
Abstract
Introduction:
Several complications of retrograde intrarenal surgery have been attributed to inadvertent increases in intrarenal pressure. We recently described the development of an innovative isoprenaline-eluting guidewire (IsoWire). The objective of this study was to investigate the impact of this IsoWire on the intrarenal pressure and evaluate its safety.
Materials and Methods:
This study was performed in 17 renal units using a porcine model. As controls, the intrarenal pressure, heart rate, and mean arterial pressure were measured for a duration of six minutes with a standard guidewire placed in the renal pelvis. For the experiment, the conventional guidewire was substituted with the IsoWire and the same parameters were measured. Blood samples were taken at one-minute intervals to measure plasma isoprenaline levels. This procedure was repeated on the opposite side.
Results:
The mean intrarenal pressure reduction was 29% (95% CI: 13%–53%). The mean isoprenaline effect time was 174 seconds. No changes in heart rate (p = .908) or mean arterial pressure (p = .749) were recorded after IsoWire insertion. Plasma isoprenaline levels were below the quantitation threshold. Isoprenaline concentrations in the plasma were below the quantification threshold. Ureteroscopy revealed no ureteral lesions.
Conclusions:
The IsoWire demonstrated a safe and effective reduction of intrarenal pressure. Additional research is necessary to determine whether ureteral smooth muscle relaxation generated by isoprenaline facilitates easier insertion of a ureteral access sheath, decreases the incidence of ureteral access sheath related ureteral lesions, or even encourage the practice of sheathless retrograde intrarenal surgery.
Introduction
The prevalence of urolithiasis has steadily increased in the recent decades. The lifetime risk is 7 and 13% in women and men, respectively, with a recurrence rate of 50% within 10 years. 1
Increased prevalence leads to increased costs for both the patient and health care system. The use of flexible ureterorenoscopic devices and lasers for retrograde intrarenal surgery (RIRS) has gained traction, so much so that prominent urological societies, including the European Association of Urology (EAU) and the American Urology Association (AUA), continue to expand its use in their guidelines. 2,3
