
Abstract
Purpose:
To determine if single-port robotic-assisted radical prostatectomy (SP-RARP) has higher rates of incisional hernias when compared with multi-port robotic-assisted radical prostatectomies (MP-RARP).
Materials and Methods:
A retrospective, single-institution review of all consecutive robotic prostatectomy cases between January 2017 and December 2022. Analyzed multi-port and single-port robotic prostatectomies performed by two high-volume surgeons. Measured primary outcome for the development of incisional hernias, as defined by computed tomography imaging and clinical documentation. Multivariable logistic regression was used to determine the effect of the single-port approach on incisional hernia outcomes.
Results:
A total of 493 patients were included in the study (320 SP-RARPs and 173 MP-RARPs). The overall incisional hernia rate was 8.5% (SP-RARP 8.1% vs MP-RARP 9.2%, p = 0.669). A median follow-up time was 16.6 months and a median time from procedure to hernia diagnosis was 7.4 months. SP-RARP had shorter OR time than the MP-RARP (236 minutes vs 276 minutes, p < 0.001). Patients who developed hernias had higher body mass index (BMIs) than those who did not (30.7 vs 29, p = 0.009). Multivariable logistic regression analysis revealed that patients with higher BMI (odds ratio [OR] 1.07, 95% confidence interval [CI] 1.01–1.14) and a history of prior operation (OR 2.23, 95% CI 1.71–4.29) were more likely to develop incisional hernias. Cox regression analysis accounting for the difference in follow-up period demonstrated that SP-RARP 3.4× more likely to develop incisional hernias than MP-RARP (hazard ratio 3.38, 95% CI 1.50–7.58).
Conclusions:
Patients with higher BMIs and prior history of abdominal surgeries are at increased risk of developing postoperative incisional hernias. SP-RARP procedures confer a higher risk of postoperative incisional hernias.
Introduction
Prostate cancer is the most common nonskin malignancy and the second most common cause of cancer-related death of men in the United States. 1 Radical prostatectomy is an accepted treatment for localized prostate cancer with a survival advantage when compared to watchful waiting. 2 Since the introduction of the da Vinci Surgical System in 2000, an increasing proportion of radical prostatectomies have been performed using a robotic approach, making up over 75% of total radical prostatectomies in 2013 with a continued upward trajectory of use. 3
Incisional hernias (IH) occurring at laparoscopy/robotic port and specimen extraction sites are a known complication of multi-port robot-assisted radical prostatectomy (MP-RARP). 4 Most patients with diagnosed IH necessitate surgical repair resulting in increased healthcare costs. 5 In addition, IH can lead to significant morbidity and mortality rate with the risk of incarceration, obstruction, or strangulation of bowel. 6
The da Vinci Single-Port robotic-assisted radical prostatectomy (SP-RARP) was introduced by Intuitive Surgical in 2018 with early adoption at several academic medical centers. 7 –9 The single-port platform featured multiarticulating instruments and a flexible camera all through a single operative trocar with the proposed benefits of minimizing a number of incisions, improved cosmesis, and improved observation within the deep pelvis using a flexible camera. 7,10,11 However, it has been suggested that there is an increased risk of IH with the usage of larger robotic trocars across various types of abdominal operation. 12 In regard to SP-RARP cases, the occurrence of IH has not been well described in the literature, though the Single-port Advanced Research Consortium (SPARC) study recently reported the rate of IH after SP-RARPs was 0.2% out of their 1103 cohort. 13
There is currently a paucity of studies that have investigated the rate of IH after SP-RARP compared to MP-RARP. The aim of this study was to examine the incidence of postoperative IH in patients after undergoing SP-RARP at our institution, whereas identifying other risk factors for this postoperative complication.
