
Abstract
Purpose:
Residual stone fragments are common after percutaneous nephrolithotomy (PCNL), however, there is an unclear relationship between the presence of these residual stone fragments and the risk of unplanned stone events (USE). We investigated how the size of the largest residual stone fragment (LRSF) impacts the risk of USE post-PCNL.
Materials and Methods:
We conducted a retrospective cohort study of PCNL between 2018 and 2022. Preoperative computed tomography of the abdomen and pelvis (CTAP) imaging and postoperative CTAP imaging were reviewed. The primary outcome was the incidence of postoperative USE, defined as stone-related emergency department visits or unplanned stone procedures. LRSF were stratified by five thresholds (no postoperative stone fragments vs ≥0 mm, <2 vs ≥2 mm, <3 vs ≥3 mm, <4 vs ≥4 mm, and <5 vs ≥5 mm), and Cox regression was used to compare the impact of these thresholds on the risk of USE.
Results:
After exclusions, we identified 138 patients who underwent PCNL during the study period; 42 patients had a USE. When applying a 4 mm threshold, 52% of patients with LRSF ≥4 mm experienced USE vs 21% with LRSF <4 mm (log-rank p = 0.0004); similarly, with a 5 mm threshold, 62.5% with LRSF ≥5 mm had such events compared with 21% with LRSF <5 mm (log-rank p < 0.00001). A larger LRSF was associated with a greater risk of having a USE.
Conclusion:
After PCNL, larger residual stone fragments, particularly those ≥4 mm, are associated with an increased risk of USE. These results demonstrate the value of identifying residual fragments in predicting USE.
Introduction
Urinary stone disease (USD) is one of the most common urologic conditions affecting patients; with an estimated prevalence within the U.S. of 11%. 1 The incidence and burden of USD are expected to rise, given the rising prevalence of comorbidities that contribute to the development of USD and climate change. 2 Percutaneous nephrolithotomy (PCNL) is indicated for the treatment of USD in which the total stone burden (TSB) within one kidney is >2 cm. 3,4 Given the high stone burden of patients undergoing PCNL, residual stone fragments are common and may result in postoperative symptomatic USD requiring further procedures. Stone-free status (SFS) is not well defined in the literature—some authors use SF to mean no residual fragments while others have used 2 and 4 mm as acceptable cutoffs. A largest residual stone fragment (LRSF) of <2 mm is commonly considered important to achieve to avoid postoperative symptomatic USD or obstructive uropathy. 5
The impact of SFS on the risk of unplanned stone events (USE) (stone-related emergency department [ED] visit or reintervention, and residual stone fragments after PCNL) has been studied by other groups with varying results. 6 –8 A recent multi-institutional cohort study of patients with PCNL found that stone-related reinterventions are higher among patients with >2 and >4 mm residual fragments, 9 while a 2021 meta-analysis failed to find an association between residual fragment size and further stone-related event. 10 Thus, a knowledge gap exists in this area—the relationship between SFS or LRSF size and the risk of an USE after PCNL requires further study. This study aimed to analyze the effect of SFS and LRSF on USE after PCNL.
Materials and Methods
Study design and patient population
We conducted a retrospective cohort study of adult patients (ages >18) who underwent a PCNL for the treatment of USD at our academic medical center from October 2018 to July 2022. At the time of data collection, all included subjects had at least 2 years of follow-up. All PCNL procedures were performed by a single surgeon, as previously described. 11 using standard PCNL—miniature PCNL approaches were not used. In brief, the patient is positioned in split-leg supine, and retrograde access into the target calyx is obtained using flexible ureteroscopy. Ureteral access sheaths are routinely utilized. Needle puncture is performed with bi-planer angulation of the C-arm and using the bulls-eye technique. A 24fr Amplatz sheath was used for all cases. Nephrolithotomy is carried out either using a pneumatic lithotripter or with holmium laser lithotripsy. All patients had a Double-J stent inserted postoperatively for drainage for 7–14 days.
