
Abstract
Introduction and Objective:
Given the favorable cancer-specific survival rates in localized prostate cancer and the negative impact of whole-gland treatments on functional outcomes, the field is moving toward precision strategies such as focal therapy and organ-sparing surgery. We aim to report medium-term functional and oncologic outcomes for the initial Single-Port Robotic Transvesical Partial Prostatectomy (SP-TVRAPP) patient cohort.
Materials and Methods:
We analyzed a prospectively maintained database of 20 patients who underwent SP-TVRAPP between February 2021 and March 2024. Inclusion criteria were prostate-specific antigen (PSA) ≤10 ng/mL, clinical stage ≤ cT2b, ISUP Grade Group ≤3, unilateral lesions on multiparametric magnetic resonance imaging (mpMRI) with positive biopsy cores on the same side, and preoperative IIEF-5 ≥ 17. We also considered bilateral prostate cancer in the anterior zone and invisible mpMRI tumors confirmed by unilateral positive biopsies.
Results:
At baseline, patients had an average age of 61 years, a median PSA of 4.8 ng/mL (interquartile range [IQR]: 3.7–7.7), and a median Sexual Health Inventory for Men (SHIM) score of 24 (IQR: 18–25). All procedures were completed without complications, need for additional ports, or conversion. After a median hospital stay of 4.2 hours, 94% of cases were discharged without opioid prescriptions, and Foley catheters were removed after approximately 4 days. At 6 weeks, 3, 6, and 12 months postprocedure, potency rates, defined as a SHIM score ≥17, were 45.0%, 77.7%, 83.3%, and 87.5%, respectively. When potency was defined as having erections sufficient for penetration, the rates were 80.0%, 88.8%, 88.8%, and 93.7% for the same time intervals. Regarding urinary function, 60.0% were continent at 1 week, increasing to 85.0% by 6 weeks, 88.8% at both 3 and 6 months, and reaching 93.7% at 12 months postsurgery. Oncologically, 30.0% experienced upgrading and 40.0% upstaging within this cohort. Negative surgical margins were attained in 85.0% of the cases and the median PSA was 0.4 ng/mL 12 months after SP-TVRAPP. Two men were found to have residual GG1 cancer in the protocol biopsies and are currently on active surveillance. At a mean follow-up of 15.5 months (0.2–34.8) months, none of the patients has required secondary interventions, and all remain free of both clinically significant residual prostate cancer and metastatic disease.
Conclusions:
SP-TVRAPP represents a promising treatment for certain patients with localized prostate cancer. This targeted surgical method has been associated with faster postoperative recovery and has demonstrated high rates of early recovery in erectile function and urinary continence while ensuring oncologic safety.
Introduction
Long-term studies have consistently demonstrated favorable survival outcomes in localized prostate cancer, whether patients opt for whole-gland treatments or active surveillance (AS). 1,2 This observation, coupled with the high incidence of erectile dysfunction (ED) (50%–70%) and urinary incontinence (5%–20%) after radical surgery and radiation, underscores the pressing concern of overtreatment. 3 On the contrary, the risk of metastatic progression, particularly for those with intermediate-risk disease, increases under an AS approach. 1,4 Recent data suggest that about 60% of patients initially choosing conservative management will transition to radical interventions within 10 years. 1 Recognizing these complex dynamics, focal therapy (FT) has emerged as a middle-ground option, bridging the gap between AS and whole-gland treatments. Nevertheless, questions persist about its oncologic safety, with reported local recurrence rates as high as 42% at a median follow-up of 24 months. 5
Given the critical role of the index lesion (IL) in prostate cancer progression and the limitations of FT, innovative surgical methods such as precision prostatectomy and partial prostatectomy have emerged, pioneered by Menon et al., Kaouk et al., and Villiers et al. 6 –10 These techniques focus on removing clinically significant cancer while preserving the neurovascular bundle and seminal vesicle opposite the IL. For lesions exclusively anterior, some approaches strive to safeguard both the bilateral seminal vesicles and neurovascular bundles. 8,10,11 Although the degree of prostate tissue preservation varies between techniques, the overarching goal remains the same: to balance effective cancer treatment with maximal conservation of functional outcomes.