However, RIRS is associated with several complications. Normal physiological intrarenal pressure (IRP) in an unobstructed human kidney ranges from 0 to 15 mmHg (0–20 cmH2O) 4 and this IRP is comparable to pressures in pigs. 5 During RIRS, intraluminal renal pelvic pressure ranges from 35 (±10) mmHg during simple diagnostic ureterorenoscopy to 54 (±18) mmHg during stone management. Maximum pelvic pressure peaks of 288 and 328 mmHg were recorded during forced irrigation with a 20-mL syringe and holmium laser use, respectively. 6 Dangerous increases in IRP beyond the safety threshold result in pyelorenal reflux and forniceal rupture. The former predisposes the patient to fever, urosepsis, and postoperative pain and was initially thought to occur when pressures exceed 30–45 mmHg. 7 However, recent work by Lildal et al. showed that intrarenal reflux may occur at IRPs as low as 16 mmHg (range 16–25 mmHg, mean 21 mmHg) in normal, nonhydronephrotic kidneys. 8
We recently presented the design and first in vitro release tests of an isoprenaline-eluting guidewire (“IsoWire”). 9 This IsoWire, depicted in Figure 1, has a nitinol core and a fine stainless-steel wire twisted tightly around it. The spiral grooves created by the coil served as a reservoir for the loading of hydrogel and isoprenaline. This hydrogel-coated isoprenaline-loaded guidewire was sheathed into a 5 French (F) open-ended ureteral catheter. Hydrogel was strategically applied to seal the junction between the open-ended catheter and guidewire to prevent the unintended release of isoprenaline, allow easy cannulation of the ureteral orifice, and allow smooth guidance into the pelvicalyceal system. After fluoroscopy confirms the accurate position, the protective sheath is removed and the drug diffuses from the coating when it becomes hydrated. Isoprenaline is a beta-agonist, which stimulates beta-adrenergic receptors in the renal pelvis and ureters causing relaxation of the smooth muscle. 7
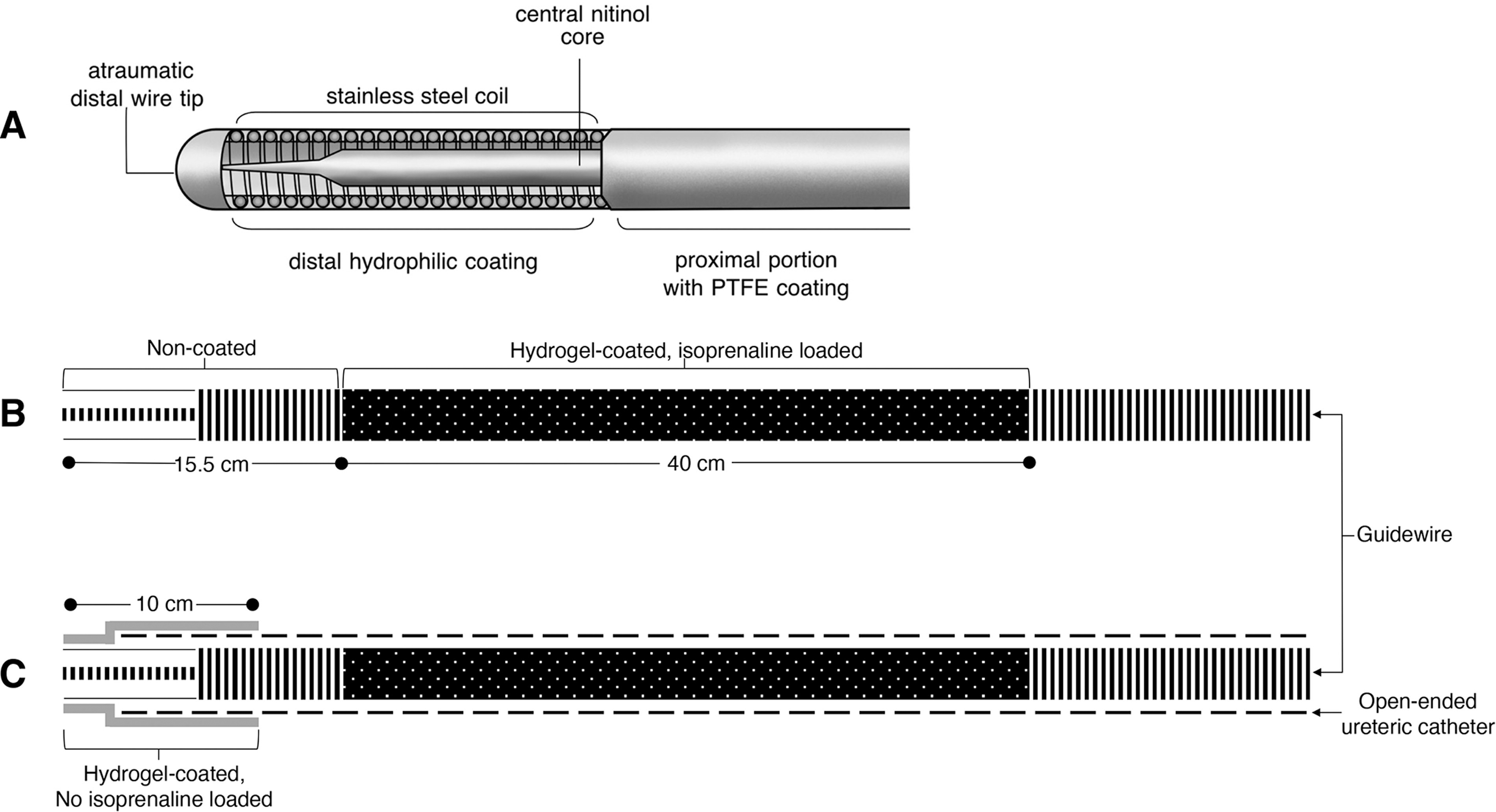
Schematic illustration of the structure of IsoWire
Our preliminary in vitro pilot demonstrated that the IsoWire, which releases 7.5 ug isoprenaline during the first minute, is safe, with no changes in mean arterial pressure (MAP), heart rate (HR), or any abnormal electrocardiography (ECG) changes. Furthermore, analysis of the isoprenaline release profile from the hydrogel-coated guidewire showed that most (63.9 ± 5.9%) of the loaded drug mass was released in the first minute, and almost all the drug was released exponentially in the first 4 minutes. All plasma isoprenaline levels were below the quantitation limit. 9 The aim of this study was to investigate the effect the IsoWire, which releases 7.5 ug isoprenaline during the first minute, has on IRP, how long this effect lasted for, and to determine its safety in a porcine model.
