
Abstract
Introduction:
Renal pelvis urine density (RPUD), as measured by computed tomography (CT), may serve as an effective predictor for pyonephrosis. Our objective was to evaluate the correlation between the likelihood of developing infectious complications post-retrograde intrarenal surgery (RIRS) and RPUD measurements obtained from preoperative CT scans.
Materials and Methods:
We retrospectively reviewed data from patients who underwent RIRS for kidney stone treatment at a tertiary care facility between June 2017 and June 2024, using the hospital’s database. The patients were divided into two groups based on the development of postoperative infective complications. The groups were compared in terms of preoperative (demographic data, stone characteristic, and RPUD) and operation data. RPUD was measured by creating an ellipse much as possible area encompassing the renal pelvis on the treated side area encompassing the renal pelvis on the treated side, and the average Hounsfield unit (HU) value was recorded.
Results:
Postoperative infection developed in 31 of 588 patients (5.3%). The median RPUD value was 15 in the infective group and 8 in the noninfective group, with a statistically significant difference between the groups (p = 0.001). Body mass index, stone burden, stone density, and RPUD were associated with postoperative infection in the multivariate analysis (p = 0.001, p = 0.008, p = 0.007, and p = 0.001, respectively). Each unit increase in RPUD increased the risk of postoperative infection 1.107-fold. The receiver operating characteristic (ROC) analysis demonstrated a significant relationship between RPUD value and the risk of postoperative infection, with an area under the curve of 0.742 (p = 0.001). When the RPUD cut-off value was accepted as 14, sensitivity was 0.613 and specificity was 0.779.
Conclusion:
This study showed a significant association between HU values in RPUD and the risk of infectious complications following RIRS. This finding suggests that incorporating urine HU values from CT images into preoperative risk assessment could be crucial for infection prevention and management.
Introduction
In recent years, the role of retrograde intrarenal surgery (RIRS) in treating renal calculi has increased because of advances in minimally invasive technology and the increased use of powerful lasers. RIRS is frequently used to treat kidney stones smaller than 2 cm, as it offers higher success rates than extracorporeal shockwave lithotripsy (SWL) and lower complication rates than percutaneous nephrolithotomy. 1 Although RIRS is a minimally invasive and generally safe method, there is a risk of complications, especially postoperative infection. Rates of infective complications after RIRS range from 2.8% to 7.5%. 2
Various studies have shown relationships between the development of infective complications after RIRS and factors such as operation time, age, renal anomalies, diabetes mellitus, and stone density. 3,4 Many centers routinely obtain preoperative urine cultures from patients to help prevent postoperative infection. However, negative urine cultures may be insufficient to determine infection status, especially in obstructive systems. Basmaci et al. showed that urine cultures were positive in only 49.3% of patients with pyonephrosis. 5 Hydronephrosis and bacterial proliferation in the obstructive system may cause pyonephrosis. Yuruk et al. demonstrated that renal pelvis urine density (RPUD) measured by computed tomography (CT) may be an effective method for predicting pyonephrosis. 6 Surgical interventions on kidney stones in patients with pyonephrosis may increase the risk of postprocedural infectious complications. Supporting this notion, Liu et al. showed that higher RPUD measurements on CT images were associated with an increased risk of infective complications after SWL. 7
The high morbidity and mortality rates of postoperative infective complications underscore the importance of evaluating predictive factors. In this study, we aimed to assess the relationship between the risk of developing infective complications after RIRS and RPUD measurement on preoperative CT.
Materials and Methods
Data of patients who underwent RIRS for kidney stone treatment at a tertiary care institution between June 2017 and June 2024 were retrospectively analyzed using the hospital database. The study was designed in accordance with the Declaration of Helsinki and approved by the local ethics committee (Ethics Committee No: 52-2024). Exclusion criteria included the following: patients younger than 18 years of age; those with JJ stent or nephrostomy before the procedure; patients with infective symptoms (e.g., fever, elevated white blood count, positive urine culture); patients on immunosuppressive medications, those with bilateral kidney stones or solitary kidneys; patients without hydronephrosis; those who underwent procedures without the use of an access sheath; patients without preoperative CT scans; and those with insufficient postoperative follow-up data. Urinalysis data were evaluated to assess the presence of pyuria. Pyuria was defined as the presence of five or more leukocytes in microscopic urine examination. The patients were divided into two groups based on the development of postoperative infective complications. The groups were compared in terms of preoperative and operation data. All patients had a preoperative sterile urine culture. Informed consent was obtained from all patients prior to inclusion in the study.