In 2018, Kaouk et al. introduced the Single-Port Robotic Transvesical Partial Prostatectomy (SP-TVRAPP) technique, demonstrating its feasibility with the da Vinci SP (Intuitive Surgical, Inc., Sunnyvale, CA). 12 The SP-TVRAPP approach resulted in minimal patient morbidity and improved focalization of the surgical field compared to previously reported transperitoneal approaches. In this analysis, our objective is to present the medium-term oncologic and functional outcomes observed in the initial patient cohort treated with SP-TVRAPP.
Materials and Methods
Study population
We performed a retrospective analysis using a prospectively maintained database of patients who underwent SP-TVRAPP between February 2021 and March 2024. The criteria for procedure eligibility included a prostate-specific antigen (PSA) ≤10 ng/mL, clinical stage ≤ cT2b, ISUP Grade Group ≤3, detection of unilateral lesions in multiparametric magnetic resonance imaging (mpMRI) with corresponding positive biopsy cores on the same side, and a preoperative Sexual Health Inventory for Men (SHIM) score of ≥17. We also considered cases with bilateral cancer localized in the anterior zone and mpMRI-invisible tumors confirmed by unilateral positive biopsies. Patients were excluded if they presented with a large cribriform pattern, had received androgen deprivation therapy within the past 6 months, or had undergone primary treatments such as radiation therapy or FT. Before providing the consent, patients were thoroughly informed about the innovative aspects of the procedure, including its indications, which are similar to those used for FT, as well as the risks, benefits, and possible complications.
Surgical technique
Our technique has been previously described. 9,11,12 In summary, patients are placed in a lithotomy position, and the Koelis Trinity (Koelis Inc., Princeton, NJ, USA) is used to merge preoperative mpMRI and real-time intraoperative ultrasound images, facilitating the identification of the IL. A suprapubic incision is made two fingerbreadths above the pubic symphysis, and after exposing the bladder, a vertical cystotomy is performed to insert the wound retractor. The da Vinci SP access kit is attached, and insufflation is set at 10–12 mm Hg.
In cases where the tumor is located in the peripheral zone (PZ), both the anterior and posterior bladder neck on the same side as the IL are transected. Posteriorly, the dissection continues through the retrotrigonal layer until exposing the ipsilateral vas deferens and seminal vesicle. Anteriorly, the endopelvic fascia is incised, and the ipsilateral puboprostatic ligament is transected. If necessary, the dorsal vein complex can be ligated. A tailored anterograde nerve-sparing approach is executed on the side of the lesion, with the vascular pedicle being controlled using clips and/or bipolar limited cautery. The apical dissection is then carried out, preserving the maximal length of the membranous urethra. Subsequently, the prostate is incised along the midline, tracing the course of the urethra (Fig. 1). For tumors located in the anterior zone, the procedure spares the posterior PZ and the seminal vesicles, whereas an en-bloc excision is performed on the transitional zone (TZ), anterior fibromuscular stroma, and apical anterior horns.
