
Abstract
The following video atlas summary comprehensively reviews all technical aspects of the standardized set-up, patient positioning, electromagnetic-guided renal access, integrated irrigation-aspiration system use, and robotic lithotripsy of the novel MONARCHTM (Johnson & Johnson MedTech, Redwood City, CA) combined mini-percutaneous nephrolithotomy and flexible ureteroscopy platform.
Indications
Percutaneous nephrolithotomy (PCNL) is the procedure of choice for the management of complex (i.e., staghorn calculi or calyceal diverticular stones) and large renal stone burdens (i.e., lower pole linear stone burden ≥10 mm or nonlower pole linear stone burden ≥20 mm). 1,2 Albeit associated with higher stone clearance rates than flexible ureteroscopy (fURS), the risk of complications should not be overlooked. 3 –10 When encountered, hemorrhage necessitating blood transfusion has been identified as the most severe complication after PCNL (ranging from 1% to 17.5%). 11 Most bleeding events are associated with suboptimal renal puncture and tract dilation (i.e., infundibular or lateral to the calyceal fornix). 12,13 The potential for lesions of the surrounding viscera should also be considered. 11
Endoscopic combined intrarenal surgery (ECIRS), first described in 1995 for the management of patients with complex stone burdens and nondilated collecting systems by Grasso et al. and popularized by Khan, Clayman, and colleagues, seeks to maximize the advantages of both percutaneous and ureteroscopic approaches to stone burden while mitigating the associated morbidity seen with these procedures. 14 –16 Leveraging the ECIRS concept, this novel robotic platform allows for real-life ureteroscopic monitoring of renal puncture, tract dilation, and percutaneous sheath advancement. As an experimental device that is not Food and Drug Administration-approved and with only limited experience at the time of the writing of this article, the indications for MONARCH™ PCNL are yet to be defined. However, with the authors’ initial experience, and with a sense of realistic optimism, we believe that the platform will replace manual PCNL just as robotic-assisted laparoscopy replaced manual laparoscopy over the course of less than a decade.
Preoperative Evaluation
A thorough medical history and physical examination should be performed in all patients before percutaneous access. It is crucial to identify any conditions that may defer PCNL or favor alternative lithotripsy approaches, such as the presence of untreated urinary tract infections and uncorrected coagulopathies. Given the similarities in approach to ECIRS, patients should be counseled on the potential risks associated with both fURS and PCNL. Risks specific to fURS include ureteral wall injury, ureteral stricture formation, and ureteral avulsion. 17,18 Conversely, risks associated with PCNL include bleeding necessitating transfusion, radical nephrectomy or angioembolization, infection, and possible sepsis, development of arteriovenous fistula in cases of delayed bleeding, and injury to the surrounding viscera (resulting in pneumothorax, hydrothorax, or nephropleural fistula if the lung of the lung space is involved). 3,11 –13 If medically feasible, patients taking aspirin, or other antiplatelet, or anticoagulant medications should discontinue these medications before surgery to reduce the risk of bleeding complications during the procedure.
Preoperative laboratory evaluation for stone management procedures should encompass a complete blood cell count, serum electrolyte determinations, and renal functional tests. A crucial component of this evaluation is a preoperative urine culture to rule out an active urinary tract infection. 1,2 If the urine culture is positive, targeted perioperative antibiotic therapy should be administered to reduce the risk of infectious complications. The authors will not proceed with any PCNL procedure without a documented negative culture and have minimized severe infectious complications.
Although the evidence to support prophylactic antibiotic use in patients with sterile urine culture is scarce, it is widely accepted that prophylactic antibiotics can effectively mitigate infectious risks. 19 –22 This precaution is based on the understanding that although the urine is sterile, microorganisms may reside within the core of the stone. When the stone is fragmented during the procedure, these microorganisms can be released into the collecting system, potentially leading to infection. To this end, it has been noted that many patients with negative voided urine cultures before PCNL actually have positive kidney stone cultures. 23,24
Stone burden characterization is best achieved using helical noncontrast computed tomography. 25 –27 Understanding the renal vasculature and its relationship with the collecting system is essential for minimizing the risk of hemorrhagic events during percutaneous access gain. Important metrics to consider as part of preoperative planning include skin-to-stone distance, stone density, and the maximum linear dimensions of the stone in the three axial planes. Coronal views are also crucial for identifying the optimal calyx of percutaneous entry. As highlighted by Guglielmetti et al., determining the optimal angle of entry is critical, with recommended angles of ≥117° for rigid nephroscopy and ≥68° for flexible nephroscopy, respectively. 28 Additionally, CT scans can occasionally reveal the presence of a retrorenal colon, which, although rare, increases the risk of colon perforations during percutaneous access procedures.
