
Abstract
Objective:
Surgical gestures, defined as the smallest meaningful interactions of surgical instruments with tissue, are a novel approach to objectively deconstruct surgery. We have previously classified gestures among three major categories: blunt, sharp, and supporting. Retraction is a supporting gesture, which involves placing tissue on stretch to gain better access to surgical site and to allow tension for effective tissue dissection. We aim to assess utilization and efficacy trends of gestures between these retractions, based on surgeon experience and the anatomical location where gestures are performed.
Methods:
Robotic prostatectomy surgical videos from two centers were captured and manually annotated to identify each surgical gesture, its efficacy and anatomical location, using a classification system previously published. Surgeons were separated by median split—high experience (HE) vs low experience (HE). Sequences of gestures within each sequential retraction gesture were labeled as retraction units (RUs). RUs were split equally into quartiles based on number of gestures in that RU and trends in gesture efficacy were described.
Results:
Overall, 61 surgical videos were annotated to identify 21,045 gestures. Median gestures per case were 222 (interquartile range [IQR]: 163–364) and 337 (IQR: 222–398) for surgeons with HE and LE, respectively. HE surgeons had fewer RUs (p < 0.001), higher gestures per RU (p = 0.031) and greater gesture efficacy (p = 0.023) per RU. There was a significant decline in gesture efficacy for blunt gestures as evaluated from first to last quartile within each RU (p < 0.001). This decline was evident for both HE (p < 0.001) and LE surgeons (p = 0.009) and irrespective of the anatomical location (pedicle, p = 0.04; lateral fascia, p = 0.01).
Conclusion:
Experienced surgeons demonstrated higher gesture efficacy, fewer retractions, and more gestures per RU. Decline in gesture efficacy for blunt gestures is apparent across each RU irrespective of surgeon experience and anatomical location, suggesting re-retract during dissection is an active and dynamic activity.
Introduction
Surgical performance has been correlated with improved clinical outcomes such as reduced post-operative complications and improved continence recovery. 1 –4 We have previously described surgical gestures, which are the moment-to-moment interactions between instruments and tissue during surgery, to objectively quantify surgical performance. 5 –8
Surgical gestures comprise of blunt gestures (for e.g., peel, spread, and hook), sharp gestures (for e.g., cold cut, hot cut, and burn), and supporting gestures (for e.g., retraction). We have also described gesture efficacy as efficacious if the gesture produced its intended effect. By deconstructing surgical procedures into gestures and incorporating their sequences with clinical features, we demonstrated improved prediction of erectile function recovery after radical prostatectomy. 5 Building on this body of work, we aim to extend our gesture classification system by examining their efficacy within the context of retraction gestures
Proper retraction enhances visibility by placing tissue on stretch to stabilize the surgical field, thus enabling effective gesture execution. 9,10 This is particularly important in nerve-sparing prostatectomy, where the preservation of delicate neurovascular bundles is critical. 11 In addition, although gestures are performed, tissue tension enabled by retraction may gradually decrease, causing these gestures to become less effective. Therefore, studying the interplay of retraction and dissection gesture efficacy can provide valuable insights for improving surgical techniques and training programs.
By integrating gesture utilization in the context of retractions, we seek to enhance the understanding of gesture efficacy and how it relates to anatomy during the nerve-sparing prostatectomy. We aim to assess gesture utilization and efficacy trends as the tension resulting from each retraction diminishes, and to explore how these factors vary with surgical experience and the anatomical location where they are performed to inform strategies for optimizing surgical training and improving technical performance during surgery.
Methods
Surgical videos comprising the nerve-sparing step of robot-assisted radical prostatectomy performed at two international centers between 2016 and 2022 were collected. Case-load volume of any robotic surgery was collected from surgeons to establish surgeon experience. Forty procedures were performed with seven surgeons with high experience (HE) (median case-load volume = 2000, interquartile range [IQR] = 2000–4879), while 21 procedures were performed by 11 surgeons with low experience (LE) (median case-load volume = 500, IQR = 150–500). Each surgical video was manually annotated by human annotators (U.G., R.M., J.H., C.Y.), trained on our previously described classification system, to identify and classify surgical gestures. 5 Further annotation was performed to identify each gesture as efficacious or nonefficacious. A gesture was considered efficacious if it produced its intended effect. Anatomical location at which gesture was performed was labeled, which for the nerve-sparing step of prostatectomy comprised predominantly of lateral fascia, pedicle, posterior plane, and apical regions.