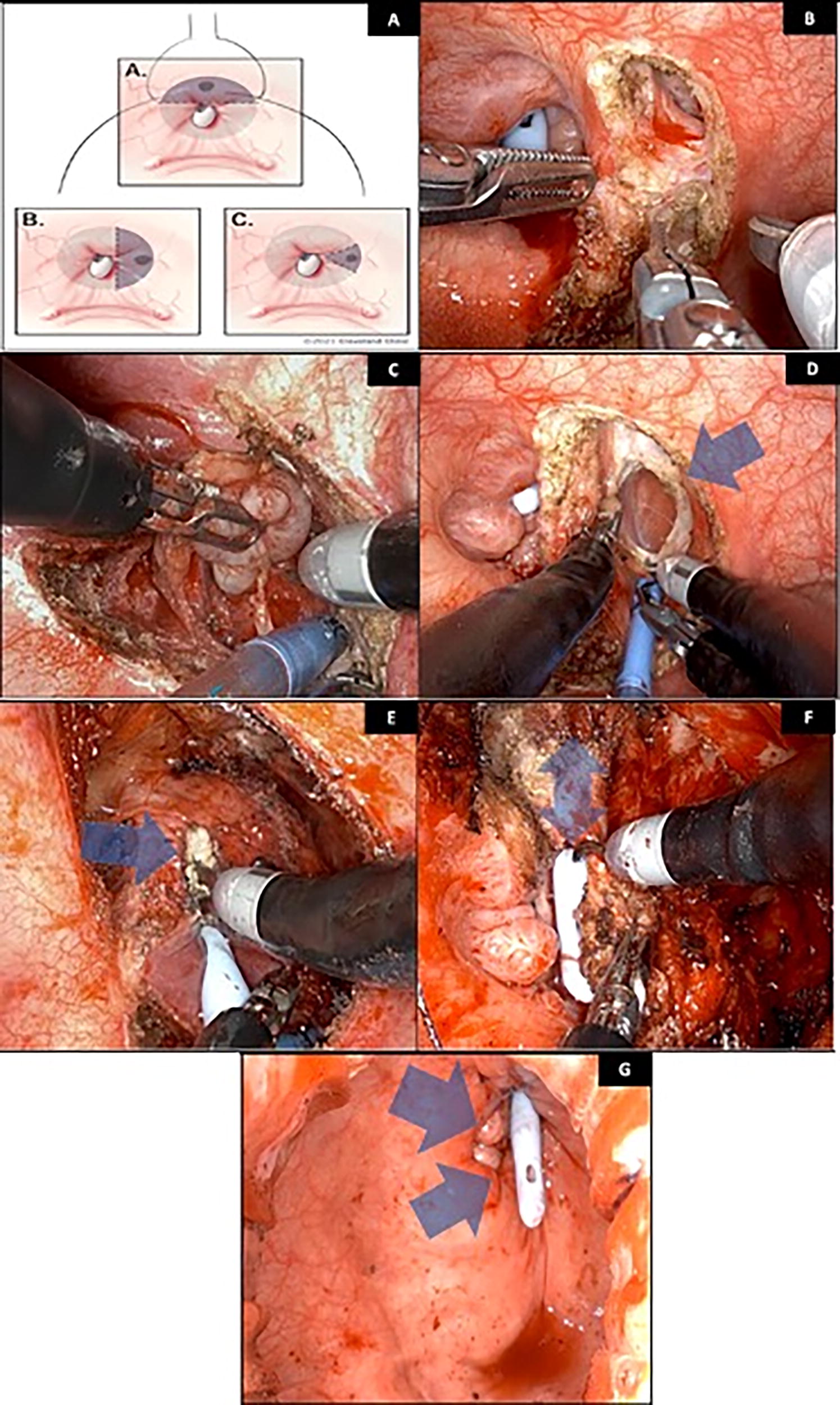
Intraoperative images of a right-side Robot-Assisted Partial Prostatectomy are presented.
Finally, the specimen is removed, and the Koelis system is employed to assess the remaining prostate. Tissue samples from the apex, mid, and base, both medially and laterally within the excised field, are then sent for intraoperative frozen section analysis to confirm the absence of the tumor. Thus, for anterior prostatectomies, a total of 12 samples are sent, whereas in cases of right or left PP, 6 samples are dispatched. Under decreased pneumovesicum pressure, ranging from 5 to 8 mm Hg, the vesicourethral anastomosis is performed using a monofilament barbed suture. A 20F Foley catheter is then inserted, the robot is undocked, and a layered closure is completed. 13
Importantly, in the most recent four instances of SP-TVRAPP, a 3D-printed model derived from preoperative mpMRI (Lazarus 3D, Albany, OR 97321) was utilized immediately prior to the surgery. This model served educational purposes and allowed for rehearsal of the procedure, aiding in tailoring the nerve-sparing approach on the side of the IL and in planning the resection margins (Fig. 2).

Preoperative 3D-printed model for rehearsal of a right-side Robot-Assisted Partial Prostatectomy.
Definition of outcomes
The follow-up appointments were conducted at 6 weeks, 3, 6, and 12 months postsurgery, and semiannually thereafter. A mandatory mpMRI was performed at 6 months, and a remnant biopsy at 12 months, or earlier if clinically indicated (Fig. 2).