Material and Methods
Ethics statement
This study adhered to the institutional protocol for animal experimentation and was approved by the Animal Ethics Committee of the Faculty of Health Sciences of the University of Cape Town (020_011).
Study design
Animal model
Nine female pigs (white, Landrace breed, weight 50–60 kg) were transferred to the study site and kept for a period of seven days to adapt to the new surroundings (Fig. 2). The subjects were provided with a conventional pig diet for up to 12 hours before the investigation, but their access to water was unrestricted. Before transfer to the operating room, the pigs were premedicated with diazepam using a transdermal patch. They were administered medetomidine (0.06 mg/kg IM), Zoletil (3 mg/kg IM), and butorphanol (0.15 mg/kg IM) to induce anesthesia. Subsequently, they were intubated and ventilated using the GE Healthcare S5 Avance system. Anesthesia was maintained with isoflurane 1.5–3% in oxygen. To maintain proper hydration, an initial rapid infusion of saline was administered at a rate of 90 mL/kg/hour for 5 minutes. Hydration was then sustained during the procedure by administering saline solution (9 g/L sodium chloride) at a rate of 10 mL/kg/hour continuously through an ear vein. Under ultrasound guidance, a central venous catheter and a femoral arterial catheter were placed to facilitate blood sampling and monitoring of invasive blood pressure and HR. Baseline HR and MAP were measured, and any anomalies on the three-electrode ECG were documented. Blood was drawn for baseline isoprenaline levels.
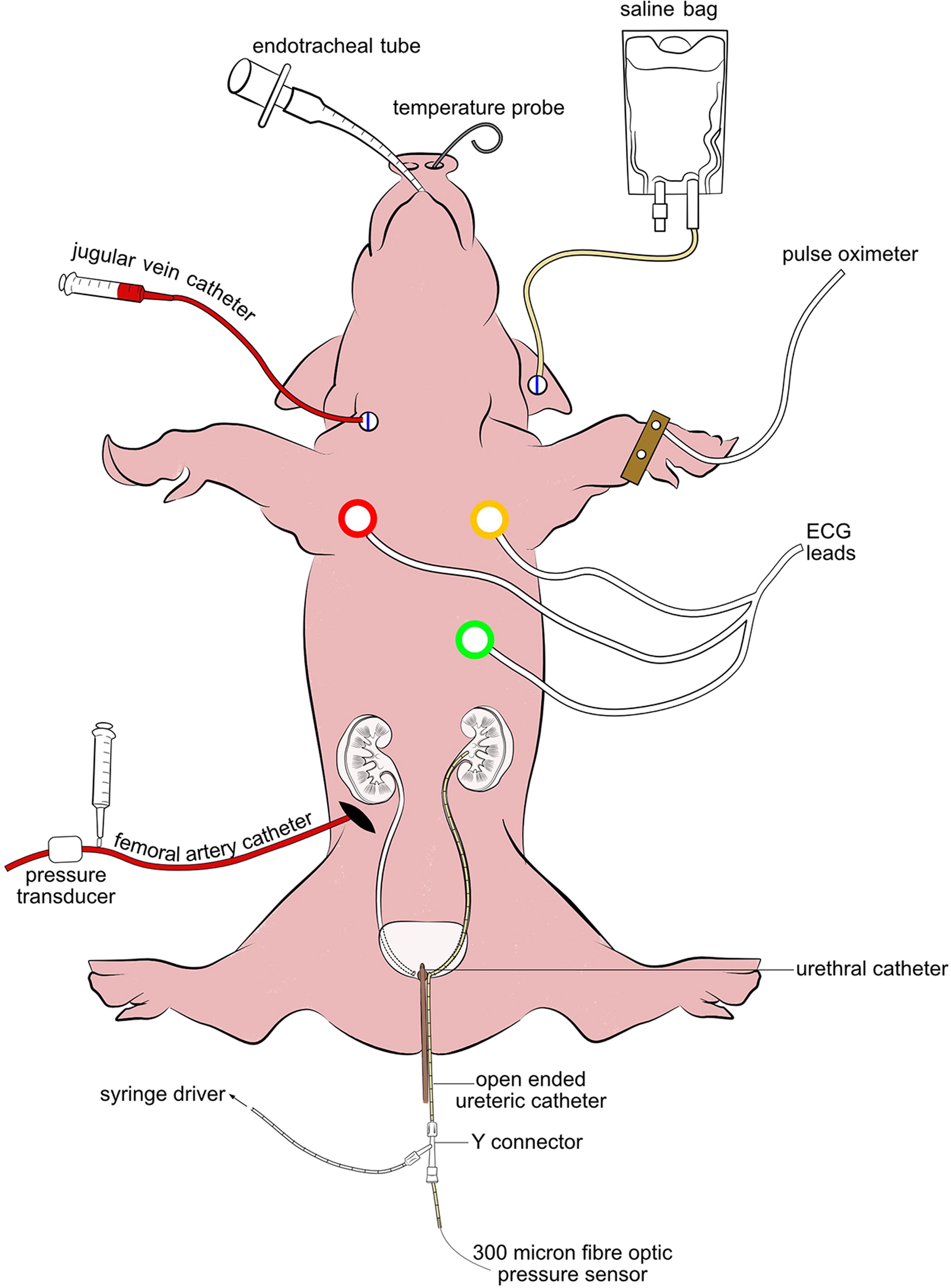
Visual demonstration of the animal model. 9 ECG-Electrocardiogram.
Endourological procedure
Both ureteral orifices were first cannulated using hydrophilic guidewires (0.035 inches). A 6F ureteral catheter was inserted over one guidewire. Retrograde pyelography was performed to identify any congenital abnormalities. Thereafter, a Y-connector was attached to the end of the ureteral catheter to allow passage of a 300 µm fiberoptic pressure measurement device (FISO Technologies, Inc., Quebec, Canada) into the renal pelvis through one port. Saline irrigation was initiated through the second port at a rate of 10 mL/min. The bladder was kept empty using a 10F urethral catheter. In the control group, a standard guidewire was inserted into the renal pelvis on one