
Abstract
Objective:
This prospective observational study aimed to explore the predictive value of serum nuclear factor erythroid 2-related factor 2 (Nrf2) levels and its combination with the prognostic nutritional index (PNI) for postoperative sepsis in patients undergoing percutaneous nephrolithotomy (PCNL) for renal stones.
Methods:
This prospective observational study included 112 patients with renal stones who underwent PCNL surgery in our hospital from January 2023 to December 2023. The diagnosis of sepsis was based on the third international consensus definitions for sepsis and septic shock (Sepsis-3). Clinical data on all patients were collected, and the PNI index was calculated. The serum levels of Nrf2, interleukin-6 (IL-6), interleukin-1 beta (IL-1β), tumor necrosis factor alpha (TNF-α), and C-reactive protein (CRP) in all patients were measured using enzyme-linked immunosorbent assay. Data analysis was performed using Statistical Package for the Social Sciences (SPSS) 25.0 statistical software.
Results:
Compared with the nonsepsis patients, the sepsis patients had a higher proportion of positive preoperative urine cultures, longer activated partial thromboplastin time, and lower PNI scores. At 6, 12, and 24 hours after surgery, the sepsis patients had significantly lower serum Nrf2 levels and higher levels of IL-6, IL-1β, TNF-α, and CRP. Pearson’s analysis showed a negative correlation between serum Nrf2 levels and IL-6 and CRP levels. The combination of PNI and serum Nrf2 levels at 24 hours after surgery had a higher predictive level, with an Area Under the Curve (AUC) of 0.844, a sensitivity of 75.3%, and a specificity of 77.8%. Finally, logistic regression analysis showed that decreased serum Nrf2 level at 24 hours after surgery was a risk factor for postoperative sepsis in renal stone patients.
Conclusion:
In conclusion, our study results indicate significantly lower serum Nrf2 levels in postoperative sepsis patients undergoing PCNL. Serum Nrf2 levels in combination with PNI can be used to predict the occurrence of postoperative sepsis in renal stone patients undergoing PCNL.
Introduction
Renal stones, also known as renal calculi, are common urinary tract disorders characterized by the formation of hard deposits in the kidneys. These stones can cause severe pain and discomfort, leading to the need for intervention. 1,2 Percutaneous nephrolithotomy (PCNL) is a minimally invasive surgical procedure commonly used for the removal of renal stones. 3 However, one potential complication of PCNL is the development of sepsis, a life-threatening condition characterized by a systemic inflammatory response to infection. 4,5 It has been reported that the incidence of sepsis associated with PCNL ranges from 0.9% to 4.7%, with a mortality rate exceeding 30%. 6,7 Therefore, early prediction and screening of patients at risk of developing sepsis can prompt the medical care team to take necessary measures such as careful monitoring and adjustment of treatment plans to ensure patient safety.
Inflammation is a key aspect of the immune response and plays a critical role in the pathogenesis of sepsis. 8 Inflammatory mediators, such as cytokines, chemokines, and reactive oxygen species, are released in response to infection and act as signaling molecules to recruit immune cells and promote tissue repair. 9 However, an uncontrolled and excessive inflammatory response can lead to tissue damage and organ dysfunction. In sepsis, a dysregulated immune response triggers a systemic inflammatory cascade, resulting in multiple organ failure and, in severe cases, death. 10 Previous studies have demonstrated the role of inflammatory markers such as interleukin-6 (IL-6), interleukin-1 beta (IL-1β), tumor necrosis factor alpha (TNF-α), and C-reactive protein (CRP) in the diagnosis and prognosis prediction of sepsis patients. 11 –13 However, further research is still needed to explore the role of serum markers regulating inflammatory response in sepsis. Nuclear factor erythroid 2-related factor 2 (Nrf2) is a transcription factor that regulates the expression of antioxidant and anti-inflammatory genes. Studies have reported that Nrf2 inhibits cellular inflammatory response by blocking the transcription of proinflammatory cytokines. 14 It has also been shown to be a key regulatory factor for survival in experimental sepsis. 15 However, there have been no clinical studies focusing on the expression and significance of Nrf2 in sepsis patients. The prognostic nutritional index (PNI) is an established clinical marker that reflects both the nutritional and immune status of patients. Calculated using serum albumin (ALB) levels and lymphocyte count, PNI has shown prognostic relevance in various diseases, including inflammatory conditions and sepsis, by indicating nutritional and immunological reserves. Several studies have demonstrated the value of PNI in predicting postoperative complications and mortality rates across multiple clinical settings, thus making it a suitable primary input variable in this study. 16 Moreover, although Nrf2 functions in cellular defense mechanisms, PNI provides a broader assessment of patient resilience and immune readiness, contributing complementary insights into the risk of postoperative sepsis in patients undergoing PCNL.