Data concerning urinary continence (UC) and erectile function (EF) were independently verified by two authors. UC was defined as requiring either zero or one safety pad daily. Adequate EF was indicated by a SHIM score ≥17 or erections enough for penetration. Biochemical recurrence (BCR) was assessed using the Phoenix criterion for radiation therapy, defined as an increase of 2 ng/mL or more above the nadir PSA, 14 and the Huber criterion for FT defined as a PSA nadir of 1.0 ng/mL at 12 months and 1.5 ng/mL at 24–36 months after treatment. 15
The presence of the IL was identified using the highest Prostate Imaging–Reporting and Data System score or, in cases with multiple lesions of identical scores, by the lesion with the greatest volume. A positive surgical margin (PSM) was noted when cancer cells were found in contact with the inked edge of the prostatectomy specimen. PSM was categorized as “Limited” for lengths <3 mm, and “nonlimited” for lengths ≥3 mm.
Statistical analysis
Continuous variables were presented as either the median with the interquartile range (IQR) or as the mean along with its corresponding range. Categorical variables were expressed in terms of frequency and percentages. The Kaplan–Meier analysis was utilized to evaluate the probability of remaining free from biochemical failure. All statistical evaluations were conducted using STATA 18 software (StataCorp LP, College Station, TX, USA).
Results
At baseline, patients had an average age of 61 years, a median PSA of 4.8 ng/mL (IQR: 3.7–7.7), and a median SHIM score of 24 (IQR: 18–25). Most individuals had intermediate-risk prostate cancer at diagnosis. All procedures were completed without intraoperative complications, use of additional ports, or conversion. After a median hospital stay of 4.2 hours (IQR: 3.7–4.9), 94% of cases were discharged without opioid prescriptions, and Foley catheters were removed after approximately 4 days (range 3–6). No readmissions were observed after the surgery. Nonetheless, two patients experienced hypercontinence and needed urethral catheterization for 24 and 72 hours, respectively (Table 1). Unfortunately, one patient died 2 months postsurgery from an acute myocardial infarction, as confirmed by autopsy, with no findings related to the surgery. Postoperative oncologic and functional outcomes were analyzed accordingly.
Perioperative Characteristics of the Patients Who Underwent SP-TVRAP
BMI = body mass index; EBL = estimated blood loss; IQR = interquartile range; ISUP GG = International Society of Urological Pathology Grade Group; mpMRI = multiparametric magnetic resonance imaging; PDE5i = phosphodiesterase type-5 inhibitor; PSA = prostate-specific antigen; PI-RADS = Prostate Imaging–Reporting and Data System; SHIM = Sexual Health Inventory for Men.
Potency, defined as a SHIM score ≥17, was achieved by 45.0% (9/20) of patients at 6 weeks, 77.7% (14/18) at 3 months, 83.3% (15/18) at 6 months, and 87.5% (14/16) at 12 months. When a definition of erections enough for penetration was employed, 80.0% (16/20), 88.8% (16/18), 88.8% (16/18), and 93.7% (15/16) were potent at 6 weeks, 3, 6, and 12 months, respectively. Remarkably, 35.0% (7/20) did not require phosphodiesterase type 5 inhibitors after the procedure. Regarding urinary function, 60.0% (12/20) of patients were continent at 1 week, and 85.0 (17/20) achieved continence at 6 weeks. This rate improved to 88.8% (16/18) at 3 months and remained stable at 6 months postsurgery, eventually reaching 93.7% (15/16) at 12 months (Fig. 3).