Preoperative CT imaging was performed using a Philips Ingenuity CT (Philips Medical Systems, Cleveland, OH, USA) scanner with the stone protocol (100 kV, 150 mAs, 2.1 mm slice thickness). Stone characteristics and RPUD were evaluated using preoperative CT scans. Stone size was measured as the widest diameter on CT. Stone burden was calculated using the following formula: stone length × stone width × 3.14 × 0.25. RPUD was measured by creating an ellipse much as possible area encompassing the renal pelvis on the treated side area encompassing the renal pelvis on the treated side, and the average Hounsfield unit (HU) value was recorded (Fig. 1). Two experienced urologists performed each measurement, and in case of discrepancies, the average value was used. Interobserver reliability was assessed using the intraclass correlation coefficient (ICC)
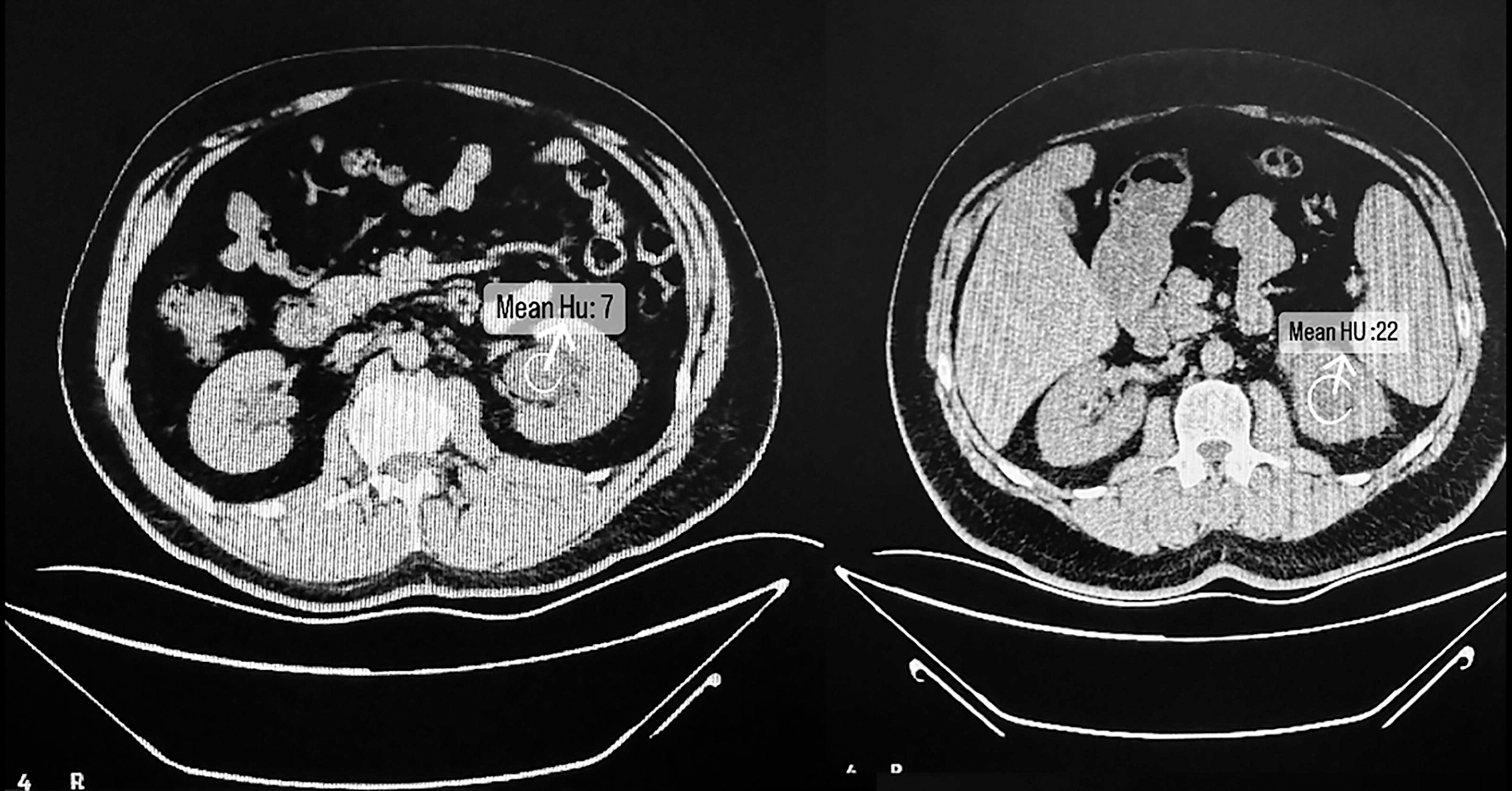
Example of the measurement of RPUD by CT. CR = computed tomography; RPUD = renal pelvis urine density.