Materials and Methods
This study is a retrospective, single-institution review of 565 RARP procedures from January 2017 to December 2022. We exclusively analyzed patients from two high-volume robotic urologic oncology surgeons who have significant clinical experience and familiarity with both the multi-port and single-port robotic platforms. We included only those patients with a new primary diagnosis of prostate cancer without prior treatment who had at least one follow-up visit within 3 months postoperatively. A total of 493 patients (320 SP-RARP and 173 MP-RARP) who underwent primary RARP with or without concomitant bilateral pelvic lymph node dissection via a transperitoneal approach were included for analysis. Patients who underwent extraperitoneal or transvesical approaches were excluded because of anatomically and physiologically different risk of forming postoperative IH after these operative approaches. 14 Additionally, patients who underwent simple prostatectomy for treatment of BPH or salvage oncologic procedures were also excluded (Fig. 1). The research described herein was conducted in compliance with the ethical principles outlined in the Declaration of Helsinki and adhered to Health Insurance Portability and Accountability Act policies. This retrospective human subjects clinical outcomes study was approved by the Institutional Review Board at the University of Alabama at Birmingham (IRB# 141001004).
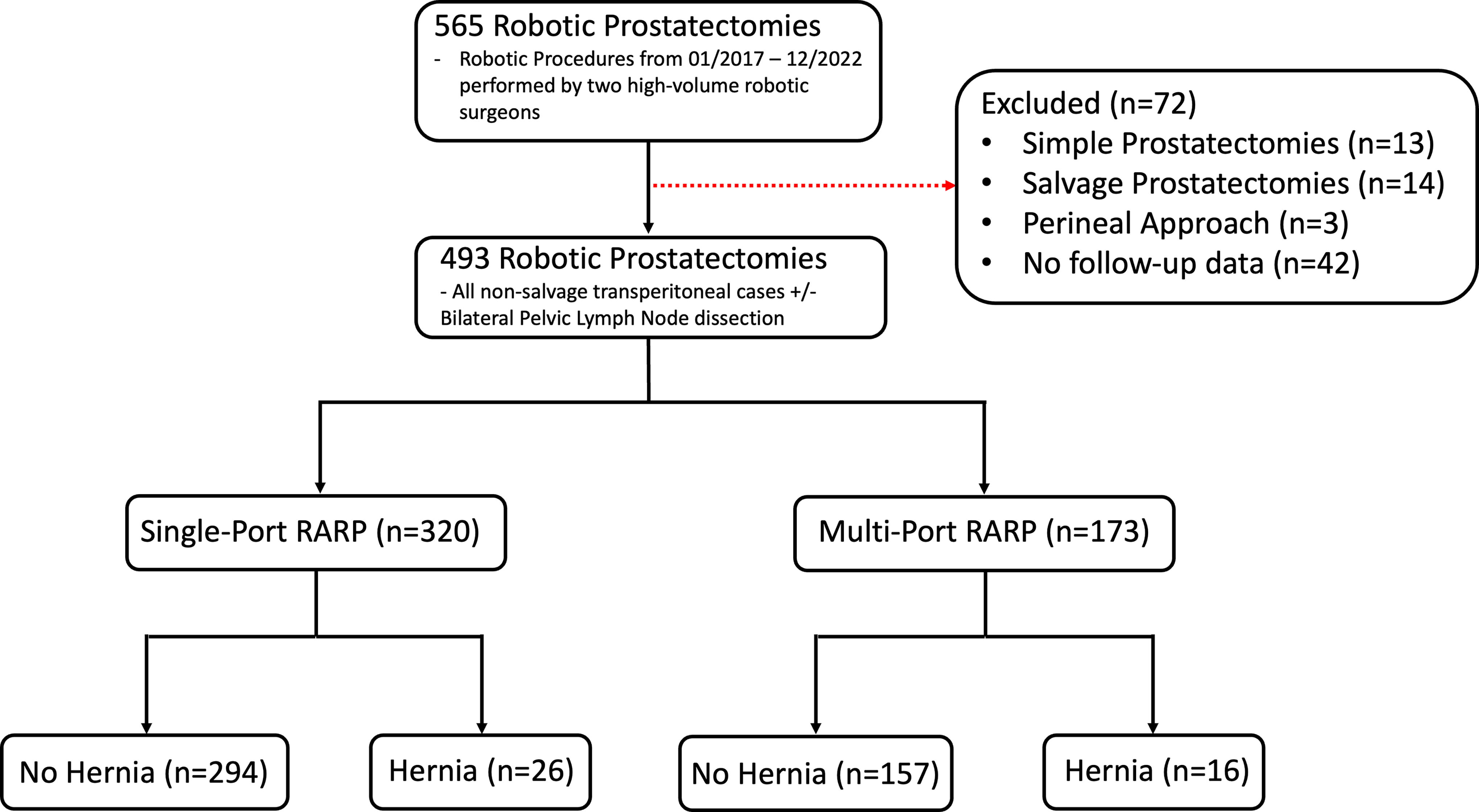
Consort diagram. Reviewed a total of 565 robotic prostatectomy procedures from January 2017 to December 2022. Excluded patients (n = 72) who had salvage procedures, had simple prostatectomies, had a nontransperitoneal approach (i.e., extraperitoneal or transvesical), or who did not have follow-up data. This left a total of 320 single-port and 173 multi-port robotic-assisted radical prostatectomies.