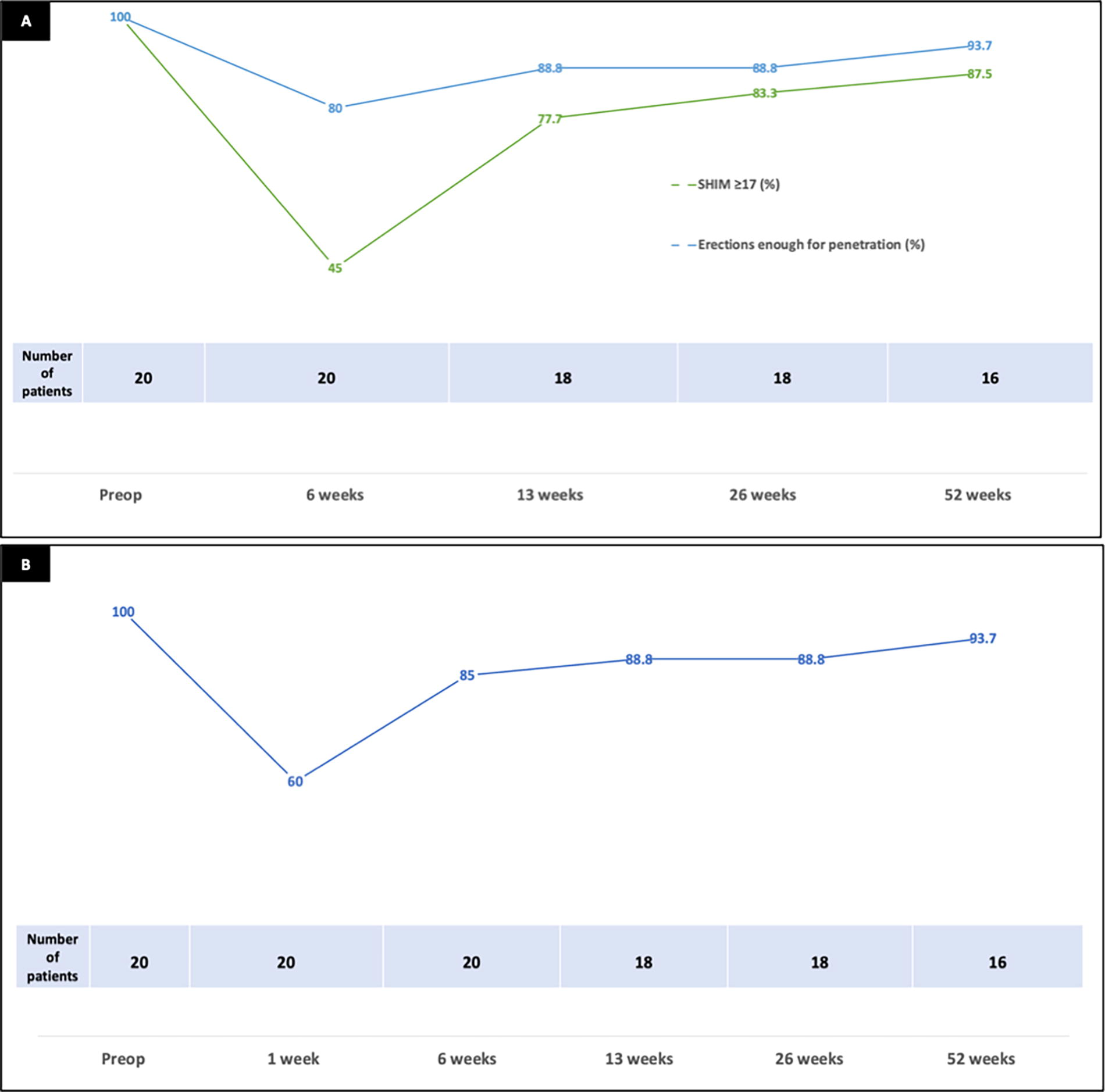
Functional outcomes after SP-TV RAPP.
From an oncological perspective, 30.0% (6/20) of patients in this cohort experienced upgrading, and 40.0% (8/20) upstaging. Negative surgical margins were achieved in 85.0% (17/20) of the cases, and the median PSA was 0.4 ng/mL (IQR: 0.2–1.2) 12 months after SP-TVRAPP. Although parameters for BCR have not been established in this context, the application of the Phoenix and Huber Criteria would yield an estimated 24-month freedom from BCR of 83.6% (95% CI 46.5%–95.9%) and 73.2% (95% CI 42.0%–89.4%), respectively. However, it is important to note that among patients meeting BCR criteria, only one was found to have GG1 prostate cancer upon subsequent biopsy. In the remaining cases, elevated PSA interfaces were attributed to the presence of benign tissue.