Patient Positioning
To date, all PCNL procedures have been conducted under general anesthesia. The patient is positioned securely in a modified supine lithotomy position, with the respective flank elevated using a bolster to optimize access to the targeted kidney. Next, an axillary roll is deployed under the patient, caudal to the axilla. It is important that the axillary roll does not occupy the axilla to avoid the potential development of brachial plexus palsy. The ipsilateral arm is draped across the torso and separated from the dependent arm by multiple pillows (Fig. 1). All pressure points are carefully padded to minimize the risk of pressure injuries. The posterior axillary line, 12th rib, and iliac crest are marked, and the patient’s flank and genital area are prepped and draped in the standard sterile manner.

Patient positioning. All patients were placed in a modified supine position, with the lower body placed in a lithotomy position, the ipsilateral flank raised using a bolster to optimize access to the targeted kidney, and the ipsilateral arm draped across the body and separated from the dependent arm by multiple pillows.
Gaining Retrograde Access
Manual flexible cystoscopy is then performed to assess the urethra and bladder for any tumors, stones, or foreign bodies. Upon identification of the ipsilateral ureteral orifice, a retrograde ureteropyelogram was conducted. A 12 French (Fr) Foley catheter was deployed to maintain bladder decompression, and a 35 or 45 cm 14 Fr ureteral access sheath (UAS) was deployed ∼4 cm below the ureteropelvic junction. This specific distance allows for optimal deflection of the robotic ureteroscope tip. After placing the UAS, the two lower robotic arms, utilized for driving the ureteroscope, laser, and basket, were docked between the patient’s legs (Fig. 2). A single-use robotic ureteroscope was then locked in place onto the robotic arm and guided through the UAS into the collecting system using the robotic hand-held console.
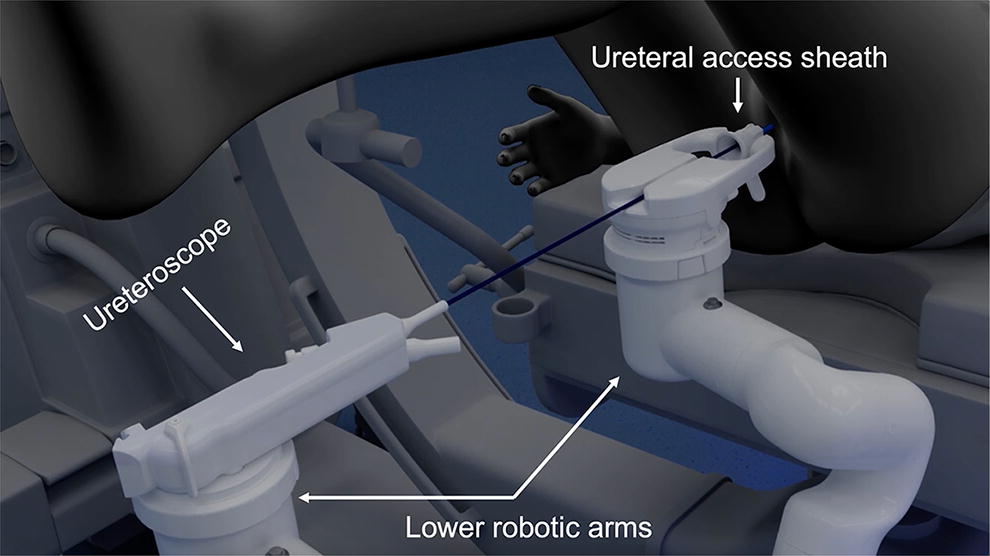
Lower robotic arms docking. A single-use robotic ureteroscope was locked in place onto the two caudal arms and guided through the deployed ureteral access sheath into the collecting system via the hand-held robotic console.
