
Abstract
Background:
To report the surgical and functional outcomes of the holmium laser enucleation of the prostate (HoLEP) surgical program implemented at a high-volume tertiary referral center and to estimate the learning curve (LC) duration for this surgical procedure.
Methods:
Data of all consecutive patients undergoing HoLEP at the University of Verona between June 2022 and April 2024 were retrieved from a prospectively maintained institutional database of patients undergoing benign prostatic hyperplasia (BPH) surgical treatment. The primary endpoint was functional outcomes evaluation during the surgeons’ LC. The secondary endpoint was to define the surgical LC for HoLEP. A multivariable test of means was performed to compare functional outcomes at different time points. After adjusting for potential confounders (age, preoperative pharmacotherapy, and prostate volume), multivariable linear regression models were fitted to evaluate the effect of experience on operative time (OT) and enucleation efficiency. To assess LCs for HoLEP surgery, the non–risk-adjusted cumulative sum (CUSUM) method was used.
Results:
A statistically significant improvement in International Prostate Symptoms Score (IPSS) score, delta% IPSS score, IPSS quality of life (IPSS-QoL) score, and delta% IPSS-QoL score was observed over the study period. Furthermore, the incidence of irritative symptoms (p < 0.001) and stress incontinence (p = 0.01) significantly decreased over time, with a 12-month incidence of 8.4% and 9.5%, respectively. A statistically significant association between experience and both OT and enucleation efficiency was observed in multivariable linear regression analysis. The CUSUM chart for OT and enucleation efficiency showed a steep initial upward/downward trend of ∼50 cases each, and a plateau until ∼100 procedures are reached, where the breakpoint is recognized for both variables and where the CUSUM curve goes below the locally weighted scatterplot smoothing curve in the corresponding observed–expected CUSUM plot.
Conclusions:
HoLEP represents an effective treatment for BPH, demonstrating significant improvement in BPH-related symptoms over the study period, despite the considerable LC of ∼50 cases associated with the procedure.
Introduction
Holmium laser enucleation of the prostate (HoLEP) represents a well-established treatment of benign prostatic hyperplasia (BPH), 1 providing durable functional improvements over extended follow-up periods, 2,3 along with a low rate of surgical retreatment. 4 This technique has garnered significant interest within the urologic community, with an increasing adoption worldwide and a growing number of procedures conducted yearly. 5 –7
Nevertheless, its outcomes are influenced by surgical experience, 8 and its steep learning curve (LC) can represent a significant limitation to a wider adoption of this technique. 9 Indeed, various authors have suggested that a significant number of procedures, sometimes exceeding 50 cases, are necessary to achieve proficiency in this surgical procedure, with a high rate of surgeons discontinuing their involvement. 8,10,11 The analysis of a surgical LC depicts how surgeon’s proficiency affects patient outcomes by modeling a variable representing performance or efficiency as a function of another variable reflecting experience, to monitor trends in healthcare results and estimate the risk of suboptimal outcomes because of the learning process. 12 Different approaches for evaluating the LC exist, and among these, the cumulative sum (CUSUM) method offers a retrospective analysis of a time-ordered sequence of events relative to a specified outcome. This approach effectively detects changes in performance as surgeons accumulate experience, providing real-time insights into their learning progression. 13
The primary aim of the present study was to report the surgical and functional outcomes of the HoLEP surgical program at a high-volume tertiary referral European center and to estimate the LC duration for this surgical procedure.
Materials and Methods
Study population
The study data were retrieved from a prospectively maintained institutional database of patients undergoing BPH surgical treatment. Data of all consecutive patients undergoing HoLEP at the University of Verona between June 2022, when the laser enucleation surgical program began at our institution, and April 2024 were collected into a dedicated data sheet.
The standard preoperative evaluation included medical history, physical examination, administration of the International Prostate Symptoms Score (IPSS) questionnaire, prostate-specific antigen (PSA) testing, uroflowmetry, and abdomen ultrasound (US) for prostate volume estimation. Transrectal ultrasound (TRUS) was obtained whenever feasible for a more precise adenoma measurement. All the indications for bladder outlet obstruction surgery were given according to current guidelines. 1 After receiving adequate counseling regarding potential complications of the approach, every patient provided specific consent for HoLEP. The study was conducted following the principles of the Declaration of Helsinki. Patients with missing data regarding the outcomes of interest and/or incomplete follow-up data were excluded.