Human annotators (U.G., R.M., J.H., C.Y.) underwent a standardized training process to ensure accurate and consistent annotation of surgical gestures and efficacy. The training included a theoretical component, where annotators reviewed our prior classification paper and a detailed guide on gesture classification and efficacy criteria. Practical training sessions were conducted under the direct oversight of the principal investigator and senior research members. During these sessions, annotators practiced gesture classification and efficacy evaluation using surgical videos, with periodic feedback provided to refine accuracy and consistency. To ensure reliability, inter-rater reliability (IRR) was calculated using Cohen’s kappa on a subset of annotated videos. Annotators were only permitted to proceed with annotations after achieving an IRR threshold of ≥0.90 for gesture classification and ≥0.70 for gesture efficacy. Specific details about the classification and efficacy criteria, as well as IRR calculations, are provided in Supplementary Table S1 and Supplementary Figure S1.
Surgeons were classified into HE and LE groups based on median case-load volume of total robotic surgeries performed. Univariable logistic regression was utilized to assess factors associated with high surgical experience. Multivariable analysis was not performed because of multi-collinearity.
A retraction unit (RU) was defined as the sequence of gestures occurring between each sequential retraction gesture (Fig. 1). Each RU was divided internally into four quartiles based on the number of gestures within it. Gesture efficacy for each quartile was pooled and differences in efficacy of each quartile was assessed using chi-square analysis. Gestures were further stratified by type of dissection gesture (blunt/sharp), anatomical location at which the gesture occurred, and surgeon experience. 5 RUs with greater than two positive standard deviations from the mean number of gestures utilized were additionally analyzed as a subgroup to see how they compare with RU with fewer number of gestures.
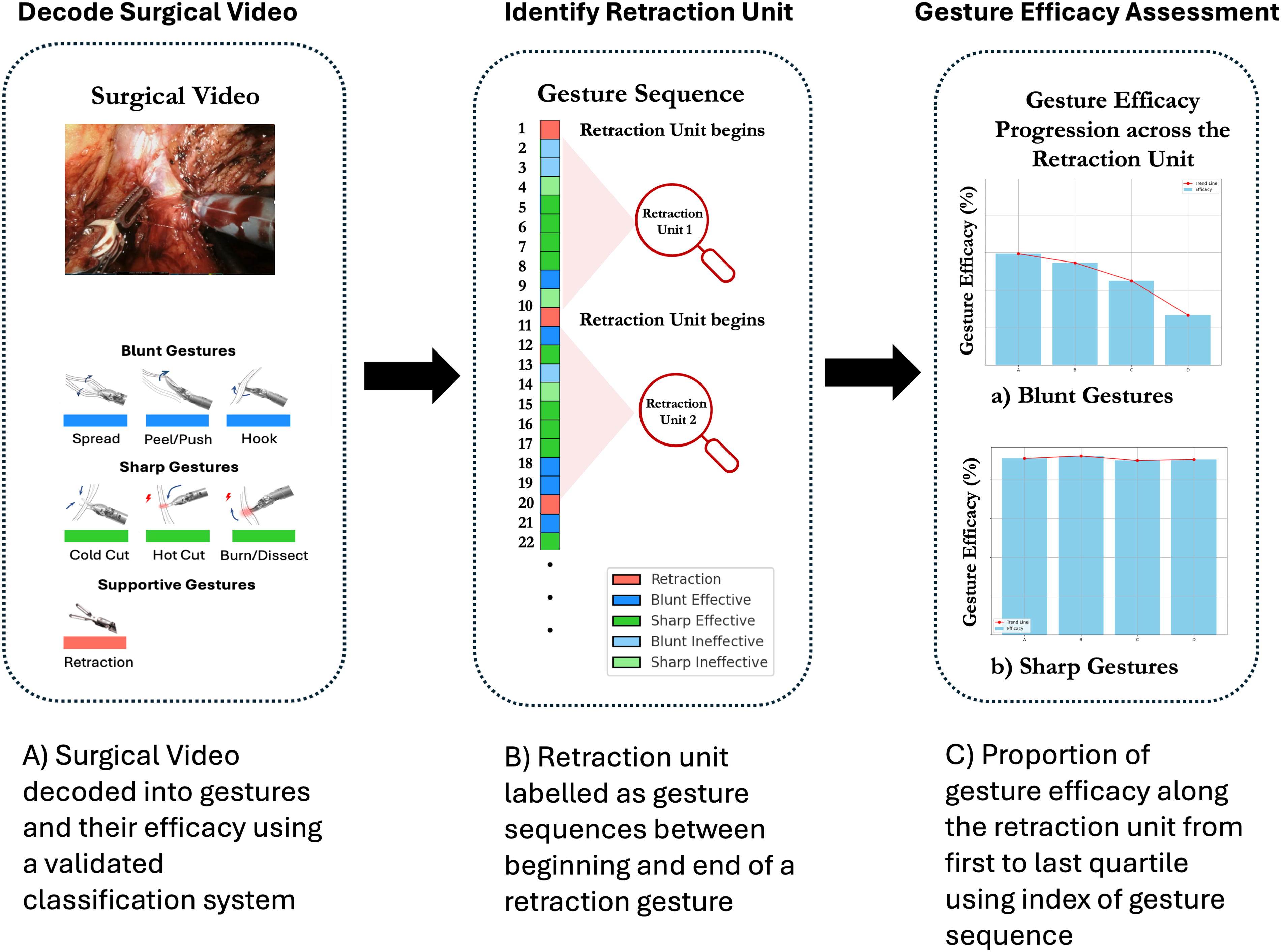
Workflow of decoding surgical videos into surgical gestures and labeling sequences of gestures between retractions as retraction units.