The decision for patients to undergo either MP-RARP or SP-RARP was based solely on surgeon preference and robotic console availability, with the vast majority of SP-RARPs being performed after the introduction of the Intuitive daVinci Single-port robotic platform to our institution in January 2019. All multi-port robotic surgeries were performed using a 12 mm or 8 mm vertical midline skin incision, supraumbilical camera port with the Si or Xi systems, respectively. Additionally, two 8-mm trocars are placed roughly 7–8cm lateral to the camera port on either side or an additional right-sided 8-mm trocar that is placed 8-cm inferior-laterally just superior to the superior iliac spine on the right. Additionally, a 12-mm assistant trocar was placed on the left lower quadrant roughly 3-cm superior to the iliac crest, and a 5-mm accessory trocar on the right that is roughly 7–8cm superior-laterally from the camera port. Single-port prostatectomies were achieved via a single 2.2-cm vertical-midline, supraumbilical incision as well as a 12-mm Airseal accessory trocar that was placed in the left abdomen at the interface of the umbilicus. All fascial closures were performed using 0-polydioxane suture in a running continuous technique.
Patient demographics, history, surgical parameters, pathology, and postoperative outcomes were recorded. The primary outcome for this study was the occurrence of IH that was diagnosed via clinical assessment and physical examination findings as noted in postoperative chart review, or if available, via official postoperative computed tomography (CT) imaging reports. Findings of inguinal hernias were not included in this analysis. Secondary outcomes such as operating room time (defined as interval between incision and closing) and estimated blood loss (EBL) were obtained from anesthesia postoperative reports. Prostate size and tumor staging were obtained from pathology reports.
Descriptive statistics such as frequency, median, and interquartile ranges were performed on demographic and clinical variables. All continuous variables such as age, body mass index (BMI) (kg/m2), EBL, operating room time, and prostate weight were compared using Mann–Whitney tests. All categorical data such as ethnicity, development of IH, and tumor stage were compared using Chi-Square tests. We compared all single-port vs multi-port prostatectomies. Additionally, within each cohort, we compared patients who developed hernias postoperatively vs those who did not. Multivariate logistic regression models for the outcome of IH were fitted for variables with p-values <0.05. 95% confidence intervals for odds ratios were obtained. To account for the variation in follow-up durations within the cohort, a Cox regression analysis was also performed using the same variables that were included in the multivariable logistic regression model. Statistical significance was defined by a two-sided p value <0.05. All statistical analyses were performed using R for Statistical Computing (R Foundation, version 4.04).
Results
A total of 493 patients were included in the study with 320 SP-RARPs and 173 MP-RARPs. The majority of patients were Caucasian (n = 326, 66.1%) with an average age of 64.1 years. The overall incidence rate of IH was 8.5% (n = 42). No significant difference in the rate of IH (8.1% vs 9.2%) was observed between SP-RARP and MP-RARP, respectively (p = 0.669). There was no major difference in age (p = 0.115), ethnicity (p = 0.835), history of prior hernia repairs (p = 0.805), BMI (p = 0.324), EBL (p = 0.974), or prostate size (p = 0.098), between SP-RARP vs MP-RARP patients. Overall, the median follow-up period 16.6 months. The SP-RARP had a significantly shorter median follow-up period than the MP-RARP cohort (15.1 vs 24.5 months, p < 0.001). The MP-RARP cohort had a higher proportion of patients undergoing bilateral pelvic lymph node dissection (87.3% vs 76.9%, p = 0.005), had longer median operating room times (276 minutes vs 236 minutes, p < 0.001), and higher organ-confined disease defined by pathological T2 stage disease (54.3% vs 38.8%, p = 0.003) than patients who underwent SP-RARP, respectively (Table 1).