Surgical technique
All surgeries were conducted by experienced endourologists, who were well beyond the LC phase for the main endourological procedures 14,15 but novices to HoLEP. The involved surgeons (A.B., A.V.) were mentored for the initial 20 cases by a surgeon (R.R.) who had already completed >50 procedures when the mentoring program commenced, thus overcoming the learning phase. 10 The mentorship program involved gradual and incremental exposure for the trainee, from performing a single lobe to completing the entire procedure in 3–4 cases, depending on their autonomy and learning pace. Subsequently, the trainee performed the procedure independently, with the mentor available for guidance in case of need or intraoperative nuances.
All the procedures were performed with a 26-Ch continuous flow laser resectoscope, a laser fiber stabilizing bridge, a holmium YAG (Ho:YAG) laser generator (Asclepion Laser Technologies GmbH, Jena, Germany) set to 60–120 W, a 550 µm end-firing laser fiber to perform enucleation, and a 26-Fr nephroscope with a tissue morcellator (Asclepion Laser Technologies GmbH, Jena, Germany) to remove the enucleated tissue. The surgical approach used was the modified Gilling technique. 16 According to internal protocol, the catheter was removed one day postoperatively, unless otherwise necessary, and patients were discharged on the same day of its removal.
Study variables
Baseline patient features [age, body mass index, preoperative medical therapy, comorbidities classified according to the Charlson Comorbidity Index (CCI), 17 preoperative maximum flow (Qmax), IPSS and IPSS quality of life (IPSS-QoL), 18 preoperative PSA, preoperative hemoglobin, presence of indwelling catheter, execution and results of preoperative multiparametric MRI (mpMRI) and prostate biopsy, prostate volume measured by mpMRI, abdominal and TRUS, presence of median lobe, and/or bladder stones], intraoperative variables [operative time (OT), enucleation and morcellation time, total kilojoules, weight of morcellated tissue, enucleation efficiency, defined as the ratio between the weight of the specimen and the duration of the enucleation, and the occurrence of intraoperative complications], and postoperative surgical [30 days postoperative complications, graded according to the Clavien–Dindo classification (complications with Clavien–Dindo grade ≥ III considered as “major complications”), 19 length of hospital stay (LOS), catheterization time, 90-day hospital readmission, and identification of incidental prostate cancer] and functional [postoperative PSA, IPSS, IPSS-QoL, Qmax, presence of irritative symptoms with or without urge incontinence (defined as urinary leak concomitant with urinary urgency), and/or stress incontinence (defined as urinary leak with an increase in intra-abdominal pressure), and eventual use of pads, at 3, 6, and 12 months after surgery] data were prospectively collected from the institutional electronic medical records.
The study’s primary endpoint was to analyze the progression of surgical and functional outcomes of HoLEP during the surgeons’ LC. The secondary endpoint was to define the LC for HoLEP, by evaluating how surgeon experience, defined as the number of procedures performed by each surgeon before the patient’s operation, influenced intraoperative variables over the study period.
Statistical analysis
Statistical analysis was conducted following published guidelines. 20,21 Medians and interquartile ranges (IQRs) and proportions and frequencies were adopted to report continuous and categorical variables, respectively.
A multivariable test of means was performed to compare functional outcomes at different time points. After adjusting for potential confounders (age, preoperative pharmacological treatment, and prostate volume), multivariable linear regression models were fitted to evaluate the effect of experience on OT and enucleation efficiency. These variables were chosen for the LC analysis because of their widespread literature use and objective measurability. Assuming a nonlinear effect of the experience on outcomes attributable to the learning process, the experience was modeled using restricted cubic splines where this condition was verified. Model-derived coefficients were used to compute estimated OT and enucleation efficiency. The non–risk-adjusted CUSUM method was used to assess LCs for HoLEP surgery. The standard CUSUM curve for OT and enucleation efficiency was generated. Subsequently, the observed–expected CUSUM curve (O-E CUSUM), was generated using predicted values from the previously plotted predictive models for each outcome. Locally weighted scatterplot smoothing (LOWESS) smoothers were applied to the O-E CUSUM plots to help visualize trends in the curve. Statistical analysis was performed using Stata® 17.0 software (StataCorp LLC, College Station, TX, USA), with statistical significance set at p < 0.05.