This study received approval from our institution’s research subjects review board. Patients were followed from the time of surgery until August 2023 or the time of their USE, whichever came first. A list of patients who underwent PCNL during the study period was extracted from our institutional electronic medical record (EMR) using current procedural terminology codes 50080–50081. Preoperative computed tomography of the abdomen and pelvis (CTAP) imaging and postoperative CTAP imaging on postoperative day 1 were performed routinely for patients who underwent PCNL. Data was extracted from the EMR through manual review, capturing demographic variables (age at surgery, race/ethnicity, gender), clinical parameters (body mass index [BMI)]), and outcome data (timing of stone-related events). Operative features were collected through a review of operative notes and records. An endourology fellowship-trained endourologist (who also performed all PCNL in this series) manually reviewed all CTAP imaging. All stones on preoperative imaging and all fragments on postoperative imaging were measured in three dimensions on axial (length, width) and sagittal (height) sections using the bone window in order to avoid overestimation of small (<2 mm) stones due to voxel-averaging phenomenon. 12 TSB was calculated as the sum of the longest dimension of all stones or fragments. The primary outcome was an incidence of postoperative USE. Follow-up time was defined as the time between the date of surgery and either the occurrence of a stone-related event or the last clinic visit. Our exclusion criteria were 1) planned secondary stone procedure by time of hospital discharge, defined as a planned second procedure at the end of the procedure or if the patient elected for the secondary procedure after discussion of postoperative day 1 CTAP results; 2) no preoperative CTAP imaging available for analysis, or if the preoperative CTAP was more than 1 year old at the time of surgery and 3) no postoperative CTAP performed.
Operational definitions
For the purposes of our study, we defined an USE as a stone-related ED visit or unplanned stone procedure (e.g., ureteroscopy with laser lithotripsy, extra-corporal shockwave lithotripsy, or cystoscopy with ureteral stent insertion) after PCNL. ED visits for hematuria or non-stone-related complaints were not considered USE, and patients had to have pain in the ipsilateral kidney to be considered USE. USE can occur from the time of surgery to the last follow-up; patients were followed up for at least 2 years. An ED visit with a stone procedure in the same admission was counted as a single event. Residual stone fragments refers to individual stone fragments as measured by postoperative day 1 CTAP. The LRSF was defined as the largest-measuring residual fragment in the axial plane on the postoperative day 1 CTAP.
Statistical analysis
We compared demographic, clinical, and operative features between patients who experienced an USE and those who did not. Student’s t-test and Mann–Whitney U-test were used for continuous variables with normal (i.e., age) and non-normal distributions respectively, while the χ2-test was used for categorical variables. Subsequently, we conducted separate analyses in which the cohort was stratified by five different LRSF thresholds: no postoperative stone fragments (stone free) vs ≥0 mm, <2 vs ≥2 mm, <3 vs ≥3 mm, <4 vs ≥4 mm, and <5 vs ≥5 mm. Note that each analysis is separate from each other and that varying thresholds were compared. Kaplan–Meier survival analysis and the Mantle–Cox log-rank test were used to compare the impact of LRSF threshold on the incidence of USE. Cox proportional hazard models were used to estimate the hazard ratio (HR) and 95% confidence interval (CI) for the risk of USE based on the LRSF threshold. Models were adjusted for confounders based on clinical features associated with USE. Sensitivity analyses included exclusions for stone-free patients. All tests were 2-sided with a significance level of p < 0.05. Statistical analyses were performed using Stata v18 (StataCorp, College Station, TX).