This prospective observational study aimed to explore the predictive value of serum Nrf2 levels and its combination with the PNI for postoperative sepsis in patients undergoing PCNL for renal stones. Understanding the relationship between Nrf2 and sepsis can provide insights into its underlying mechanisms and potentially identify biomarkers for early detection and intervention.
Methods
Participants
This prospective observational study included 112 patients with renal stones who underwent PCNL surgery in our hospital from January 2023 to December 2023. All patients were diagnosed with renal stones based on clinical ultrasonography or Computed Tomography (CT) examination. Exclusion criteria were as follows: (1) patients who received immunotherapy within 1 month before surgery; (2) patients with a history of acute or chronic infection within the past 14 days; (3) patients who had undergone recent urologic surgery within the last 6 months, as prior surgical intervention may impact baseline inflammatory markers and postoperative recovery outcomes; (4) patients deemed “unable to tolerate surgery” based on a preoperative assessment of significant comorbidities or risk factors that contraindicate anesthesia or surgical intervention; and (5) patients with severe liver, kidney, malignant tumor, cardiovascular dysfunction, or autoimmune diseases.
The diagnosis of sepsis was based on the third international consensus definitions for sepsis and septic shock (Sepsis-3). 17 It is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Sepsis can be diagnosed if the Sequential Organ Failure Assessment (SOFA) score is ≥2 points compared with the baseline (for patients with unknown organ dysfunction, the baseline SOFA score can be assumed to be zero), or if the quick SOFA (qSOFA) score is positive (qSOFA score positivity is defined as the presence of 2 or more qSOFA signs, including systolic blood pressure ≤ 100 mmHg, respiratory rate ≥ 22/min, or altered mental status) at the onset of infection.
All experiments involving human samples in this study were approved by the Ethics Committee of our hospital (ethics no. 202307) and were conducted in accordance with the principles of the Helsinki Declaration. In addition, all patients provided informed consent.
PNI calculation
PNI has been widely validated in surgical and oncology research as an indicator of malnutrition and systemic inflammation, both of which significantly influence postoperative recovery. Before the procedure, all patients had 5 mL of fasting venous blood drawn from the elbow vein. Whole blood analysis was performed using an automated biochemical analyzer (Hitachi 7600, Hitachi Corporation, Japan) to measure white blood cell count, blood lymphocyte (BL) count, hemoglobin, and serum ALB level. The PNI was calculated based on the serum ALB and BL count. PNI = (serum ALB, g/L) + (5 × BL count, 109/L).
Collection of demographic and clinical data
Demographic data, including age, body mass index, gender, and comorbidities (hypertension and diabetes), were collected for all patients. Additionally, intraoperative clinical data were recorded, including preoperative fasting time, preoperative positive urine culture, surgery time, intraoperative blood loss, coagulation indicators prothrombin time and activated partial thromboplastin time (APTT), and occurrence of postoperative sepsis.
Enzyme-linked immunosorbent assay
The levels of serum Nrf2, IL-6, IL-1β, TNF-α, and CRP in all patients were measured using enzyme-linked immunosorbent assay (ELISA). Venous blood samples (5 mL) were collected from the patients before surgery and at 6 h, 12, and 24 hours after surgery. The samples were centrifuged at 2000 g for 15 minutes, and then commercial ELISA kits were used for detection (Nrf2, MBS024775, MyBioSource, range: 62.5–2000 pg/mL; IL-6, MBS175877, MyBioSource, range: 4.69–300 pg/mL; IL-1β, MBS3803011, MyBioSource, range: 50–800 pg/mL; TNF-α, MBS824943, MyBioSource, range: 15.6–1000 pg/mL; CRP, MBS177184, MyBioSource, range: 156–10,000 pg/mL).