Results
Baseline characteristics
Sixty-one nerve-sparing videos were annotated to identify 21,045 gestures altogether (Table 1). The number of gestures (IQR) per case was 222 for HE (163–364) and 337 (222–398) for LE. Median age was 66 and 64.6 years, respectively, for surgeons with HE and LE, respectively. The median postoperative Gleason score was seven for cases performed by both HE and LE surgeons (p = 0.129). Furthermore, 50% (20/40) of cases performed by HE surgeons were classified as clinical stage T3a or above, compared with 28.6% (6/21) of cases performed by LE surgeons.
Patient Characteristics of Included Nerve-Sparing Robotic Prostatectomy Surgical Videos
BMI = body mass index.
Factors associated with high surgical experience
On univariable logistic regression, high surgeon experience was associated with lower RUs per case (odds ratio [OR]: 0.92; 95% confidence interval [CI]: 0.89–0.96; p < 0.001), greater number of gestures performed within the RU (OR: 1.14; 95% CI: 1.01–1.29; p = 0.031), and higher overall gesture efficacy per RU (OR: 1.04; 95% CI: 1.01–1.07; p = 0.023) (Table 2). Duration of the RU was longer in HE cases but was not significantly associated with surgeon experience (p = 0.089) (Table 2).
Univariable Logistic Regression Model for Factors Associated with High Surgical Experience
IQR = interquartile range; RU = retraction unit; SD = standard deviation.
Gesture efficacy trends
On analysis of all gestures utilized, gesture efficacy significantly declined from first quartile to last quartile (p < 0.001). On stratification by type of gesture, efficacy was significantly decreased over the RU for blunt gestures (65% in Q1 to 57% in Q4; p < 0.001) but not for sharp gestures (p >0.05) (Fig. 2). Efficacy decline during the RU was evident irrespective of the anatomical location at which gestures occurred (prostatic pedicle, p = 0.04; lateral prostatic fascia, p = 0.01) (Fig. 3). When stratified by surgeon experience, both HE and LE surgeons had significant decline in efficacy during the RU (HE, p < 0.001; LE, p = 0.009) (Fig. 3).

Gesture efficacy of retraction unit quartiles for (
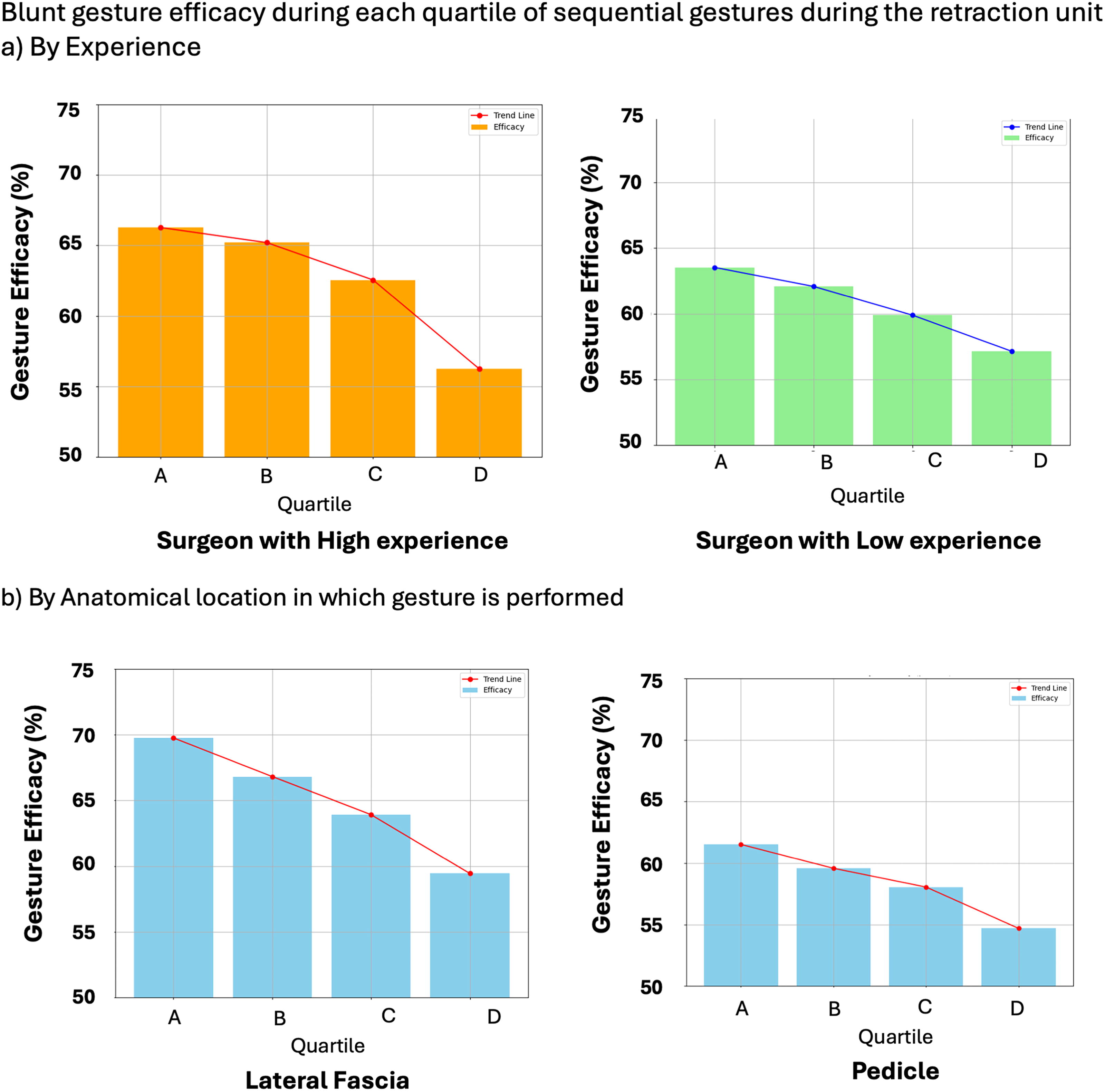
Gesture efficacy of retraction unit quartiles by surgeon experience and anatomical location at which gesture is performed.
Retraction units with higher gesture frequency
We compared efficacy in RUs with high gesture frequency (mean + standard deviation [2SD]) to those with low gesture frequency and found similar gesture efficacy for both groups (p > 0.05). Figure 4 shows two selected examples of gesture counts across an entire nerve-spare step. Across all cases, although outlier RUs show significantly higher gesture counts, there is not a lower rate of gesture efficacy within them.