Overall, two patients were found to have ISUP GG1 cancer in the protocol biopsies and are currently under AS. In the first case, a single positive core with 15% involvement was identified on the side of the partial prostatectomy. In the second case, a total of three positive cores were detected, with two on the contralateral side and one on the partial prostatectomy side, exhibiting core involvement ranging from 10% to 30%. At a mean follow-up of 15.5 months (0.2–34.8), none of the patients have required secondary interventions, and all remain free of clinically significant residual prostate cancer and metastatic disease (Table 2).
Oncologic and Functional Outcomes of Patients Who Underwent SP-TVRAPP
One patient died 2 months after the surgery because of an acute myocardial infarction. This death was determined not to be related to the surgical procedure. Postoperative oncologic and functional outcomes were analyzed accordingly.
Both corresponded to ISUP GG 1.
BCR = biochemical recurrence; IQR = interquartile range; ISUP GG = International Society of Urological Pathology Grade Group; PSA = prostate-specific antigen; SP-TVRAPP = Single-Port Robotic Transvesical Partial Prostatectomy.
Discussion
The management of localized prostate cancer is increasingly focusing on improving patient quality of life. This shift is supported by the encouraging long-term cancer-specific survival rates observed after both whole-gland treatments and AS, with only about 3% of patients dying from prostate cancer. 1 In this context, the risk of overtreatment represents a significant issue, particularly considering the prevalent incidence of ED. 16 –18 Furthermore, although many patients are initially eligible for AS, a high percentage will eventually require radical interventions within 5–10 years, emphasizing the complexity involved in prostate cancer treatment.
FT has arisen as an option between AS and whole-gland treatments, mainly suited for patients with intermediate-risk prostate cancer. By targeting the tumor-affected area, FT seeks to preserve organ function without compromising cancer control. Early outcomes appear promising, indicating potency rates of approximately 90% and UC rates from 92% to 100%, over median follow-up periods ranging between 13 and 32 months. 19 –21 Nonetheless, high local recurrence rates remain a concern, largely because of the inherently multifocal nature of prostate cancer. 5,22 Compounding this challenge is several factors that limit FT’s applicability, including prostate size, the presence of calcifications, tumor location, proximity to the external urethral sphincter, and the size of the IL. Moreover, FT is mostly restricted to treating visible lesions on mpMRI, which may overlook as much as 35% of clinically significant prostate cancers. 23 –25 In response to those limitations, organ-sparing surgeries, also known as precision and partial prostatectomies, have been developed. These approaches were initially described for the management of anterior prostatic tumors and have since been progressively adapted to treat posterior tumors. 26 The primary goal is to preserve critical anatomical structures, such as the neurovascular bundles and seminal vesicles, on the side opposite to the IL, thereby minimizing functional impairment. Unlike FT, these surgical techniques allow for the retrieval of the specimen and the use of intraoperative frozen sections, ensuring the complete excision of the tumor and addressing the potential underestimation of the IL volume by mpMRI. 27
Our functional outcomes from partial prostatectomy align with those reported by Sood et al. on precision prostatectomy. 7 The authors observed that by the fourth month, 63% of patients had achieved a SHIM score ≥17, increasing to 79% by the eighth month. In a similar trend, our study demonstrated potency rates of 77% and 83% at 3 and 6 months, respectively. Furthermore, 89% of our cases were continent at 3 months, which is comparable to the 94% reported by Sood et al. at 4 months. As anticipated, partial prostatectomy, which preserves a greater amount of prostatic tissue, resulted in higher median PSA interfaces at one year and, consequently, higher rates of BCR according to the Phoenix and Huber criteria. However, our study has not yet detected any cases of clinically significant prostate cancer in follow-up biopsies, nor have our patients required salvage treatments. It is also noteworthy that in most instances where the PSA was detectable, benign tissue was identified in the remnant prostate.