Results
A total of 209 patients underwent PCNL during the study period; of whom 138 (mean age at surgery, 59.8 ± 14.9 years) were included in the analysis after exclusions for missing imaging or planned second procedure. Of the 138 patients in our cohort, 42 underwent an USE, either as a stone-related ED visit (n = 30) and/or required an unplanned stone procedure (n = 25). Presenting chief complaints for USE were flank/abdominal pain (n = 28), urinary infection with obstruction (n = 5), interval stone growth which resulted in subsequent stone procedure (after shared decision making with patient) (n = 7), obstructive uropathy (n = 2). Table 1A shows the demographics of subjects who had USE vs those who did not. Our study population was majority non-Hispanic White (90%), with Hispanic (2%) and non-Hispanic Black (4.4%) patients composing a minority. Patients who had an USE were younger and had a higher median BMI. The median preoperative TSB was 22 mm (IQR: 20.0–35.8), which did not vary significantly between the two groups. Patients who had an USE had a higher median postoperative TSB (7.3 mm, IQR: 1.9–12.9) and higher median LRSF (4.6 mm, IQR: 1.9–7.3) compared with those who did not (3.3 mm, IQR: 0–6.9 and 2.2 mm, IQR: 0–3.6, respectively, p = 0.0023; 0.0003) (Table 1B). The median number of residual stone fragments was 1 (IQR: 0–3), the distribution of the residual stone fragment number is described in Supplementary Figure S1.
Clinical Characteristics (A) and Operative Features (B) Among All Patients, Stratified by the Presence of a Unplanned Stone Event
Bolded p-values indicate significance (p < 0.05). Largest residual fragment refers to stone fragments following percutaneous nephrolithotomy assessed by computed tomography on postoperative day 1. Follow-up time was assessed from index surgery to stone-related events or last follow-up appointment in months. p-Values represent either student’s t-test or the Mann–Whitney U Test for continuous, normally distributed, or non-normally distributed variables, respectively, or the χ2-Test for categorical variables.
IQR, interquartile range.
Table 2 and Figure 1 compare the cumulative incidence of USE based on varying LRSF thresholds. The cumulative incidence of USE fails to reach statistical significance when LRSF thresholds of stone-free vs ≥0 mm, <2 vs ≥2 mm, and <3 vs ≥3 mm are used. When using an LRSF threshold of 4 mm, 52% of patients with LRSF ≥4 mm experienced USE compared with 21% of patients with LRSF <4 mm (log-rank p = 0.0004). Similarly, for patients with LRSF ≥5 mm, 62.5% experienced USE compared with 21% of those with LRSF <5 mm (log-rank p < 0.00001). When we measured the risk of having an USE based on LRSF, we found that having a higher LSRF was associated with having an USE (HR 1.22, 95% CI: 1.12–1.34, p < 0.0001; Table 3). Furthermore, we found that LRSF ≥4 mm or 5 mm had a 3.3- or 4.4-fold increased risk of having an USE compared with LRSF <4 or 5 mm, respectively. When we excluded stone-free patients, we had similar results to our main analyses, see Supplementary Table S2.