Illustrative example of gestures across an entire nerve-spare step.
Discussion
This international bi-center study provides context regarding assessment of surgical performance by further studying the gestures utilized by surgeons during the nerve-sparing step of the prostatectomy. We demonstrated distinct gesture usage patterns in surgeons with HE in comparison to LE, including performing fewer retractions, but more efficacious intervening gestures between retractions. We also illustrate the interplay between gestures and their efficacy within the context of the corresponding retraction gesture showing downstream decline of efficacy during the RU, especially with blunt gestures.
Surgeons with HE demonstrated fewer RU than LE surgeons and performed fewer number of gestures during these RU while maintaining higher efficacy. It is plausible that this efficiency may stem from the more experienced surgeons’ ability to perform a more effective initial retraction with optimal tension, reducing the need for frequent re-retraction adjustments. This optimal retraction allows them to execute more relevant and effective gestures to accomplish the same task, thereby minimizing the overall number of retractions required. In addition, experienced surgeons may tend to avoid unnecessary gestures entirely, further enhancing their efficiency.
We observed that efficacy of blunt gestures declines as the RU progresses. Initially, higher tissue tension during retraction may allow for more effective gestures. As the tension loosens, subsequent gestures become less effective, with the least efficacy observed toward the end of the retraction. This necessitates re-retraction to restore optimal conditions for effective gestures. This decline in blunt gesture efficacy is consistent regardless of the anatomical location, highlighting the importance of maintaining effective retraction regardless of the region at which dissection is performed. Pedicle and lateral prostatic fascia as these were the most common anatomical regions where gestures were performed during the nerve-sparing step. This trend was also observed irrespective of the surgeon’s experience, although overall efficacy was higher in the HE groups as anticipated. It highlights the need to re-retract once the surgeon observes declining gesture efficacy during progression of a retraction.