Optimal of Choice Selection
Following the endoscopic examination of the collecting system and selection of the optimal calyx by the surgeon, fluoroscopy is briefly utilized to refine the percutaneous needle deployment site. The surgeon selects a percutaneous site posterior to the posterior axillary line for needle insertion. Next, the third robotic arm is positioned at the patient’s side, aligned with the level of the anterior superior iliac spine. The compact field generator (CFG) is attached to the robotic arm and an electromagnetic field is activated (Fig. 3). The surgeon initiates the targeting process by gently touching the tip of the ureteroscope of the chosen papilla and marking the site for percutaneous access with the system (Fig. 4A). The ureteroscope is then retracted ∼5 mm from the targeted papilla to optimize visualization of the intended percutaneous access site, and this site is noted with the system (Fig. 4B). This provides the robotic platform with an understanding of the target location relative to the needle and ureteroscope.
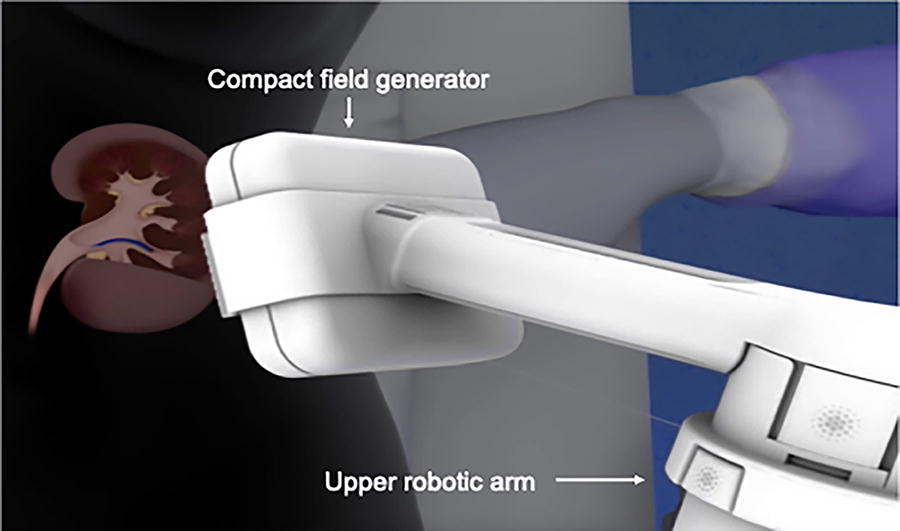
Upper robotic arm docking. To enable electromagnetic-guided percutaneous renal access, a compact field generator was locked in place on the upper robotic arm at the level of the anterior superior iliac spine.
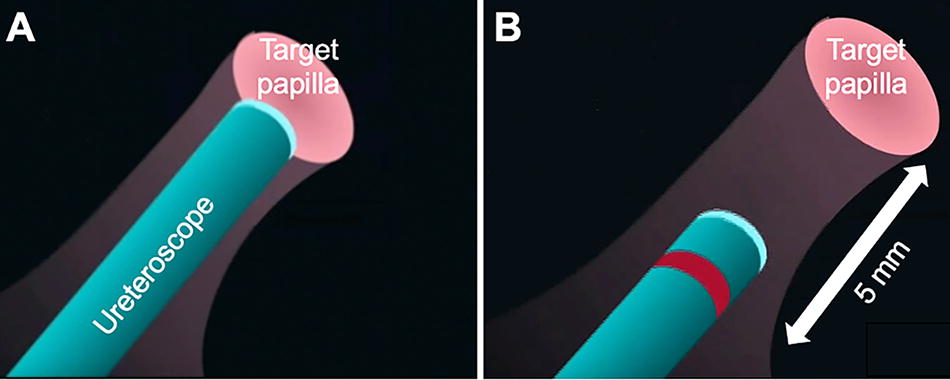
Target papilla selection.