Statistical analysis
Data analysis was performed using SPSS 25.0 statistical software (IBM, Armonk, NY, USA). The normal distribution of data was confirmed by Kolmogorov–Smirnov analysis. Normally distributed data were presented as mean ± standard deviation, whereas nonnormally distributed data were presented as median (range). The Mann–Whitney test or Student’s t test was used for comparisons between two groups. The chi-square test was used for proportions. Pearson’s correlation analysis was used to determine the correlation between serum inflammatory factors in patients. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive value of serum Nrf2 levels and PNI scores for sepsis in patients undergoing PCNL surgery for renal stones. In addition, logistic regression analysis was conducted to identify risk factors for postoperative sepsis in patients. A p-value of <0.05 was considered statistically significant.
Results
Basic characteristics of all patients
A total of 112 renal stone patients undergoing PCNL surgery were recruited for this study. Based on the occurrence of sepsis after surgery, the patients were divided into the sepsis group (n = 27) and the nonsepsis group (n = 85). After comparing the demographic and clinical data between the two groups, we found that compared with the nonsepsis patients, the sepsis patients had a higher proportion of positive preoperative urine cultures and longer APTT. In addition, the sepsis patients had significantly lower PNI scores (Table 1, p < 0.05).
Basic Characteristics of All Patients
APTT = activated partial thromboplastin time; BMI = body mass index; Hb = hemoglobin; PNI = prognostic nutritional index; PT = prothrombin time; WBC = white blood cell.
Elevated levels of inflammatory factors in sepsis patients
To further investigate the relationship between serum Nrf2 and cytokines IL-6, IL-1β, TNF-α, CRP levels, and postoperative sepsis in renal stone patients, we measured the serum levels of Nrf2, IL-6, IL-1β, TNF-α, and CRP in all patients before surgery and at 6 h, 12, and 24 hours after surgery using ELISA. As shown in Figure 1, the serum levels of cytokines gradually increased, whereas serum Nrf2 levels decreased in both groups of patients after surgery. Before