Single-Port Versus Multi-Port Robotic-Assisted Prostatectomy Summary Statistics
BMI = body mass index; EBL = estimated blood loss; IQR = interquartile range; N = number; OR time = operating room time.
Within the SP-RARP cohort, men who developed IH had higher median BMIs than those who did not (30.4 vs 29.3; p = 0.035). In addition, SP-RARP patients who developed IH had a higher proportion of prior abdominal operation than patients who did not (57.7% vs 35.1%, p = 0.022). Otherwise, there was no significant difference between patients with documented postoperative IH and nonhernia formers in terms of patient demographics or intraoperative findings. The MP-RARP cohort showed no significant difference between men who developed hernias and nonhernia formers in terms of patient characteristics or intraoperative parameters with the exception that patients who underwent prior hernia repair procedures had higher rates of postprostatectomy IH (37.5% vs 17.2%, p = 0.049) (Table 2).
Hernia Versus Nonhernia Patients Between Single-Port and Multi-Port Robotic-Assisted Platforms
ASA = American Society of Anesthesiologist Classification; BMI = body mass index; EBL = estimated blood loss; IQR = interquartile range; N = number; OR time = operating room time.
When comparing all patients who developed hernias (n = 42) vs those who did not (n = 451), regardless of treatment platform (i.e., single-port or multi-port), hernia patients had significantly longer follow-up periods (23.3 months vs 16.1 months; p = 0.003) and had significantly higher BMIs (30.7 vs 29, p = 0.009) than nonhernia formers (Table 3). A multivariable logistic regression was performed which examined the likelihood of developing IH controlling for factors such as surgical platform, history of prior abdominal operation, diabetes, and smoking status at time of operation. Of these factors, the single-port approach was not associated with an increased risk of developing post-prostatectomy IH (odds ratio [OR] 1.24, 95% confidence interval [CI] 0.63–2.40, p = 0.522). Patients with higher BMI (OR 1.07, 95% CI 1.01–1.14, p = 0.037) and history of prior operation (OR 2.23, 95% CI 1.71–4.29, p = 0.015) were more likely to develop IH (Table 4). A Cox regression controlling for patient follow-up was performed and demonstrated that SP-RARPs were significantly more likely to develop IH than MP-RARPs (hazard ratio [HR] 3.38, 95% CI 1.50–7.58, p = 0.003) (Fig. 2).

Cox Regression Analysis. A Cox regression analysis was performed using the same variables that were included in the multivariable logistic regression model and controlled for differences in follow-up period.
Robotic-Assisted Laparoscopic Prostatectomy No Hernia Versus Hernia Cohorts
BMI = body mass index; EBL = estimated blood loss; IQR = interquartile range; N = number; OR time = operating room time.
Incisional Hernia Multivariate Logistic Regression Model
BMI = body mass index; CI = confidence interval; OR = odds ratio.
Of the patients who developed IH within the MP-RARP cohort with documented hernia site information (n = 15), all of them were located at the umbilical incision extraction site. The median time from operation to hernia diagnosis within the MP-RARP cohort was 9.2 months. Fourteen of those patients were diagnosed via physical examination during routine follow-up appointments. One patient developed postoperative fascial dehiscence with herniation identified during emergency room evaluation, and a second patient had incidental finding of ventral hernia diagnosed via CT imaging during work-up for cholecystitis. Nine of the 16 MP-RARP patients (56.3%) had symptomatic hernias with subsequent operative repair with mesh. Within the SP-RARP cohort, a total of 26 patients developed IH. The median time from operation to diagnosis was 7.2 months and all patients, except for two, were symptomatic or diagnosed via physical examination during routine follow-up. Two of the patients were underwent CT imaging in the emergency room, one for acute urinary retention with an obstructed foley catheter and the other for a symptomatic incarcerated hernia. Of the 26 SP-RARP hernia patients, 10 (38.5%) underwent operative repair with mesh (Table 5).