The electromagnetic-guided percutaneous renal access utilizes electromagnetic markers on both the tip of the ureteroscope and the puncture needle to facilitate precise targeting. An intuitive graphical user interface (GUI) provides the surgeon with crucial targeting information, in terms of both the relative direction of the needle to the target (represented by the position of the virtual electronic bubble) as well as the relative distance to the desired calyx of choice (represented by the outer circumferential line on the GUI). When aiming to gain percutaneous access, the surgeon’s objective is to ensure that the position of the virtual electronic bubble, representing the needle tip, remains consistently centered on the target as the needle is manually advanced.
With progressive advancement through the skin, the outer circumferential line on the GUI moves from its initial 12 o’clock position around the circle until it completes an almost full rotation back to the 10 o’clock marking at which point the needle penetrates the collecting system (Fig. 5). This visual feedback assists the surgeon in accurately approximating the distance toward the target calyx. Ultimately, the goal is to visualize the puncture needle penetrating within 2 mm of the center of the papilla, ensuring a safe and precise access to the calyx of choice. Mapping of the renal vasculature highlighted that to mitigate the risk of vascular injury, one should aim for the central region of the renal papilla as the risk of hemorrhage is heightened by percutaneous punctures through the infundibulum, a region that is highly vascularized. 12,13

Graphic user interface for the electromagnetic-targeted percutaneous renal access.
Irrigation-Aspiration System
After deploying the needle, the CFG, two guidewires, a safety, and a working guidewire are then introduced into the collecting system. Using the standard Seldinger technique, tract dilation is performed, and an 18 Fr percutaneous metal sheath is inserted into the collecting system and securely locked onto the bed. This access site is immobile throughout the procedure minimizing parenchymal trauma and risk of loss of access.
Once the 18 Fr sheath is deployed and stabilized, a steerable robotic 15 Fr irrigation-aspiration catheter is introduced through the metallic 18 Fr percutaneous sheath. Irrigation goes into the collecting system around the suction catheter. The robotic console provides precise control not only of the ureteroscope but also over the irrigation inflow and suction outflow, allowing adjustment of these parameters according to the surgeon’s needs.
Laser Stone Lithotripsy with Active Fragment Suctioning
The MONARCH™ robotic platform is laser agnostic. For the 13 cases performed so far utilizing this novel robotic system, we have utilized the Moses™ 2.0 120 W Holmium Laser System (Boston Scientific, Marlborough, MA), but any laser can be used with the system. During the procedure, smaller stone fragments are rapidly aspirated through the suction catheter. Larger fragments, on the other hand, land on the tip of the aspiration catheter, where they are held in place by suction, facilitating laser lithotripsy. In addition to fragment aspiration, the suction catheter can be utilized to relocate stones within the collecting system, enhancing stone ablation and fragment removal during the procedure.
Postoperative Follow-Up
All procedures were “tubeless,” completed without the need for a nephrostomy tube but an indwelling ureteral stent was left in place for 7 days postoperatively. A postoperative chest X-ray was only performed if percutaneous access was gained above the 12th rib.
Although a thorough ureteroscopic examination of the collecting system to identify any residual stone fragments (RSF) is warranted at the end of the procedure, stone-free status post-PCNL should be assessed based on a thin slice (2–3 mm thickness) noncontrast CT scan performed within 3–4 weeks after the procedure. The use of plain abdominal X-ray and ultrasonography is, unfortunately, lacking the proper sensitivity to detect “clinically insignificant” RSF (i.e., 4 mm or less). 25 –27 However, recent studies have emphasized that RSFs are far from being clinically insignificant, as even smaller fragments can act as a nidus for stone growth and eventually, reintervention. 29,30 In fact, it seems that upon stratification by maximum linear measurements, among patients with RSF <2 mm in size, 16% require reintervention and 47% experience stone growth within the first postoperative year. 29
Footnotes
Authors’ Contributions
J.L. and M.D. conceptualized the study. J.L., M.D., and A.D.C. worked on methodology. J.L., M.D., and A.D.C. performed investigation. J.L., M.D., and A.D.C. wrote, reviewed, and edited the manuscript. J.L. and M.D. performed supervision of the study.
Author Disclosure Statement
The following are paid consultants of the company who have sponsored this study: Jaime Landman, MD, and Mihir Desai, MD.
Funding Information
This study was funded by Auris Health, Johnson and Johnson.
Supplementary Material
Supplementary Data S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.