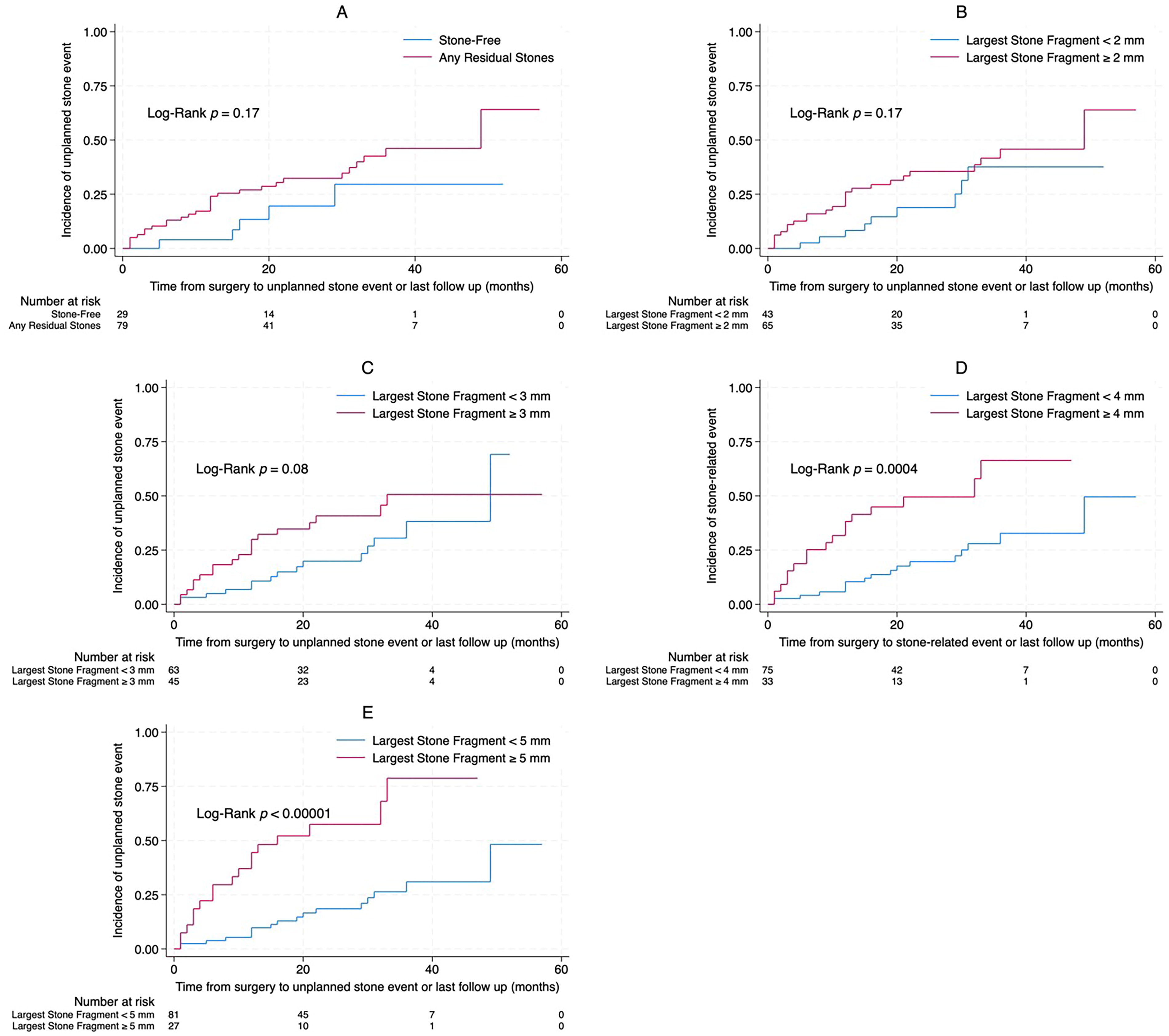
Kaplan–Meier survival analysis comparing the cumulative incidence of unplanned stone events based on different thresholds of a largest residual stone fragment (A, stone-free; B, 2 mm; C, 3 mm; D, 4 mm; E, 5 mm). Stone-free refers to no residual stones remaining when assessed by postoperative day 1 computed tomography.
Relationship Between Unplanned Stone Event and Varying Thresholds of Largest Residual Stone Fragment
Stone-free refers to no residual stones remaining when assessed by postoperative day 1 computed tomography. p-Value refers to the Mantle–Cox log-rank test. Bolded p-values are significant (p < 0.05). Percentages are
Cox Proportional-Hazards Models Estimation of the Hazard Ratio for Unplanned Stone Event During the Follow-Up Period Based on Different Thresholds of Largest Residual Stone Fragment
Stone-free refers to no residual stones remaining when assessed by postoperative day 1 computed tomography. Presented are univariate and age- and body mass index (BMI)-adjusted models. Bolded p-values are significant (p < 0.05).