side, and the IRP, HR, and MAP were measured continuously for six minutes. The conventional guidewire was replaced with an IsoWire for the experiments. Once the IRPs had stabilized during the exchange of guidewires and fluoroscopy confirmed that the correct position of the IsoWire was in the renal pelvis, the protective covering of the IsoWire was removed to allow for discharge of isoprenaline and exposure of the drug to the urothelium. The IRP, HR, and MAP were measured continuously for six minutes. Blood samples were obtained every minute, for six minutes to measure plasma isoprenaline levels. Once collected, they were centrifuged at 1000×g for 15 minutes and stored at −80°C (−112°F) until analysis. To stabilize isoprenaline in the serum, 30 µL of an aqueous solution containing 6.5M citric acid and 0.568M ascorbic acid was added to 6700 µL of plasma. On the day of the analysis, freshly prepared working solutions in water containing 0.1% acetic acid and 1 g/L ascorbic acid were spiked into the plasma. Following a validated method 10 set by the Federal Drug Association (FDA) and European Medicines Agency (EMA), 10 µL of extracted plasma was injected for analysis using liquid chromatography–tandem mass spectrometry. This method yielded a minimum quantifiable limit of 0.488 ng/mL.
Ten minutes after the experiment and control were completed on one side, the same procedure was repeated on the contralateral side. This ten-minute interval was determined after considering the short half-life of isoprenaline 11 and findings from our release profile investigations showed that almost all the drug was released exponentially in the first 4 minutes. 9 To conclude the experiment, bilateral ureteroscopy was performed to detect any ureteral injuries.
Statistical analyses
All analyses were performed using Statistical Package for the Social Sciences Version 28, and the significance level was set at p < 0.05. Data are reported as the mean, median, and standard deviation (SD). Dependent sample t-tests compared the mean pressure between the standard guidewire and IsoWire for the entire sample and each kidney. Pearson’s correlation analyses were used to assess the relationship between isoprenaline effect time and pressure reduction for the whole sample and for each kidney. Dependent sample t-tests were used to compare the MAP and HR before and after IsoWire insertion.