Incisional Hernia Outcomes
Total of 42 patients developed incisional hernias. One of the 26 single-port patients who developed an incisional hernia developed an incisional hernia at both the supraumbilical extraction site and the assistant port site. Of the 16 patients within the MP cohort, one patient was diagnosed and underwent hernia repair at outside hospital. The site and location of his hernia was not available from his records to be included in our analysis. Overall, this represents 42 unique incisional hernias.
CT = computed tomography.
Discussion
This study represents one of the largest high-volume, single-institution analyses of SP-RARP to date with a total of 320 patients. We found that the overall rate of IH across both platforms within our cohort was 8.5%. This is consistent with prior research that cites the rate of IH after robotic prostatectomy between 4.8% and 8.6%. 15 –17 Although prior research investigating hernia rates after multi-port robotic prostatectomies has been described, there is a paucity of literature on single-port outcomes. Most recently, a multi-institutional SPARC study reviewed 1,103 SP-RARP procedures that included different surgical approaches (i.e., transperitoneal, extraperitoneal, and transvesical), of which 244 were transperitoneal. In this study, only two IHs were identified over a median follow-up of 11 months, both being transperitoneal. 13 Our study builds on this by also including a comparative arm of patients undergoing multi-port prostatectomy, with a longer median follow-up period of 16.6 months, where all procedures in both arms of the study were performed by the same two high-volume surgeons. The SPARC study concluded that SP-RARP was associated with a low incidence of IH via the transperitoneal approach (1.2%), 13 whereas we found that transperitoneal SP-RARP procedures were still associated with an 8.1% risk of hernia formation after operation.
This provides valuable information for the practicing urologist to counsel patients on the risk of IH formation after robotic prostatectomy no matter which surgical platform is utilized. Additionally, we identified all but one patient who developed an IH that occurred at the midline extraction site. This is consistent with prior research that examined ventral wall hernias after robotic prostatectomies, which found that the majority of all IH occurred at the midline extraction site. 18,19 Another comparative study examining 90-day complications between patients who underwent transvesical and extraperitoneal SP-RARP vs standard transperitoneal MP-RARP found only one case (0.3%) of IH in the MP-RARP cohort and no cases among the SP-RARP cohort. 20 These findings suggest that an extraperitoneal or a transvesical approach in appropriately selected patients may help to reduce this risk.
Longer incision length and larger port sizes have been correlated with an increased risk of developing IH. 21 Prostate weight can be a good surrogate for the length of the incision at the extraction site necessary for specimen retrieval. For example, Chennamsetty et al. found that with every 5 gm increase in prostate volume, there was a 1.13x increased risk of developing IH. 22 Meanwhile, our study did not find any relation in terms of prostate size and the rate of IH. This highlights that more-so than the size of the prostate, surgical technique plays the most important role in preventing the risk of IH. Some researchers suggest that using continuous suture techniques is best for closing supraumbilical incisions, 23 whereas others have recommended interrupted sutures. 16 Additionally, other research has suggested that transverse camera port incisions may help reduce the incidence of IH when compared to midline vertical fasciotomy among patients undergoing MP-RARP. 24 Notably, within our study extraction sites were closed in a continuous, running fashion, and the vast majority of camera port placements were performed via a midline vertical incision which may also be a contributing factor. Further prospective studies will need to be conducted to better determine the best closure techniques, that is, continuous vs interrupted suturing as well as transverse vs vertical fasciotomies, to help reduce the rate of postoperative IH among patients undergoing SP-RARP.
Numerous potential risk factors for hernia formation after robotic prostatectomy have been described such as higher ASA classification, obesity, diabetes, age, smoking, operative duration, prior abdominal operation, and immunosuppression. 17,21,25 –29 Of these factors, we found that higher BMIs and prior abdominal operation were significantly associated with a higher risk for developing IH. Within the SP-RARP cohort, those who developed IH had higher BMI than their counterparts (30.4 vs 29.3, p = 0.035), a finding we did not see with the MP cohort, which could be related to the larger incision. In our overall sample, regardless of surgical platform, patients who developed IHs had higher BMIs than those who did not (30.7 vs 29, p = 0.009) and for every one point increase in BMI we saw an associated 7% increase in the risk for developing IH (OR 1.07, 95% CI 1.03–1.14). Additionally, patients with a history of prior abdominal operation were more likely to develop IH (OR 2.23, 95% CI 1.71–4.29). Although we did not see a significant difference in operation duration between hernia and nonhernia formers, we found that SP-RARP procedures had a significantly shorter operating time compared to MP-RARP (236 minutes vs 276 minutes, p < 0.001). Although this could be related to a higher rate of bilateral pelvic lymph node dissection within the MP-RARP group, our findings suggest that with experience, the single-port robotic platform may reduce operating times. The decision to perform concurrent pelvic lymph node dissection at the time of RARP was derived by evaluating patient-specific data parameters including PSA, biopsy pathology data, clinical stage, preoperative imaging findings, and risk calculators which drove shared decision-making processes with the patients preoperatively.