CI, confidence interval.
Discussion
Patients with a large urinary stone burden often undergo PCNL as it confers the highest stone-free rate. 4 However, residual stone fragments are often left behind due to various factors such as migration into inaccessible parts of the urinary tract, difficulties in visualization due to bleeding, excessive edema due to large stone burden or surgical manipulation and sometimes, residual fragments are too small or radiolucent on intraoperative fluoroscopy. In this study, we explored the association between SFS, various thresholds of residual fragment size, and the risk of USE. We demonstrated that, at certain sizes, residual stone fragments after PCNL are associated with a higher risk of an USE. Upon exploratory analyses, patients who had an USE had larger LRSF and postoperative TSB. While truly stone-free patients did not have a difference in the risk of USE compared with patients with any residual stone fragments, using a threshold of 4 and 5 mm for LRSF corresponded to a significantly higher risk of USE, while smaller thresholds failed to reach statistical significance. In fact, the risk of USE was 3.3× higher in patients with LRSF ≥4 mm and 4.4× higher in patients with LRSF ≥5 mm. Furthermore, we found that younger patients had a higher incidence of USE. This is similar to epidemiological studies finding that younger patients are more likely to have stone events compared with patients who develop stone episodes later in life, possibly reflecting a genetic predisposition to more aggressive USD. 13
Our findings support the existing literature on the relationship between residual stone fragments and post-PCNL reinterventions and stone-related events. Wong et al. similarly demonstrated that individuals with residual fragments >4 mm had significantly higher incidences of stone-related events and subsequent reintervention after PCNL compared with patients with residual fragments <4 mm; (16.2% vs 43.7%, p < 0.0001). 9 Unlike our study, their cohort did not include truly stone-free patients and the composite primary outcome included stone symptoms and renal insufficiency. 9 Emmot et al. 6 examined 723 patients with PCNL and found that individuals with fragments >4 mm were more likely to have a re-intervention (28%). A recent study of 103 subjects found fragments >4 mm had a higher rate of stone-related events compared to those who had fragments <4 mm, although intervention rates in both arms were high compared with patients who were truly stone free (45.7% for >4 mm and 23.5% for <4 mm). 7 Therefore, our study corresponds to the recent literature indicating the higher risk of re-intervention or stone-related event for fragments >4 mm after PCNL. 14
However, other literature examining >4 mm fragments after PCNL and reintervention has failed to find a relationship. A smaller retrospective study of 44 patients who underwent a PCNL and had residual stone fragments failed to find an association between fragment size and risk of a clinical event, although the study may have been underpowered given the small sample size. 8 Furthermore, a meta-analysis performed in 2021 of 18 studies (1996–2021) representing 2096 patients who underwent any stone-procedure (e.g., PCNL, URS, ESWL) found that fragments >4 mm were not associated with an increased risk of subsequent reintervention (odds ratio [OR] = 1.50, 95% CI: 0.70–2.30), however substantial protocol heterogeneity, differences in technology for monitoring stone size throughout the study period, and the variation in stone removal technique may have contributed to the failure to find an association.
Despite being a frequently reported outcome in studies of PCNL, there is no standardized definition for SFS. 5 Some clinicians define SFS as the complete absence of visible or measurable fragments on follow-up imaging, while others argue that a patient can still be considered stone-free with the presence of clinically insignificant residual fragments (CIRFs) on postoperative imaging. 15 Similar to SFS, there is no globally accepted cutoff for CIRF size. 15 In a survey of 44 experts, a majority (56.8%) suggested that CIRFs should be defined as <4 mm. 5 Our results support the opinion of this panel of experts as we did not observe a significantly higher incidence of USE after PCNL until a residual fragment threshold of 4 mm was reached. However, other studies have demonstrated findings that suggest CIRFs be defined as ≤2 mm. Raman et al. 16 found post-PCNL LRSFs >2 mm to be an independent predictor of stone-related events. Similarly, upon stratification of LRSFs into ≤2 and >2 mm groups, Wong et al. 9 demonstrated that patients with LRSFs >2 mm had significantly higher rates of post-PCNL stone-related events compared with those with LRSFs ≤2 mm. Our results failed to determine if LRSF >2 mm is associated with increased stone-events, and support studies which suggest that >4 mm should represent the cut-off for CIRF size.