PCNL, there were no significant differences in serum Nrf2 and inflammatory cytokine levels (IL-6, IL-1β, TNF-α, and CRP) between the two groups. However, at 6, 12, and 24 hours after surgery, the sepsis patients had significantly lower serum Nrf2 levels and higher levels of IL-6, IL-1β, TNF-α, and CRP. Pearson’s analysis showed a negative correlation between serum Nrf2 levels and IL-6 and CRP levels (Table 2).
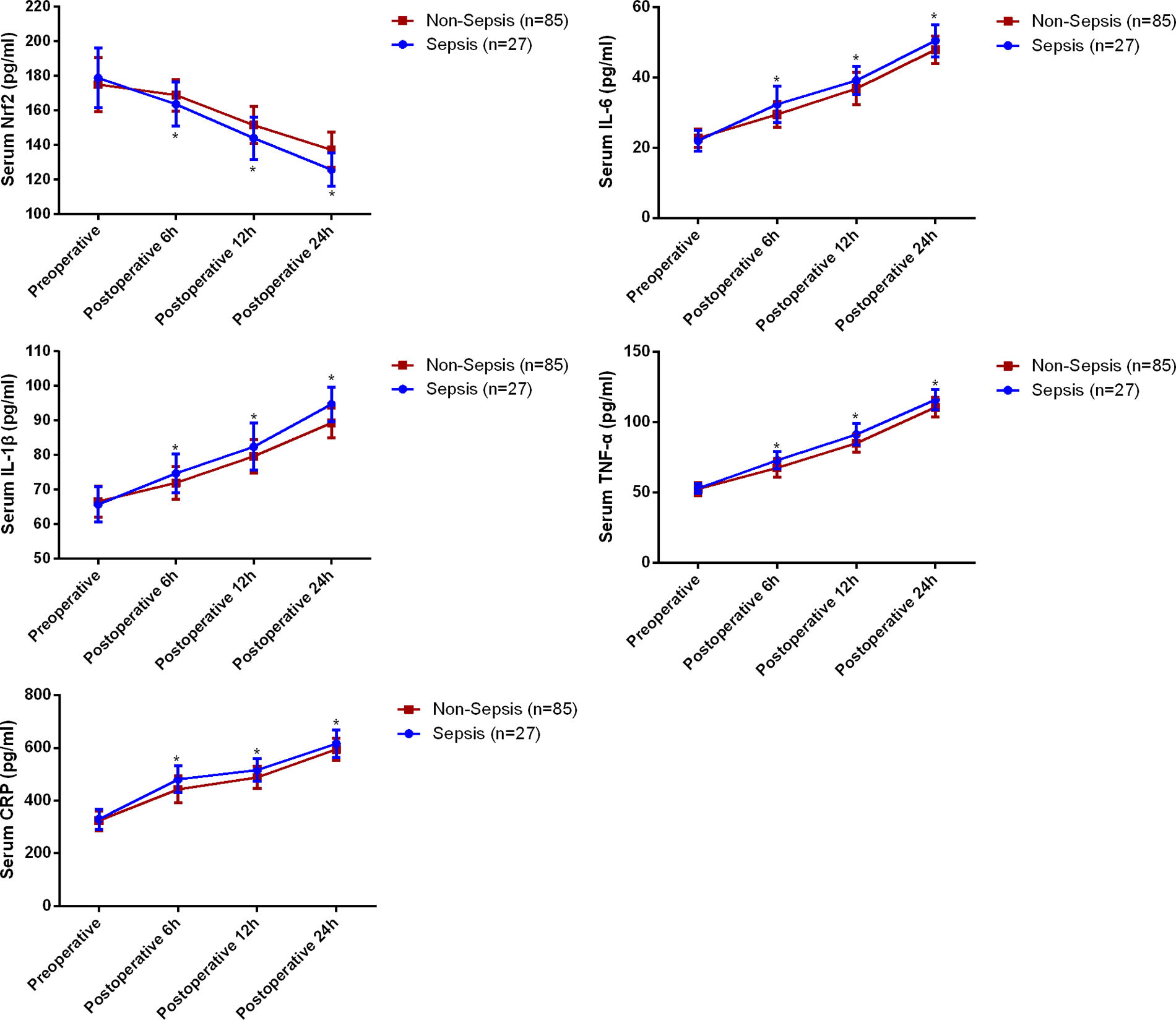
Serum biomarkers of all patients after PCNL. *p < 0.05. PCNL = percutaneous nephrolithotomy.
Pearson Correlation Analysis Among Serum Markers
CRP = C-reactive protein; IL-6 = interleukin-6; IL-1β = interleukin-1 beta; Nrf2 = nuclear factor erythroid 2-related factor 2; TNF-α = tumor necrosis factor.
Furthermore, we divided all patients into a high Nrf2 level group (n = 57) and a low Nrf2 level group (n = 55) based on the median serum Nrf2 level (134.89 pg/mL). As shown in Table 3, compared with the high Nrf2 level group, the low Nrf2 level group had significantly higher serum IL-6 and CRP levels, a higher proportion of sepsis, and a longer hospital stay (p < 0.05).
The Correlation Between Patient Severity, Serum Inflammatory Factor Levels, and Nrf2 Levels
CRP = C-reactive protein; IL-6 = interleukin-6; IL-1β = interleukin-1 beta; Nrf2 = nuclear factor erythroid 2-related factor 2; TNF-α = tumor necrosis factor.
Prognosis predictive value of serum Nrf2 levels for postoperative sepsis in renal stone patients
We plotted ROC curves using serum Nrf2 levels at 6, 12, and 24 hours after surgery to evaluate the predictive value of serum Nrf2 levels for postoperative sepsis in renal stone patients undergoing PCNL. Notably, by the 12-hour mark, Nrf2 levels showed significant predictive ability before clinical symptoms were evident. The results demonstrated that Nrf2 levels at 12 hours postoperatively held predictive value for the occurrence of sepsis, with an AUC of 0.676, a cutoff value of 144.60 pg/mL, a sensitivity of 76.5%, and a specificity of 55.6% (Fig. 2). Among them, serum Nrf2 levels at 24 hours after surgery had a higher predictive value for postoperative sepsis, with an AUC of 0.778, a critical value of 129.57 pg/mL, a sensitivity of 74.1%, and a specificity of 70.4%.