The postoperative infection group included patients who exhibited fever, sepsis, or septic shock. Fever was defined as >39°C on the first postoperative day and/or >38°C within the first 48 hours. Sepsis was defined as the presence of an infection source and two positive Systemic Inflammatory Response Syndrome (SIRS) criteria. SIRS criteria included the following: hyperthermia (>38°C) or hypothermia (<36°C); tachycardia (heart rate >90 beats); tachypnea (>20 respirations per minute); leukocytosis (>12,000 β/mm3); or leukopenia (<4000 cells/mm3). Septic shock was defined as the requirement for vasopressor medication to maintain a mean arterial pressure of 65 mm Hg or higher.
RIRS technique
All procedures were performed by the same experienced endourology surgical team. Prophylactic antibiotics were administered to all patients before anesthesia. In the lithotomy position, rigid ureterorenoscopy was performed for active dilatation, followed by placement of an 11–13 Fr ureteral access sheath into the ureter under fluoroscopic guidance. Stone fragmentation was performed using a Ho:YAG laser with a 272 µm probe. Fragmented stones were collected with a basket. A 4.8 Fr JJ stent was placed in all patients after the operation. Operation time was recorded as the duration between ureteral entry with the ureterorenoscope and JJ stent application.
Statistically analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences version 27 (SPSS IBM Corp., Armonk, NY, USA) program. The normality of variable distribution was assessed with the Shapiro–Wilk test and Q-Q plot. The independent student t-test was used to compare normally distributed variables between groups, whereas the Mann–Whitney U test was used for nonnormally distributed data. Quantitative data are presented as mean ± standard deviation or median (interquartile range) values. Categorical variables were compared using the χ2 test or Fisher’s exact test. For factors associated with the development of postoperative infective complications in the univariate analysis, multivariate analysis with a binary logistic regression model was applied. The relationship between RPUD and the development of infective complications was evaluated by ROC analysis. Data were analyzed at a 95% confidence level, and a p-value of less than 0.05 was considered statistically significant.
Results
Comparison of patient characteristics and stone characteristics between groups is shown in Table 1. Postoperative infection developed in 31 of 588 patients (5.3%). There was no statistically significant difference between the groups in terms of age and sex (p = 0.760 and p = 0.896, respectively). Body mass index (BMI) was statistically significantly higher in the infected group (p = 0.001). The mean stone burden was 235.3 mm2 in the infected group and 123.1 mm2 in the noninfected group (p = 0.011). The groups were statistically similar in terms of stone localization, stone opacity, side of operation, and pyuria in preoperative urinalysis. Stone density was statistically significantly lower in the infective group (995.9 vs 838.7; p = 0.001). The median RPUD value was 15 in the infective group and 8 in the noninfective group, with a statistically significant difference between the groups (p = 0.001). Two experienced urologists performed RPUD measurement and the ICC value was 0.937 (95% CI: 0.926–0.946), indicating a high level of agreement.
Comparison of Patients’ Demographic Data and Stone Characteristics
Mean ± standard deviation.
Median (interquartile range).
ASA = American Society of Anesthesiologists; BMI = body mass index; HU = Hounsfield unit.
Bold/italic values indicate statistically significant differences (p < 0.05).
Operative and postoperative data are compared in Table 2. Operative time and stone-free rate were statistically similar between the groups (p = 0.811 and p = 0.183, respectively). Hospital stay was statistically significantly longer in the infective group than in the noninfective group (120 hours vs 24 hours; p = 0.001).
Comparison of Operation Data and Postoperative Follow-Up Results
Mean ± standard deviation.
Median (interquartile range).
Bold/italic values indicate statistically significant differences (p < 0.05).