Results
Study population
Two hundred thirty-nine patients underwent HoLEP at our institution during the study period. The patients had a median age of 70 years (IQR: 63–75). Most patients (70.7%) received pharmacotherapy before surgical intervention, and 31.4% had an indwelling catheter. Preoperative median IPSS and IPSS-QoL scores were 17 (IQR: 12.5–22) and 4 (IQR: 4–5), respectively, with a median Qmax of 9 mL/sec (IQR: 6–12), a median PSA of 4.1 ng/mL (IQR: 2.4–7.4), and a median prostate volume of 84 mL (IQR: 75–95) as measured by TRUS (Table 1).
Baseline Features
Continuous variables are presented as median (IQR); categorical variables are presented as number (%).
ASA = American Society of Anesthesiologists; CCI = Charlson Comorbidity Index; Hb = hemoglobin; IPSS = International Prostatic Symptoms Score; IQR = interquartile range; mpMRI = multiparametric MRI; PIRADS, Prostate Imaging Reporting and Data System; PSA = prostate-specific antigen; PVR = postvoid residual; Qmax = maximum flow; QoL = quality of life; TRUS = transrectal ultrasound; US = ultrasound.
Surgical outcomes
In the overall cohort, the median OT was 101.5 minutes (IQR: 75–145), with a median enucleation time and a median morcellation time of 65 minutes (IQR: 45–97) and 10 minutes (IQR: 8–15), respectively. The median enucleated tissue weight was 46 g (IQR: 30–70), with a median enucleation efficiency of 0.78 g/min (IQR: 0.44–1.13). The median time to catheter removal was 1 day (1–2), with a median LOS of 2 (1–2) days. Surgical outcomes are detailed in Supplementary Table S1.
Functional outcomes
A statistically significant improvement in IPSS score was observed over time (p < 0.001), with delta% IPSS score improvements of 45.8% (25–58.6), 53.8% (36.4–66.7), and 57.1% (38.5–66.7) at 3, 6, and 12 months postoperatively, respectively (p < 0.01). Similarly, IPSS-QoL score significantly improved during the study period (p < 0.001), with delta% IPSS-QoL score improvements of 60% (50–75), 75% (50–100), and 80% (66.7–100) at 3, 6, and 12 months postoperatively, respectively (p < 0.01). Furthermore, the incidence of irritative symptoms (p < 0.001) and stress incontinence (p = 0.01) significantly decreased over time, with a 12-month incidence of 8.4% and 9.5%, respectively (Table 2).
Functional Outcomes
Continuous variables are presented as median (IQR); categorical variables are presented as number (%).
Bold values indicate statistically significant results.
Learning curve analysis
A statistically significant linear relationship emerged between experience and OT, with a regression coefficient of −0.27 (95% confidence interval: −0.45; −0.08, p = 0.006). On the contrary, the association between enucleation efficiency and experience demonstrated nonlinearity. When testing all spline terms, a statistically significant relationship between enucleation efficiency and experience emerged at multivariable linear regression analysis (all p < 0.05) (Table 3).
Study Variable and Multivariable Linear Regression Predicting Operative Time and Enucleation Efficiency
Modeled as restricted cubic spline, p-value computed using simultaneous test for all splines terms.
Bold values indicate statistically significant results.
CI = confidence interval.