Prior research has found that the average time interval to develop an IH after robotic operation ranged from 12 to 14.8 months. 16,17,22 The median follow-up time for our patient population was 16.6 months. Given the relative novelty of the single-port robotic platform, the median follow-up period was, unsurprisingly, significantly shorter within the SP-RARP cohort vs the MP-RARP (15.1 months vs 24.5 months, p < 0.0001). This raises the possibility of an underestimation of the true incidence of IH after SP-RARP, which may increase overtime, as suggested by the longer median follow-up time among hernia patients vs nonhernia patients (23.3 months vs 16.1 months, p = 0.003) that we observed within our cohort. To account for this, we performed a cox regression analysis that controlled for differences in follow-up periods and found that SP-RARPs patients were 3.4× more likely than the MP-RARP patients to develop IH (HR 3.38, 95% CI 1.50–7.58). This supports our initial hypothesis that patients who undergo SP-RARP may be more likely to develop IH, possibly because of increased fascial stress and shearing forces associated with the larger robotic trocar.
This study represents one of the highest volume, single-center analyses of single-port robotic radical prostatectomies to date. Limitations of our study include its retrospective design and its relatively short duration of follow-up, as previously discussed. Although all procedures were directly supervised by the same two attending physicians, resident physicians and surgical assistants across different skill levels and stages of training assisted in fascial closures for both SP- and MP-RALPs, which could affect IH rates. Additionally, without the use of standardized postoperative CT imaging, diagnosis of IHs relied on clinical documentation during routine postoperative visits. These clinical evaluations were not standardized or included Valsalva maneuvers and often relied on patient’s self-report symptoms. This leads to the potential of an underreporting of the true incidence of postoperative hernias that may have been subclinical in nature as our analysis mainly relied on patient self-reported symptomatic hernias.
Conclusion
This study represents one of the largest analyses of SP-RARP from a single institution to date. The overall rate of IH after SP-RARP was 8.1%. Patients with prior operative history and obesity were at increased risk for developing IH. SP-RARP is associated with an increased risk of developing IH when compared to MP-RARP. Only transperitoneal approaches were included within our analysis and vast majority of hernias occurred at the midline extraction site. Our findings suggest that urologic surgeons should properly counsel and monitor patients for the development of IHs who undergo either single-port or multi-port RARP via a transperitoneal approach. Future studies are needed to determine long-term hernia rates and optimum closure techniques for patients undergoing SP-RARP across a multicenter prospective study approach.
Footnotes
Authors’ Contributions
J.C.N.: conceptualization of project idea, data curation, formal analysis, writing—original draft, and writing—review and editing; T.C.: data curation and writing—original draft; L.S.: data curation and formal analysis; Z.B.: data curation; J.W.N.: writing—review and editing; A.D.P.: writing—review and editing; S.R.-B.: supervision and writing—review and editing.
Author Disclosure Statement
J.C.N., T.C., L.S., Z.B., A.D.P.: No disclosures to report. J.W.N.: Consulting: Intuitive Surgical. S.R.-B.: Consulting: Intuitive Surgical, Genomic Health Inc, Exact Sciences, MDxHealth, UroViu Corp, Boston Scientific, Blue Earth Diagnostics, Progenics/Lantheus, Photocure, Bayer Healthcare, Tempus, GE Healthcare/BK Medical; Research Funding: NIH, DoD, Mike Slive Foundation, Blue Earth Diagnostics, Astellas.
Funding Information
No additional or outside funding to report for this project.