To evaluate factors associated with the risk of postoperative infection, multivariate analysis was applied to statistically significant data from the univariate analysis (Table 3). BMI, stone burden, stone density, and RPUD were associated with postoperative infection in the multivariate analysis (p = 0.001, p = 0.008, p = 0.007, and p = 0.001, respectively). Each unit increase in RPUD increased the risk of postoperative infection 1.107-fold. The ROC analysis of the relationship between RPUD value and the risk of postoperative infection is shown in Figure 2 (area under the curve [AUC]: 0.742, p = 0.001). When the RPUD cut-off value was accepted as 14, sensitivity was 0.613 and specificity was 0.779. In a multifactorial analysis that included RPUD, stone burden, stone density, and BMI, the AUC was calculated to be 0.863.
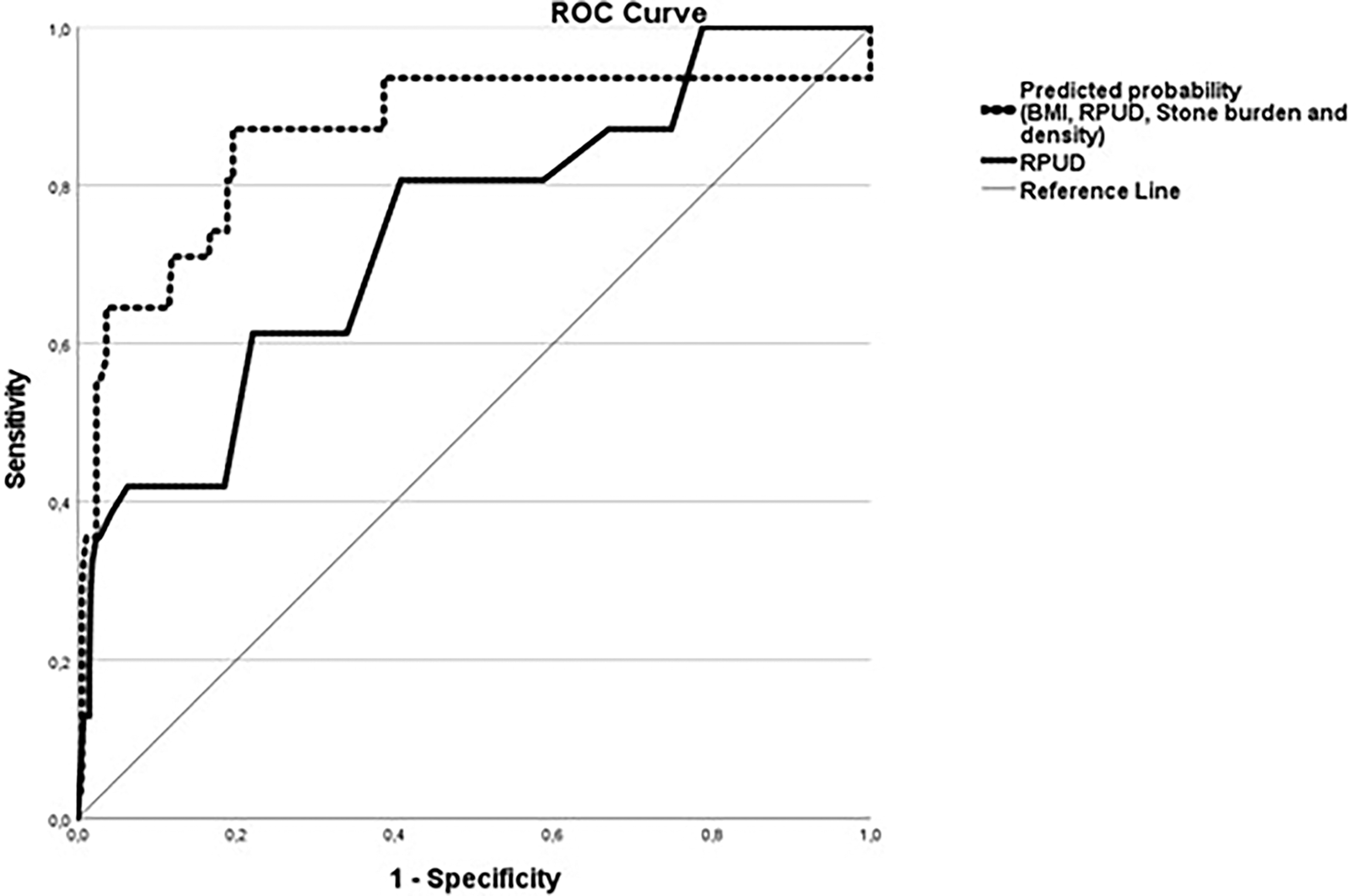
ROC curves for predicting postoperative infectious complications after RIRS: RPUD alone and multifactorial model. RIRS = retrograde intrarenal surgery.