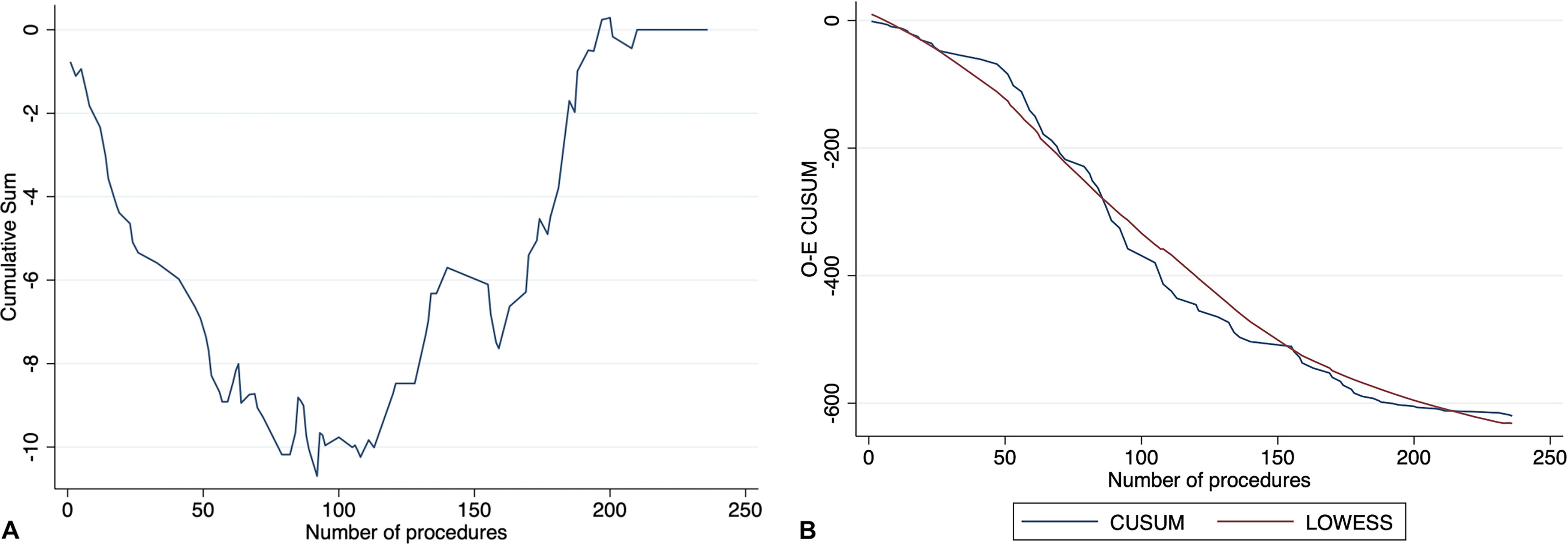
The CUSUM chart for OT showed an upward trend with three points at which the CUSUM curve breaks, identifying four phases of ∼50 cases each (Fig. 1A). The corresponding O-E CUSUM curve reaches a plateau phase at each breakpoint, surpassing the LOWESS line before 100 cases (Fig. 1B). Similarly, the CUSUM curve for enucleation efficiency can be divided into four stages of ∼50 cases each, with an initial steep downward trend, and a plateau until ∼100 procedures are reached, where the breakpoint is recognized (Fig. 2A), and where the CUSUM curve goes below the LOWESS curve in the corresponding O-E CUSUM plot (Fig. 2B).

Graphical plot of learning curve for operative time [
Graphical plot of learning curve for enucleation efficiency [
Discussion
In the present study, a statistically significant improvement in functional outcomes was observed at every time point after HoLEP, despite the ongoing LC, which, according to our results, can be divided into four phases of ∼50 cases each. Our findings add to the debate surrounding the utilization of this surgical technique, which is often focused on the procedure’s initial learning and its implications for its widespread adoption.