Predictive value of serum Nrf2 levels in postoperative sepsis. Nrf2 = nuclear factor erythroid 2-related factor 2.
Predictive value of PNI combined with serum Nrf2 levels for postoperative sepsis in renal stone patients
Since previous studies have suggested that preoperative PNI scores are potential predictors of sepsis after PCNL, 18 we further analyzed the predictive value of PNI scores for postoperative sepsis in renal stone patients using ROC curves. As shown in Figure 3, the AUC of preoperative PNI for predicting postoperative sepsis was 0.683, with a critical value of 46.95, a sensitivity of 62.4%, and a specificity of 63.0%. Furthermore, we found that the combination of PNI and serum Nrf2 levels at 24 hours after surgery had a higher predictive level, with an AUC of 0.844, a sensitivity of 75.3%, and a specificity of 77.8%.
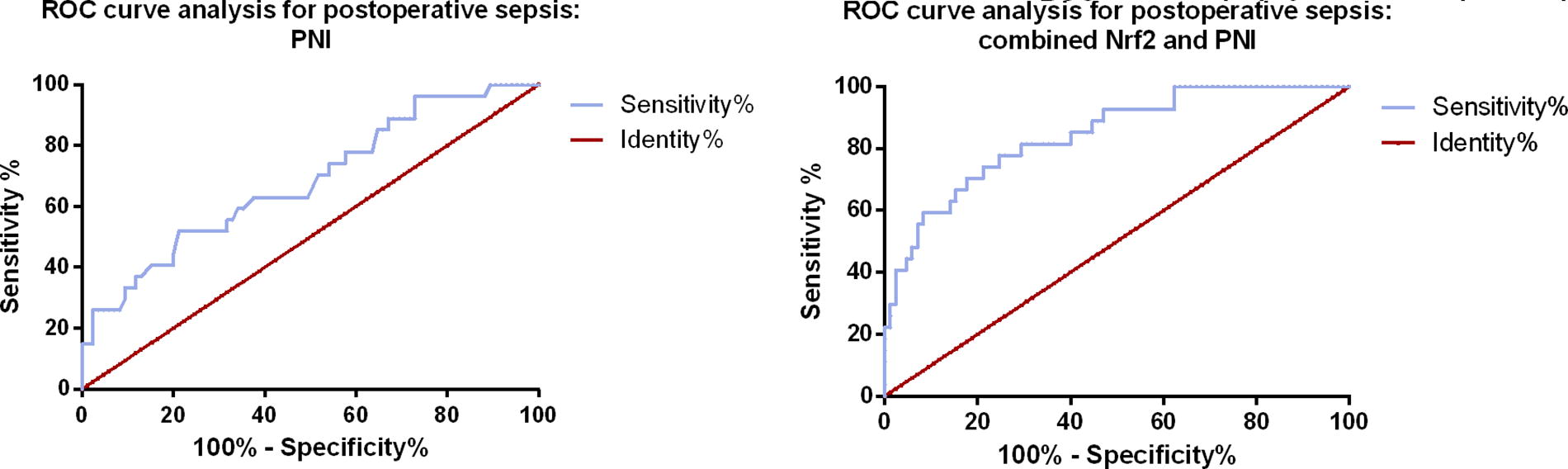
Predictive value of combined serum Nrf2 levels and PNI for postoperative sepsis. PNI = Prognostic Nutritional Index.
Logistic regression analysis of risk factors for postoperative sepsis in renal stone patients undergoing PCNL
Lastly, a multivariable binary logistic regression analysis was performed to identify risk factors for postoperative sepsis in renal stone patients undergoing PCNL. The results, as shown in Table 4, indicated that preoperative urine culture positive, decreased preoperative PNI levels, decreased serum Nrf2 levels at 24 hours after surgery, and increased serum IL-1β levels at 24 hours after surgery were all independent risk factors for postoperative sepsis in renal stone patients (Table 3).