Results
Eighteen renal units were included in this study. Neither the standard guidewire nor the IsoWire could be advanced into the renal pelvis in one renal unit. These investigations were conducted in 17 renal units. The IRP decreased across all renal units, overall and in both the left and right kidneys (p < 0.001; see Table 1). The mean IRP reduction was 29% (95% CI: 13%–53%) (SD = 13%), ranging from 13% to 55%. The mean isoprenaline effect time was 174 seconds (SD = 60.6) (Table 2). There was no significant correlation between the isoprenaline effect time and pressure reduction in the whole sample (r = −194; p = 456), left (r = −0.381; p = .312), or right (r = −0.078; p = .854) kidneys. No changes in HR (p = .908) or MAP (p = .749) were recorded after the insertion of the IsoWire. The concentration of isoprenaline in the plasma was below the quantification threshold. Ureteroscopy revealed no ureteral lesions.
Outcome Measures for IRP the Entire Sample and by Kidney
IRP, intrarenal pressure; mmHg, millimeters of mercury.
Table Showing the Isoprenaline Effect Time and Percentage IRP Reduction for the Entire Sample and by Kidney
s, seconds; SD, standard deviation; IRP, intrarenal pressure.
Discussion
The physiological IRP in an unobstructed kidney typically falls within the range of 0 to 15 mmHg (0–20 cmH2O). 4 Harmful IRPs are frequently attained during RIRS, leading to patient morbidity. Retrograde translocation of uropathogenic bacteria, caused by pyelorenal reflux, contributes to postoperative pain, acute kidney injury, and fluid overload. 12,13 In addition, the renal fornix, which is the weakest component of the collecting system, ruptures due to the precipitous increase in pressure. 14 For the surgeon, forniceal rupture results in intraoperative bleeding and, consequently, impaired vision. Appropriate strategies for mitigating unsafe IRPs include minimizing irrigation pressure by regulating the flow rate, employing a ureteral access sheath (UAS), ensuring an empty bladder throughout the procedure, and more recently, utilizing real-time IRP monitoring.
The pharmacological modulation of IRP using β-receptor agonists, such as noradrenaline and isoprenaline has been explored. Danuser et al. demonstrated that the frequency of ureteral contractions was reduced by both intravenous (0.01 to 10 mg/kg) and endoluminal (0.1 to 200 μg/mL at a flow rate of 2 mL/minute) isoprenaline infusions. Topical administration altered the amplitude of contractions. However, both drugs exhibited adverse systemic effects. 15 Experimental data were obtained from colleagues in Denmark. Following a dose–response investigation in pigs, Jakobsen et al. concluded that smooth muscle function of the renal pelvis was inhibited by endoluminal administration of isoprenaline at a concentration of 0.1 μg/mL at a perfusion rate of 8 mL/min. Systemic adverse effects and detectable plasma isoprenaline levels were not observed. 16 The same author subsequently performed a ureteroscopy on pigs using a 7.8F semirigid ureteroscope while perfusing the renal pelvis at various rates with either saline alone (control) or saline mixed with 0.1 μg/mL isoprenaline (experiment). Isoprenaline perfusion decreased renal pelvic pressure at all irrigation rates, with the greatest percentage relaxation (from 52 mmHg to 38 mmHg, or 27%, p < 0.001) occurring at an infusion rate of 4 mL/min. 17 This effect of endoluminal isoprenaline (irrigation with isoprenaline at 0.1 μg/mL) on IRP was then replicated in humans by the same research team, with no systemic effects. 18
In a porcine model, our study demonstrated that an isoprenaline-eluting guidewire can safely decrease the IRP. There are two potential explanations for this finding. First, it is believed that β-receptors are abundant on the luminal surface of the upper urinary tract. 19 Endoluminal stimulation of these receptors by isoprenaline, a β-agonist, induces ureteral relaxation by activating protein kinase A and adenylate cyclase, thereby increasing cAMP levels (Fig. 3). 20 Second, Jung et al. also postulated that isoprenaline may affect the pacemaker cells of the upper urinary tract, thereby reducing the amplitude of the ureteral contractions.

Graphical representation of the mechanism of action of isoprenaline.