Interestingly, in our study, all the patients with PSM had a Gleason pattern 3 at the margin, indicating less aggressive behavior. Moreover, two of the three patients with PSM had undergone anterior partial prostatectomy. Although the presence of a PSM in partial prostatectomy cases may be concerning, research indicates favorable oncological outcomes and higher BCR-free survival rates for tumors in the TZ. A comprehensive study of over 7000 patients undergoing Robot-Assisted Radical Prostatectomy (RARP) revealed an increased risk of PSM in TZ tumors, particularly at the anterior bladder neck and apex. However, these tumors were also less likely to show extracapsular extension, lymph node involvement, or adverse histological features. 28 Consistent with these findings, none of the patients with TZ tumors in our cohort have shown evidence of non-organ confined disease in the final pathology or signs of local recurrence to date. Similarly, Villiers et al. recently published the long-term follow-up of patients who underwent Transperitoneal Robot-Assisted Anterior Partial Prostatectomy, demonstrating acceptable oncological outcomes. The authors reported a 62.7% (35.0%–81.3%) freedom from cancer recurrence at seven years, alongside no evidence of metastatic disease or the need for systemic treatment. 10
From an operational standpoint, the primary advantages of FT include its suitability for outpatient procedures, low morbidity, short-term catheterization, favorable pain profile, and the feasibility of repeat ablative procedures in cases of residual or recurrent disease. Nonetheless, the introduction of the SP system and the advancements in TV approaches for robot-assisted prostatic surgery have extended those benefits to more complex interventions. This is exemplified in our cohort, where the average hospital stay after SP-TVRAPP was only 4.2 hours. Furthermore, 94% of our patients were discharged without the need for opioids, and the usual time of catheterization was 4 days. A key factor driving the results is the concept of surgical regionalization. The use of pneumovesicum, which avoids the peritoneal cavity, offers several gains. It reduces the risk of intraoperative complications, accelerates the recovery of postoperative bowel function, and allows patients to maintain a flat position, thereby decreasing procedure-related morbidity. 29,30 Consequently, SP-TVRAPP has emerged as a viable alternative to FT, presenting fewer contraindications and comparable functional benefits. Moreover, the incorporation of an intraoperative MRI-US fusion system has significantly enhanced the precision of our surgical approach. This system is utilized not only for tailoring surgery but also for confirming the complete elimination or treatment of the visible lesion.
The integration of 3D printing models into surgical planning, already proven effective in RARP, 31,32 is poised to improve SP TV-RAPP outcomes. Expected advantages include lower PSM rates, reduced operative times, and enhanced nerve-sparing techniques on the side of the IL. Our initial experience with two cases using this methodology is encouraging, though a larger sample of patients is needed to confirm these observations. In parallel, innovations such as prostate-specific membrane antigen positron emission tomography, microultrasound, and tissue-based biomarker profiling are anticipated to transform surgical planning, enabling more precise patient risk stratification and the development of customized treatment plans. 33,34
Our study is not devoid of limitations, including a small sample size and a retrospective design. Additionally, since all procedures were performed by an experienced surgeon in robot-assisted SP-TV techniques, our findings may not be generalizable to other clinical practices. Despite these limitations, we observed favorable perioperative results. Although the full spectrum of long-term oncologic outcomes is yet to be established for FT and partial prostatectomy, there is a growing consensus that not all prostate cancer patients require extensive radical interventions to achieve oncological safety. This recognition continues to drive efforts to minimize the side effects associated with treatments.
Conclusion
SP-TVRAPP represents a promising treatment for certain patients with localized prostate cancer. This targeted surgical method has been associated with faster postoperative recovery and has demonstrated high rates of early recovery in EF and UC while ensuring oncologic safety. However, to validate these preliminary results and evaluate long-term patient outcomes, additional research is necessary.
Footnotes
Authors’ Contributions
A.M.P.: Conceptualization (supporting), formal analysis (lead), writing—original draft (lead), and writing—review and editing (lead). E.L.F.: Data curation (lead) and writing—review and editing (equal). R.R-.C.: Data curation (supporting). N.S.: Data curation (supporting) and review (equal). J.S.C.: Review and editing (equal). C.M.: Review and editing (equal). J.K.N.: Review and editing (equal). J.K.: Conceptualization (lead), review, and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.