Sharp gestures, on the other hand, do not show a similar significant decline in efficacy as retraction progresses. Sharp gestures concentrate force on a very narrow edge, perhaps making them less reliant on the tissue tension provided by retraction. This consistency in efficacy for sharp gestures across RUs highlights the unique characteristics of sharp gestures and their relative independence from changing tissue tension conditions during surgery. Similarly, no pattern of gesture efficacy for sharp gestures was observed for either anatomical location or surgeon experience.
Analysis of RU with highest frequency of gestures revealed that gesture efficacy remains consistent regardless of the number of gestures performed within the RU. This finding suggests that the quantity of gestures within a retraction unit is not necessarily related to a relative change in efficacy of the gestures within it, provided the retraction is maintained effectively. Our early hypothesis was that peaks of gesture utilization within retraction units were related to surgeons “getting stuck” at a particular aspect of the procedure. This does not appear to be the case based on our results.
Limitations
A relatively small sample size of 61 surgical videos limits the generalizability of the findings, however this is offset by incorporating 18 surgeons from multiple institutions. External validation with data of our findings from an even broader range of institutions is necessary to ensure the findings remain widely applicable. In addition, assessment of gesture efficacy may be deemed subjective, although we have addressed this by formulating a rigorous training protocol with detailed demonstrations of efficacious and nonefficacious examples. Although gesture efficacy is subject to a degree of subjective interpretation, its association with surgical performance highlights its relevance as a meaningful metric. Future efforts to validate and standardize gesture efficacy can help mitigate this limitation and strengthen its potential for clinical applications. In addition, surgeons were classified according to case volume, which might not fully capture the nuances of their surgical expertise. Experience involves more than just the number of cases performed and can include factors such as continuous professional development and varied clinical exposure. Finally, the study focuses on only the nerve-sparing step of prostatectomy. Although the findings provide significant insights into this specific procedure, they may not directly extend to other surgical procedures or steps. Future research should investigate the applicability of these findings across different surgical contexts.
Conclusion
Our study highlights the nuanced interplay between supportive and dissection gestures to enhance our understanding of surgical processes. It highlights distinct patterns of gestures utilized by surgeons of varying experience levels and demonstrates the need for efficient and timely retraction to maintain tissue tension and enable efficacious blunt dissection. Although these insights are specific to this nerve-spare procedure, they open avenues for broader research across various surgical contexts.
Importantly, this research establishes foundational metrics and quantifications of gesture efficacy, which have broader implications for surgical training and machine learning (ML) applications. By offering concrete, objective metrics for surgical gestures, this work paves the way for developing ML/artificial intelligence systems to assess gesture efficacy, providing feedback to surgeons in real time, potentially improving perioperative outcomes, such as reducing operative time and improving precision.
The decline in efficacy over RUs observed in this study, although intuitive, now provides quantifiable insights that can inform future training methods. For instance, training programs could incorporate scenarios where surgeons learn to anticipate and correct declines in gesture efficacy, thereby shortening the learning curve. This research moves beyond description by proposing that these gesture-based metrics could serve as inputs to predictive models aimed at improving patient outcomes, particularly in complex surgeries. Future studies should focus on external validation across a broader range of procedures and institutions, and on assessing whether gesture metrics correlate with outcomes such as recovery times and complication rates.
Footnotes
Authors’ Contributions
Conceptualization: U.G., J.H., R.M., C.Y., C.W., G.G.H., and A.H.; Data curation: U.G., J.H., R.M., C.Y., J.V., and R.T.; Formal analysis: U.G., J.H., R.M., and C.Y.; Methodology: U.G., J.H., R.M., and C.Y.; Visualization: U.G., J.H., R.M., and C.Y.; Writing—original draft: U.G., J.H., R.M., C.Y., J.V., R.T., P.W., E.D., C.W., and A.H.; Supervision: G.G.H., C.W., and A.H.
Author Disclosure Statement
A.J.H. has financial disclosures with Intuitive Surgical, Inc (Sunnyvale, CA, USA) and Teleflex Medical Incorporated (Morrisville, NC, USA). The remaining authors have nothing to disclose.
Funding Information
Research reported in this publication was supported by the National. Cancer Institute of the National Institutes of Health under Award Number R01CA273031.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.