time MRI thermometry used for monitoring and control.
Outcomes:
A retrospective single-center clinical evaluation involved 300 men with primary localized prostate cancer (PCa) confirmed by biopsy. The median age was 66 years, prostate-specific antigen levels were 6.85 ng/mL, cancer length was 7.6 mm, and prostate volume was 49.2 cc. The median follow-up period was 14 months. Treatments included whole-gland (163 men) and focal TULSA (137 men), with neurovascular bundle sparing in 248 men. Additionally, 88 patients received combined therapy for PCa and BPH.
Safety:
Grade 1 and 2 complications occurred in 57 patients, resolving within 4 weeks. Grade 3 adverse events were seen in seven patients, resolving within 3 months. No grade 4 or higher adverse events and no bowel-related complications were observed.
Functional Outcomes:
The median international index of erectile function score remained stable from 24 to 25 over 48 months. The international prostate symptom score initially worsened post-treatment but improved to better than baseline levels over 48 months. Pad-free continence was preserved in 96% of patients.
Oncological Outcomes:
Biochemical failure occurred in 26 men, with residual cancer confirmed by biopsy in 14 men. Salvage therapy was required for 14 patients, with 12 patients under active surveillance.
Indications
Transurethral ultrasound ablation (TULSA) is utilized for treating localized prostate cancer and benign prostatic hyperplasia (BPH). This procedure is particularly suitable for patients with low to intermediate risk uni- and multifocal organ-confined prostate cancer, symptomatic obstructive BPH coinciding with prostate cancer, postradiation therapy with localized recurrences, and for local palliative treatment of locally advanced and metastasized prostate cancer with local symptoms or severe lower urinary tract symptoms (LUTS).
Preoperative Preparation