Logistic Regression Analysis for Delayed Healing in Patients with Femoral Neck Fractures
APTT = activated partial thromboplastin time; BMI = body mass index; CI = confidence interval; CRP = C-reactive protein; Hb = hemoglobin; IL-6 = interleukin-6; IL-1β = interleukin-1 beta; Nrf2 = nuclear factor erythroid 2-related factor 2; PCNL = percutaneous nephrolithotomy; PNI = prognostic nutritional index; PT = prothrombin time; TNF-α = tumor necrosis factor alpha; WBC = white blood cell.
Discussion
Sepsis, characterized by systemic inflammatory response syndrome caused by severe infection, is a significant cause of high mortality rates in intensive care unit patients. 19 A cross-sectional study in China demonstrated a high 90-day mortality rate of 35.5% in sepsis patients. 20 Therefore, early prediction of postoperative sepsis in patients is of great importance. In this study, we found that serum Nrf2 levels could be used to predict the occurrence of postoperative sepsis in renal stone patients undergoing PCNL, with further improvement in predictive value when combined with PNI.
Nutritional status is a crucial determinant of immune function and overall health. Malnutrition, characterized by inadequate intake or absorption of essential nutrients, can severely impair immune response and increase susceptibility to infections. 21 In the case of sepsis, malnutrition is associated with a higher risk of developing severe complications and poorer outcomes. Part of the reason is that immune cells in malnourished patients are compromised, leading to a decreased ability to mount effective immune responses against invading pathogens. In addition, malnutrition can result in muscle wasting and organ dysfunction, further exacerbating the severity of sepsis. 22,23 Therefore, assessing and optimizing the nutritional status of sepsis patients are essential to ensure clinical efficacy. For instance, Wang et al. found through multivariable Cox regression analysis that PNI is an important prognostic parameter for hepatocellular carcinoma patients undergoing liver resection. 24 Xiang et al. confirmed that PNI is an independent predictor for 3-month outcomes in patients with acute ischemic stroke. 25 Sun et al. demonstrated through multivariable logistic regression analysis that PNI is an independent predictive indicator for sepsis in patients with diabetic foot ulcers. 26 Our study adds to these findings by showing that preoperative PNI can be used to predict the occurrence of sepsis after PCNL in renal stone patients. The logistic regression analysis also supports that preoperative PNI is a risk factor for postoperative sepsis. Understanding the significance of PNI in renal stone patients undergoing PCNL helps identify patients at higher risk of postoperative sepsis, enabling targeted nutritional support and clinical management.
Nrf2 is a key transcription factor responsible for antioxidant defense in many tissues and cells, and it can inhibit the expression of inflammatory cytokines in macrophages. For example, activation of Nrf2-antioxidant signaling can alleviate Nuclear Factor Kappa-Light-Chain-Enhancer of Activated B Cells (NF-κB)-mediated inflammatory responses and induce cell apoptosis. 27 Moreover, Nrf2 induces the expression of IL-6 through antioxidant response elements in the IL-6 promoter. 28 In our study, we also found a negative correlation between Nrf2 and inflammatory markers IL-6 and CRP levels, suggesting that Nrf2 may suppress inflammatory responses by reducing the expression of inflammatory cytokines in sepsis patients. In clinical studies, Nie et al. found that serum zinc levels and Nrf2 mRNA expression were significantly decreased in diabetic nephropathy patients compared with healthy individuals, and they were associated with more severe clinical and pathological manifestations. 29 Li et al. confirmed a significant correlation between serum Nrf2 protein levels, renal injury severity, and systemic lupus erythematosus disease activity index scores in lupus nephritis patients. 30 Zinovkin et al. also proposed the theoretical basis for using Nrf2 inducers in severely ill patients with COVID-19 to prevent excessive inflammatory responses. 31 In addition, Kong et al. demonstrated in an animal study that Nrf2 is an important immune modulator in leukocytes, controlling the host’s inflammatory response to bacterial infection and preventing sepsis. 32 The ROC curve results of our study demonstrated that the combination of PNI and serum Nrf2 levels at 24 hours postoperatively achieved an AUC of 0.844 for predicting sepsis. This finding reflects a higher sensitivity (75.3% vs 63.9%) but a lower specificity (77.8% vs 93.9%) when compared with the results of Li et al.’s study. 33 This difference highlights the unique predictive contributions and limitations of Nrf2 and PNI in our specific cohort.