Like Wong et al. 9 our study included patients who underwent postoperative day 1 CT to identify residual fragments. In the quest for standardization of outcomes data, the Journal of Endourology has specified that postoperative CT be used as the standard for all submitted studies. 17 In recent years, low-dose techniques for reducing radiation dose exposure have greatly reduced the additional risk posed by CT. 18 –21 In addition, urologists performing endoscopy had a low negative predictive value for the detection of fragments <4 mm compared with CT in a cohort of 610 patients with PCNL. 22 In a 2010 study, Raman et al. 23 estimated the cost of expectant management for fragments >4 mm was $4,674 due to the likelihood of USE; this implies that postoperative CT is well justified financially due to better identifying patients at risk of USE and engaging in mitigation efforts or increased surveillance. Our study demonstrates that postoperative day 1 CT after PCNL can meaningfully guide postoperative management by identifying potentially clinically important residual fragments.
Limitations of our study include its retrospective nature, single-center and single-surgeon design, and relatively small sample size. While the majority of our cohort had their follow-up within the same medical system, it is possible that some USE occurred at outside hospitals. In addition, some residual stone fragments may represent pre-existing Randall’s plaque or other renal parenchymal stone disease, which may confound our results. Further limitations include the lack of data regarding the exact location of each residual fragment or the LRSF—this information may affect the rate of USE and represents a key area of future study. We did not have data on stone composition; certain patients with stone types, such as brushite stones, may have a higher likelihood of having recurrent stone formation compared with others. Furthermore, certain USE may reflect individual practice patterns such as the threshold to recommend intervention after stone growth after PCNL. In addition, we did not collect data on the location of the LRFS and examined whether it had an impact on the type of stone event—this remains an area of further study. This study provides evidence to support future prospective studies that examine the effect of the LRFS on USE in which a robust, prespecified analysis could be performed. Advantages of our study include our standardization of operative technique 11 and postoperative protocol: all patients underwent postoperative day 1 CTAP and their immediate postoperative residual stone fragment sizes were known.
Conclusion
Our study underscores the importance of identifying residual stone fragments in predicting USE after PCNL. Larger residual stone fragments, particularly those ≥4 mm or 5 mm are associated with an increased risk of such events. We provide further evidence that standardized definitions for SFS and CIRFs are needed to enhance clinical outcomes and research quality in this field. Further prospective studies with larger sample sizes are warranted to validate these findings and explore the impact of residual stone fragment sizes on outcomes post-PCNL.
Footnotes
Acknowledgments
The authors wish to thank Mare Perevich for assistance with research protocol development.
Authors’ Contributions
D.Z., G.C., C.C., K.M., R.K.J.: data collection. D.Z., K.M.D.: formal analysis. Data interpretation: D.Z., K.M., C.C., G.C., K.M.D., S.O.Q., R.K.J.: data interpretation. D.Z., K.M.: article preparation- first draft. D.Z., K.M., C.C., G.C., K.M.D., S.O.Q., R.K.J.: article preparation—revision. R.K.J.: supervision.
Ethical Disclosure
This study was approved by the Research Subjects Review Board (RSRB) of the University of Rochester Medical Center under RSRB protocol # 7770.
Data Availability Statement
Data supporting this work is not publicly available due to the potential to compromise patient confidentiality.
Author Disclosure Statement
The named authors have no other conflicts of interest, financial or otherwise, to declare.
Funding Information
No external funding was utilized in this study.
Supplementary Material
Supplementary Figure S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.