The preparation for the TULSA procedure is meticulously planned to ensure optimal conditions and outcomes. The process takes approximately 45 to 60 minutes and includes the following steps: The patient is restricted to a liquid diet 1 day before treatment. On the day of the procedure, a laxative is administered 2 hours prior to the procedure.
The patient is then transported to the MRI room and positioned on the MRI table with legs secured in leg supports to facilitate better access for the Endorectal Cooling Device (ECD).
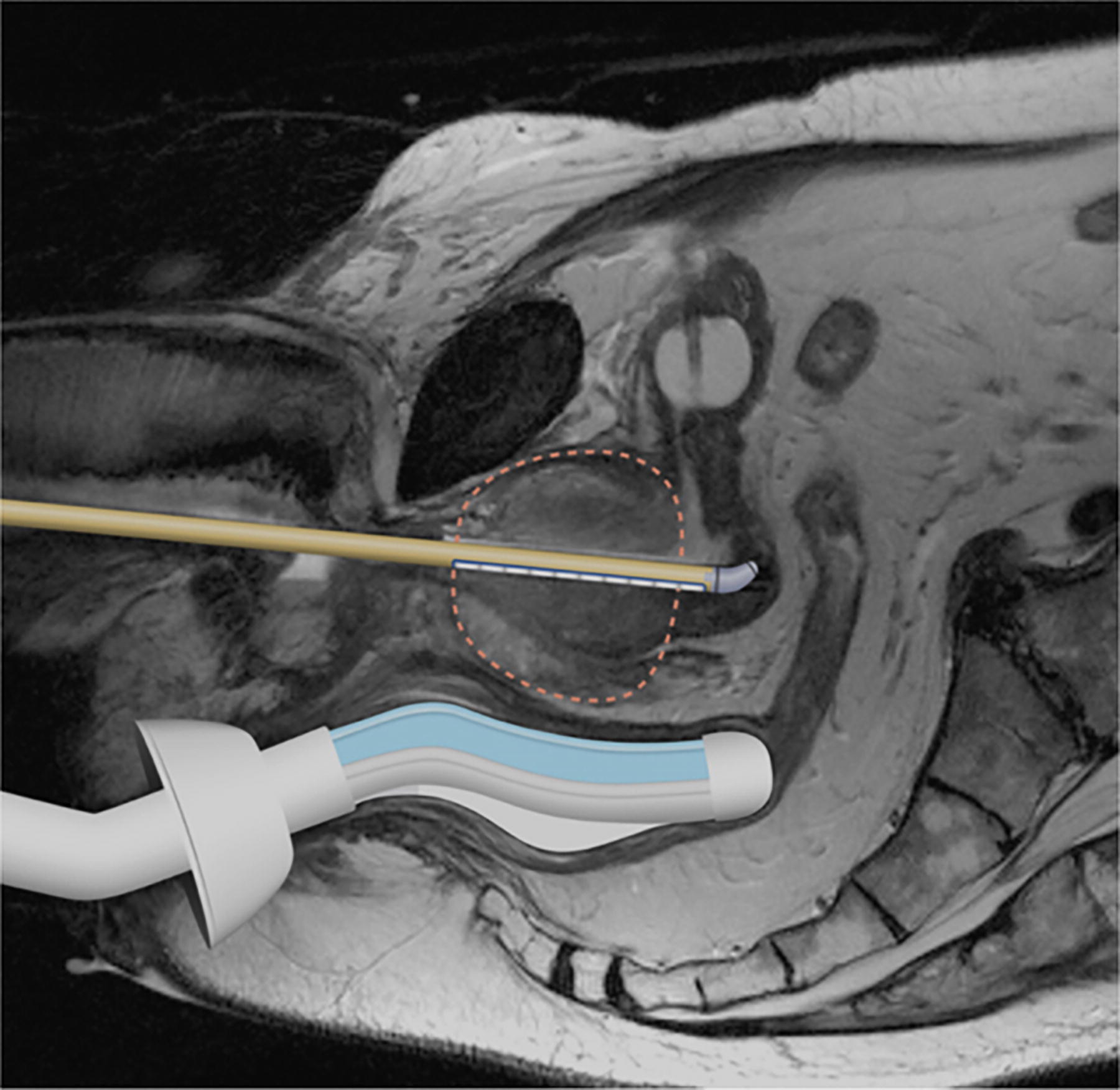
MRI image illustrating the placement of the TULSA applicator and the Endorectal Cooling Device (ECD). The TULSA applicator is precisely positioned within the prostate, indicated by the overlay illustration, ensuring targeted ultrasound ablation. The ECD, visible in the rectal area, helps maintain a stable temperature during the procedure. To enhance visualization, both the applicator and the cooling device have been added as graphical overlays on the MRI image. The MRI provides a clear view of the applicator’s alignment and the surrounding anatomical structures, confirming the correct positioning essential for effective treatment. TULSA, transurethral ultrasound ablation; MRI, magnetic resonance imaging.
Surgical Steps
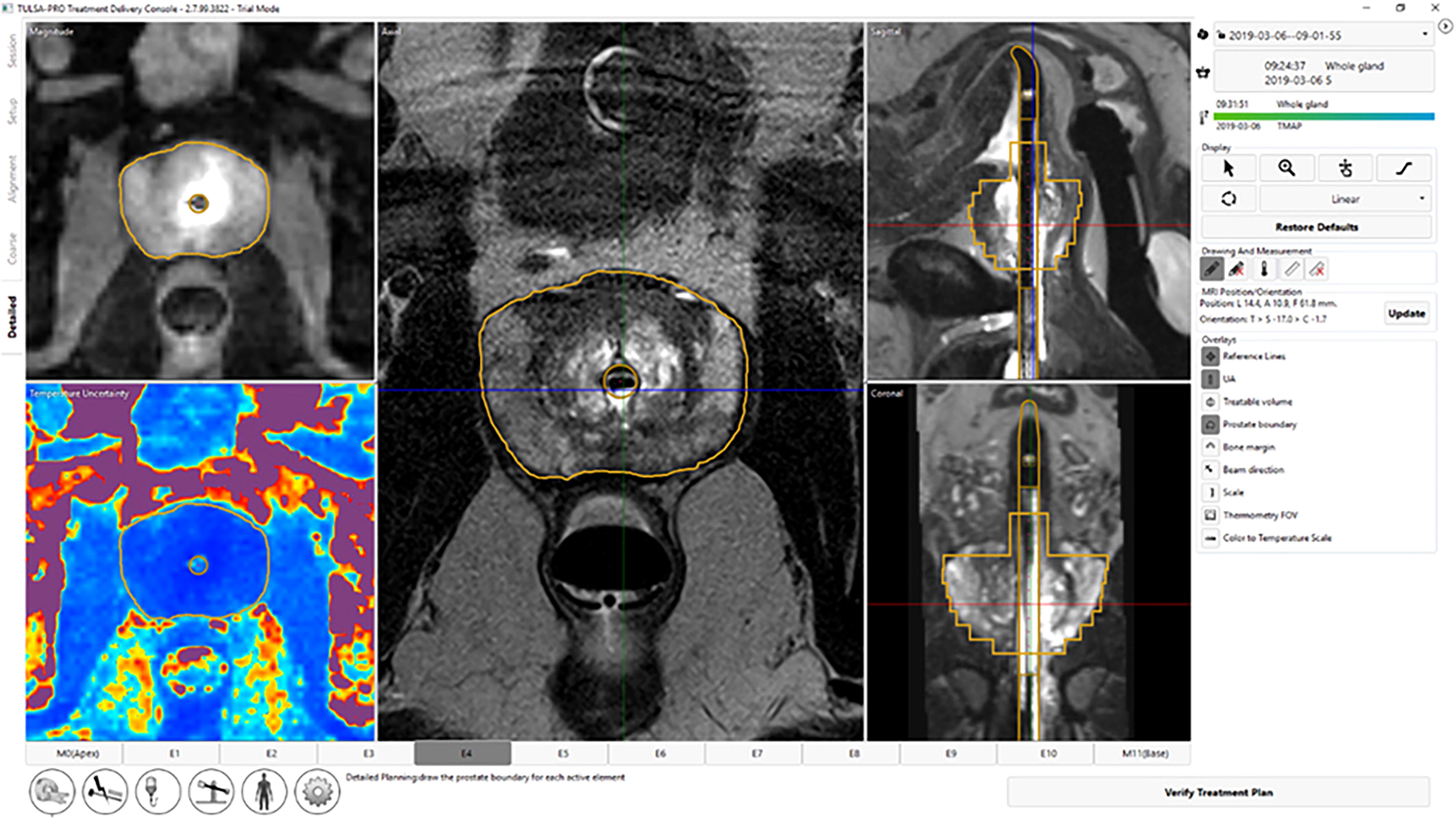
MRI image showing the delineated treatment area of the prostate. The targeted region for ablation is clearly marked, indicating the precise boundaries for the TULSA procedure. This delineation ensures that the ultrasound energy is accurately focused on the affected area, maximizing treatment efficacy while preserving surrounding healthy tissue. The overlay illustrates the extent of the ablation zone within the prostate, as confirmed by the MRI imaging. In the bottom left corner, the thermal map prior to the treatment is visible, showing the initial temperature distribution.