In this study, we also found that high serum Nrf2 levels were a protective factor against postoperative sepsis in renal stone patients and could predict the occurrence of postoperative sepsis. Although preoperative Nrf2 levels provided a useful baseline and showed no significant differences between patients who later developed sepsis and those who did not, postoperative changes in Nrf2 levels proved valuable in predicting sepsis onset. Our results demonstrate that elevated postoperative Nrf2 levels correlate with increased sepsis risk, and this predictive capacity was notably enhanced when combined with PNI. This finding suggests that monitoring postoperative Nrf2 levels in conjunction with PNI may improve early sepsis prediction, offering clinicians a more comprehensive assessment tool. Our study identified specific thresholds for Nrf2 levels at the 24-hour postoperative time point that differentiate between protective and at-risk states for postoperative sepsis. ROC analysis indicated that Nrf2 levels above 129.57 pg/mL at 24 postoperative hours were associated with a decreased risk of sepsis, whereas levels below this cutoff posed an increased risk. These defined thresholds provide a basis for clinical risk stratification using Nrf2 measurements at this critical time point. Furthermore, considering that Nrf2 levels were measured using ELISA, interdepartmental variability could pose a challenge in multicenter studies. We recommend that future multicenter research on Nrf2 as a biomarker adopt standardized ELISA protocols, consistent reagent sources, and calibration methods to minimize variability and ensure comparability across study sites. In addition, when considering the clinical applicability of serum Nrf2 and PNI as predictive markers, it is important to acknowledge the potential costs and availability challenges associated with inflammatory marker assays. Although assays such as ELISA are commonly used in tertiary health care and research settings, their routine implementation in smaller clinics may be constrained by financial and technical factors. Future work should explore cost-effective approaches and develop point-of-care tests to increase accessibility, particularly for use in diverse health care settings.
Furthermore, the limitations of our study should be acknowledged. First, it was a single-center study with a small sample size, and the observed sepsis rate of 24% in our study, although higher than that reported in other studies, highlights the variability in postoperative infection rates that may occur across different populations. This elevated rate could reflect unaccounted patient-specific factors such as underlying comorbidities, differing patient demographics, or perioperative variables that were not fully controlled in our analysis. Although we acknowledge this as a limitation, it does not detract from the validity of our findings. Future studies with a larger sample size and more comprehensive control of confounding factors are warranted to confirm the generalizability of our results and to delineate specific risk factors more accurately. This would further clarify the relevance of PNI and Nrf2 as predictive markers for postoperative sepsis in broader patient populations. Furthermore, although our study identified trends in Nrf2 levels as a predictive marker for sepsis onset, the sample size was insufficient to assess correlations with specific clinical outcomes such as mortality. Future studies with larger cohorts are warranted to determine whether reduced Nrf2 levels at 24 hours correlate with the mortality, thereby providing a more comprehensive understanding of the prognostic value of Nrf2 in septic patients. In addition, we only examined a subset of clinical data and inflammatory factors, and there may be other important factors influencing prognosis that were not considered. Finally, the molecular mechanisms by which serum Nrf2 levels affect sepsis necessitate further in-depth study.
Conclusion
In conclusion, our study results indicate significantly lower serum Nrf2 levels in postoperative sepsis patients undergoing PCNL. Serum Nrf2 levels in combination with PNI can be used to predict the occurrence of postoperative sepsis in renal stone patients undergoing PCNL. This study provides clinical evidence for the prevention of postoperative sepsis in renal stone patients undergoing PCNL.
Footnotes
Authors’ Contributions
R.Q.: Conception and design of study. S.Q. and S.H.: Acquisition of data. S.Q. and S.H.: Analysis and interpretation of data. S.Q. and S.H.: Drafting the article. R.Q.: Revising the article critically for important intellectual content. All authors reviewed the article.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this article.