According to current guidelines, HoLEP should be considered as the new gold standard for the surgical treatment of BPH-related lower urinary tract symptoms in men with large prostates (>80 mL) and as a valid alternative to transurethral resection of the prostate (TURP) for medium-sized glands. 1 However, studies analyzing the LC of HoLEP show great heterogeneity in terms of prostate volume, ranging from 60 to >90 mL. 8,9 This variability is likely caused by the unintentional propensity of surgeons embracing a new technique to start their experience with less challenging procedures. On the other hand, the median prostate volume in our study was ≥80 mL, regardless of the measurement method. Indeed, HoLEP has been fully embraced at our institution, with a complete transition toward this approach to almost completely replace TURP, irrespective of prostate volume, except for cases where patients decline the procedure or do not require prostate adenoma enucleation (i.e., small prostate <30 mL). As a result, the baseline features of our population, including prostate volume, IPSS, and Qmax, are comparable to those reported in other large case series on this surgical technique, 22,23 despite the inclusion of the LC phase. Furthermore, 31.4% of patients in our cohort had an indwelling catheter before surgery, consistent with a recent meta-analysis showing that about 30% of patients undergoing HoLEP have an indwelling catheter. 24
Functional outcomes achieved in our cohort indicate symptom relief, with a Qmax of 23.5 mL/sec at 12 months postoperatively, and a significant improvement of IPSS and IPSS-QoL throughout the study duration. Indeed, it was previously observed that alleviation of symptoms is independent of experience and can be achieved even in the initial stages of the LC. 25 However, nearly 10% of patients experienced either irritative symptoms or stress urinary incontinence 12 months postsurgery, with a significant but slow recovery of urinary continence. This trend is consistent with a similar observation reported by Capogrosso et al. in a single-center single-surgeon case series, where 30%, 17%, and 8.2% of patients still reported some degree of incontinence at 1, 3, and 12 months after surgery, respectively, with baseline continence status being a significant predictor of worse postoperative continence recovery. 26 Nonetheless, according to several studies, preoperative factors, including age and preoperative urgency, are considered the primary predictors of urge urinary incontinence, whereas heterogeneity persists regarding intraoperative variables. Moreover, patients in our cohort experienced slightly poorer outcomes than case series published by groups with more extensive experience in HoLEP. 3,5,22 Indeed, Hout et al., in a recent meta-analysis, observed postoperative urinary incontinence rates ranging between 1% and 3%. 27 Thus, we can anticipate an improvement in terms of functional outcomes with the progression of our experience. It is noteworthy to consider the substantial variability in how postoperative incontinence is defined and the diverse protocols used for follow-up across different studies, which likely contributes to the variability observed in reported incidence rates. Another potential reason for the differences between ours and other case series can be the involvement of a single surgeon in these studies. Indeed, the LC can significantly differ based on various surgeon-related factors. Some surgeons may need more time to master the procedure, and the experiences gained from using different approaches can significantly shape the learning process. In contrast, our choice to analyze pooled results from different surgeons makes our observations less susceptible to individual abilities and, as such, more generalizable. Indeed, we underline the significance of caseload in this procedure and the necessity for specific LC analysis to recognize the risk of suboptimal outcomes. However, despite the numerous studies on LC, uncertainties persist regarding the optimal variables suitable for LC evaluation. A significant association between experience and both OT and enucleation efficiency was observed in this study. These findings mirror previous data adopting these metrics as a surrogate of experience in the LC phase. 8 –11,28,29 The choice of these variables for the present study derived from their widespread use in the literature and their objectivity for analyzing intervention quality during the LC. Furthermore, using multivariable regression analysis and the CUSUM method allowed us to adjust for potential confounders. We opted not to evaluate morcellation time, as previous studies have demonstrated that it does not vary with increasing experience. 8,10,25 Other variables, such as Qmax and IPSS scores, were excluded from the analysis given their low reproducibility and subjectivity. The complication rate has been previously adopted as a proxy for the LC; however, we could not perform a formal LC analysis on this variable because of the low number of events.
Another open question is the number of procedures required to surpass the LC phase. According to some authors, the LC can be overcome with 20 procedures, 30 whereas others indicate that up to 50–60 cases may be required. 8,10 Even, certain analyses propose that the LC may never fully plateau. 11 Jeong et al. observed that reports based on subjective experience suggested that 20–30 cases were sufficient to achieve competency. In contrast, those relying on surgical parameters indicated that at least 50 cases were necessary. 29 The authors attributed this discrepancy to the increased objectivity provided by using surgical metrics, as opposed to the perception of self-confidence in performing the HoLEP procedure. When examining the CUSUM curves of OT and enucleation efficiency, we observe an initial sharp ascent in the CUSUM score, marking the learning phase. Subsequently, the curve plateaus and variations become less pronounced, corresponding to the proficiency attainment. After this, the curves rapidly descend below the predicted scores, indicating the overcoming of the LC. Hence, based on our graphical representation of the LC, these findings sustain the observation that the initial LC phase spans ∼50 cases, with an additional ∼50 cases required to achieve mastery level. Beyond this point, consistent for both the analyzed variables, performance stabilizes, and subsequent cases serve to refine skills, ensuring optimal and consistent surgical outcomes.