MRI images displaying the thermal distribution during the TULSA treatment and post-treatment MRI images of the treated area. The thermal map illustrates the cumulative heat spread within the targeted region of the prostate, ensuring effective ablation. Post-treatment MRI images confirm the ablated area, showing changes in tissue characteristics indicative of successful treatment. The thermal distribution overlay highlights the precision of the procedure, with controlled and focused energy delivery to the intended zones.
Postoperative Care
Patients typically stay in the hospital overnight following the TULSA treatment, although the procedure may also be conducted as a day case, depending on individual recovery and clinical guidelines. Continuous monitoring for potential postoperative complications is essential. Consultation for antibiotic and antithrombotic therapy is necessary to manage and prevent any adverse outcomes effectively.
Troubleshooting
Adjustments are made in cases of anatomical anomalies, such as the presence of calcifications that could block the ultrasound beam path. Previous surgical interventions are also considered during the planning of the ablation route.
Instrument List
Specific MRI-compatible instruments are used for conducting the TULSA procedure, including TULSA robots from the ALTA Clinic and various ultrasound devices and catheters. Detailed information on the manufacturers of these instruments will be included in the final manuscript.
10 independent ultrasound transducer elements; 4 & 13 MHz; 0 to 4 W acoustic/element Rigid catheter; Size 22 French; Sterile, single-use
Cooling; non-sterile, single-use
Robotically driven Linear control of UA (Coarse Planning) Rotational control of UA (Treatment)
Fluid circuit for UA and ECD System electronics to power and control all system components
Computer with proprietary software Treatment planning Real-time thermometry images Ablation feedback control algorithm
Clinical Results
Our retrospective single-center clinical service evaluation of MRI-guided TULSA for the treatment of organ-confined prostate cancer involved 300 men with primary localized PCa visible on MRI and confirmed by biopsy. The baseline characteristics included a median age of 66 years (IQR 60–73), PSA of 6.85 ng/mL (IQR 4.64–9.5), overall cancer length of 7.6 mm (IQR 4.35–10), and prostate volume of 49.2 cc (range 11–180). The median follow-up period was 14 months (IQR 4–30). Based on patients’ preferences and disease characteristics, 163 men received whole-gland treatments and 137 focal TULSA, with neurovascular bundle sparing attempted in 248 men. A subset of 88 patients with LUTS suggestive of BPH received combined therapy for both PCa and concurrent BPH in a single treatment.
Regarding safety outcomes, 57 patients experienced Grade 1 and 2 complications, mostly resolving within 4 weeks through prolonged catheterization and/or antibiotics. Grade 3 adverse events (urinary retention requiring surgical intervention) occurred in seven patients, resolving within 3 months. Notably, no grade 4 or higher adverse events and no bowel-related complications were observed.
Functional outcomes were promising. The median IIEF score of 24 [IQR 14–29] (n = 234) at baseline remained stable at 25 (IQR 13–30) (n = 28) by 48 months. The baseline IPSS of 8 (IQR 4–15) (n = 250) initially worsened post-treatment to 12 (IQR 5–19) but recovered to 8 (IQR 2.5–10.5) (n = 47) by 12 months and further improved to 6 (IQR 3–11) (n = 46) by 48 months. Importantly, pad-free continence was preserved in 96% (160/185) of patients based on surgeon assessment.
In terms of oncological outcomes, 26 men experienced biochemical failure (Phoenix ≥ 2) after a single TULSA treatment. MRI findings showed suspicion of residual cancer in 26 men, 14 of which were confirmed by positive biopsy. Subsequently, 14 patients received salvage therapy (3 surgery, 11 single repeat TULSA), 12 patients remained under active surveillance.
These results demonstrate that TULSA is a safe and effective therapy option for the treatment of organ-confined prostate cancer, offering minimal impact on patients’ quality of life while providing promising oncological outcomes. 1
Footnotes
Authors’ Contributions
L.E. and R.M.: Conceptualization; L.E. and R.M.: Methodology; L.E. and R.M.: Investigation; L.E.: Writing—original draft preparation; R.M.: Writing—review and editing; R.M.: Supervision. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
All other authors have no conflicts of interest.
Funding Information
This research received no external funding.