Multivariate Analysis of Factors Related to the Development of Postoperative Infection
CI = confidence interval.
Bold/italic values indicate statistically significant differences (p < 0.05).
Discussion
Infective complication rates after RIRS have been reported to range widely in the literature. 8 This variation may be because of a lack of standardization in classifying the severity of infective complications and deficiencies in reporting these complications. Postoperative infection is associated with prolonged hospitalization, morbidity, and mortality rate. 9 Therefore, predicting postoperative infective complications in the preoperative period is essential. Our study is the first to show the relationship between RPUD calculated on CT before RIRS surgery and postoperative infective complications.
It is known that increased intrarenal pressure occurs during RIRS surgery. 10 Fluid drainage into the venous system after increased pressure in the renal pelvis is defined as pyelovenous reflux and is the pathogenetic mechanism of urosepsis. 11 There is insufficient evidence in the literature regarding the distinction between fluid reflux and bacterial reflux. Especially in obstructed systems, it is challenging to preoperatively predict the bacterial colonization of the pelvic–axial system. The sterility of the preoperative urine culture alone does not provide sufficient evidence.
Evaluation of RPUD in the obstructed pelvic–axial system on CT images has been found to be related to pyonephrosis. 6 Infective complications after SWL have been shown to be more frequent in patients with high RPUD on CT. 7 The results of our study also revealed a relationship between the risk of developing infection after RIRS and RPUD. When the cut-off value for RPUD was 14, we found that it predicted the development of postoperative infective complications with 61% sensitivity and 78% specificity. In light of these results, the use of a drainage method such as nephrostomy before RIRS operation in patients with high RPUD calculated on CT may reduce postoperative complications.
The results of our study showed that, in addition to RPUD, high BMI, high stone burden, and low stone HU values are associated with the development of postoperative infective complications. Struvite stones are known to have a low HU value. 12 Although we did not perform a stone analysis in our study, we attribute the association between low stone HU values and the development of postoperative infective complications to this characteristic. Dybowski et al. identified struvite stones as an independent factor for the development of infection after RIRS in their review. 2
High BMI can lead to insulin resistance and immune suppression, potentially contributing to postoperative infective complications. The literature has presented conflicting results regarding the effect of BMI on infection development after RIRS. Ratajczak et al. found that patients with a BMI above 25 were more susceptible to the development of infective complications after RIRS. 13 Conversely, Kim et al. found that high BMI did not influence the development of infective complications following RIRS. 14
Although this study is the first to show the relationship between the development of infection and RPUD after RIRS, it has some limitations. Its retrospective, single-center design is a primary limitation. We did not evaluate patients’ stone analysis results, and we grouped infective criteria (e.g., fever, septic, septic shock) under a single category. Furthermore, although the RPUD measurements were performed by two experienced urologists, the possibility of human error and interpretation differences cannot be excluded. Another limitation of our study is the lack of data regarding the hydration status of patients at the time of preoperative CT imaging, which may have influenced RPUD measurements. Future prospective studies with larger patient cohorts are needed to corroborate our findings.
Conclusion
This study showed a significant association between HU values in RPUD and the risk of infectious complications following RIRS. This finding suggests that incorporating urine HU values from CT images into preoperative risk assessment could be crucial for infection prevention and management. For high-risk patients, preoperative drainage and broad-spectrum antibiotic administration may be necessary precautions.
Footnotes
Authors’ Contributions
The authors listed below have made substantial contributions to the intellectual content of the article in the various sections described below. Conception and design: U.C. Acquisition of data: C.D. and A.A. Analysis and interpretation of data: C.D., R.Y., and A.A. Drafting of the article: U.C. and U.C.A. Critical revision of the article: F.O. Supervision: F.O. and O.S. All authors approve the final version of the article to be submitted.
Ethics Committee Approval
Local ethics committee of Haseki Training and Research Hospital, Ethics Committee No: 52-2024.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.