Another point worth discussing is the importance of mentorship during the LC phase. Indeed, the presence of a structured mentoring program can shorten the LC and improve the procedure’s safety profile. 11,31 Several studies have reported good results with self-mentorship, demonstrating that supervision is not strictly necessary for achieving good functional outcomes. 8,9,29 However, the active involvement of an experienced surgeon can facilitate the learning process 10 and increase the adoption of the technique. 9 A mentor plays a pivotal role in navigating trainees through pitfalls and caveats that inevitably arise at the start of the LC, regardless of their prior experience. Previous reports suggested that mentor guidance and suggestions were essential only during the initial cases (∼15) when residents first adopted this technique. Moreover, the integration of a standardized approach, structured mentorship, and condensed surgical exposure significantly expedites the LC for residents involved in the procedure. 32,33 Thus, an open issue is determining the ideal number of mentored procedures and devising the most effective strategy for transferring surgical experience to trainees, ensuring adequate exposure, and expediting the LC.
The present study is not devoid of limitations. Although data were prospectively collected, LC analysis was retrospective, introducing selection bias, only partially mitigated by including all consecutive patients treated at our institution since the start of the HoLEP program. Performing HoLEP on every eligible patient, regardless of prostate volume, likely maximized the exposition and expedited the learning curve for the surgeons involved. However, this approach may have resulted in treating smaller glands and achieving lower enucleated volumes. On the other hand, the absence of a structured predefined mentorship program in our study protocol could lead to an overestimation of the LC. The low resected weight we reported, compared to the preoperative prostate volume, can be attributed to the existing variability between the preoperative adenoma volume planned for removal and the postoperative enucleated volume. This discrepancy can occur because of tissue loss during morcellation, vaporization during laser enucleation, and volume reduction from loss of blood supply postenucleation. These factors can lead to an underestimation of the enucleated volume, suggesting that the true volume of the adenoma removed is likely over 30% greater than the weight of the postoperative specimen in HoLEP. 34 Moreover, our study was conducted at a high-volume tertiary referral center. Thus, the generalizability of our findings to other settings may be limited. Indeed, it is important to consider that initial proctoring for the first 20 cases may be impractical in certain settings, such as private practice. This aspect could have positively influenced the LC duration observed in the present study. Indeed, the implementation of such a structured approach should be tailored to individual centers’ resources and volume. In addition, the relatively short duration of follow-up limits our ability to assess long-term outcomes, although it goes beyond the scope of our study.
Conclusions
HoLEP represents an effective treatment for BPH, demonstrating significant relief in BPH-related symptoms despite the considerable LC associated with the procedure. This underscores the importance of experience in HoLEP, emphasizing the need for tailored mentorship programs to expedite the LC and optimize surgical outcomes.
Footnotes
Authors’ Contributions
Conception or design of the work: F.D., A.V., and A.A. Acquisition, analysis, or interpretation of data: F.D., A.V., A.B., F.F., C.B., S.M., R.R., M.B., E.R., R.A., R.B., and A.A. Drafting the work: F.D. and A.V. Revising the work critically for important intellectual content: A.B., F.F., C.B., S.M., R.R., M.B., E.R., R.A., R.B., and A.A. Final approval of the version to be published: F.D., A.V., A.B., F.F., C.B., S.M., R.R., R.B., E.R., R.A., R.B., and A.A. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: F.D., A.V., A.B., F.F., C.B., S.M., R.R., R.B., E.R., R.A., R.B., and A.A. All authors read and approved the final version of the article.
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided informed consent before participating in the study.
Data Availability
The data sets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the article.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.