While previous studies have documented a comparable impact of topical or endoluminal isoprenaline administration on IRP, this study is the first to document the use of a drug-eluting guidewire for isoprenaline delivery.
In addition to the reduction in IRP with the use of endoluminal isoprenaline, it confers another benefit. Ureteral access sheaths (UAS) have become an important weapon in the armamentarium of endourologists. This is reflected in a recent survey of practice patterns of endourologists, which showed that 76% of endourologists routinely use a UAS to aid in treating renal stones. 21 The failure rates of UAS insertion in patients with stones have been reported to be 8.8% for 10/12 Fr UASs and 13% to 20% for 12/14 Fr UASs. 22,23 The failure rates are even higher in patients without stones. 24 Even in the case of a successful UAS insertion, there is a concern for ureteral wall injury and ureteral trauma with an excessive force of UAS insertion. 25 To limit this complication, urologists use a strategy to dilate the ureter, either passively or actively. The active form of dilatation involves the use of various ureteral dilators. These dilators produce a linear shearing force, which causes incisions in the ureteral mucosa. This results in the extravasation of urine and fluid, which can result in fibrosis. 26 A more favored approach is passive dilatation of the ureter by prestenting the patient with a ureteral stent and returning one to two weeks later to manage the stone. An indwelling ureteral stent makes the ureter more distensible and subsequent RIRS easier. 27 However, this prestenting strategy is not without detractors. This entails a two-stage procedure, with time and cost implications. Stent-related symptoms are problematic and can result in reduced quality of life in up to 80% of patients. 28 The presence of an indwelling stent has also been shown to increase the incidence of urosepsis in RIRS. 29
To confer this benefit of passive ureteral dilatation and simultaneously avoid the need to prestent a patient and return for a second procedure, Lildal et al. examined the effect of endoluminal isoprenaline on the success of UAS insertion. Pigs who had initially failed UAS insertion were randomized to endoluminal irrigation with either isoprenaline (0.1 μg/mL) or saline before a second attempt at UAS insertion by surgeons who were blinded. They observed greater success of UAS insertion in the isoprenaline group than in the saline group (63% vs. 27%). 30 Similarly, the use of our IsoWire will lead to subsequent ureteral muscle relaxation, which may facilitate easier insertion of a UAS. It may also decrease IRP during sheathless RIRS or even encourage the adoption of sheathless RIRS as a standard procedure. This finding warrants further investigation.
This study is not without its limitations. For dependent sample t-tests, with a medium effect size and power of 0.8, a sample size of 27 was suggested. With our sample size of 18, the power was only 0.65. Although the study was slightly underpowered, we found significant results with a smaller sample size. Furthermore, the researchers felt the need to adhere to the “three R” principles of animal research (i.e., replacement, reduction, and refinement). 31 These values uphold the principles and practice of using the most humane methods on the smallest number of animals that will permit valid scientific information to be acquired. As previously described, in clinical practice, IRPs can reach thresholds that promote intrarenal reflux. In our study, plasma isoprenaline levels were not detected and no changes in HR or MAP were observed. Even low doses of isoprenaline, as used in our study, can theoretically reach systemic circulation. However, considering that IsoWire releases 7.5 ug of isoprenaline in the first minute, and that the half-life of isoprenaline is brief, this seems unlikely. Lastly, due to the short half-life of isoprenaline (2–5 minutes 11 ), the mean duration of the effect of eluted isoprenaline in our study was limited to 174 seconds, after which the IRP seemed to return to baseline. This may not allow sufficient time to place a UAS. Further studies are needed to explore techniques to prolong this effect time.
Conclusion
Endoluminal isoprenaline administration using an isoprenaline-eluting guidewire (IsoWire) can safely reduce the IRP.
Footnotes
Acknowledgments
The authors acknowledge the invaluable contribution of several individuals: (1) Peter Zilla, Rose Boltman, and Helen Ilsley of Strait Access Technologies, (2) Janet McCullum, John Chipangura, Tashie Makwavarara, and Thireshni Chetty at the University of Cape Town Research Animal Facility, (3) Michelle Henry, at the Numeracy Center, Center for Higher Education Development at the University of Cape Town, and (4) Val Myburgh.
Authors’ Contributions
All authors contributed to the design of the study, analysis of the results, and drafting and revision of the article.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This work was supported by the