
Abstract
Introduction:
The main objective of the study was to demonstrate the noninferiority of the morcellation efficiency (ME) of the Multicut© morcellator compared with the Piranha© morcellator following anatomical endoscopic enucleation of the prostate (AEEP).
Patients and Methods
: The present study is a prospective, randomized, controlled, and single-center trial. Patients with an indication for obstructive prostate surgery via AEEP were prospectively included in the study. To assess ME, the time in minutes required for morcellation was recorded and divided by the weight in grams of morcellated prostatic tissue obtained from the pathology report. A comparative analysis of ME was also performed between cases with >60 g and <60 g of morcellated tissue.
Results:
A total of 137 patients were included, 68 in the Multicut group and 69 in the Piranha group. The average ME was higher in the Piranha group, with 9.33 g/minute compared with 7.34 g/minute in the Multicut group (p = 0.012). When analyzing cases with ≤60 g of morcellated tissue, the MEs were 7.32 g/minute for Multicut and 11.31 g/minute for Piranha (p = 0.004). For cases with >60 g of tissue, the efficiencies were 7.4 g/minute and 8.0 g/minute (p = 0.220), respectively. The incidence of beach balls was slightly higher in the Multicut group than in the Piranha group, 14.7% vs 7.2% (p = 0.261). We observed a 4.4% and 0% incidence of bladder mucosa injury with the Multicut and Piranha, respectively.
Conclusions:
In terms of ME, the Multicut is inferior to the Piranha. This difference appears to be more pronounced in smaller prostates. It seems that the Piranha might experience more malfunctions, whereas the Multicut might be associated with more bladder injuries and might require more auxiliary procedures to complete the retrieval of the prostatic tissue.
Introduction
Lower urinary tract symptoms (LUTS) are highly prevalent in males, being present in around 50% of men who are 50 years or older. 1 Despite their diverse etiology, bladder outlet obstruction caused by benign prostatic hyperplasia (BPH) is one of the most common causes of LUTS. 2 Among the various surgical techniques available for its treatment, anatomical endoscopic enucleation of the prostate (AEEP) is gaining increasing popularity. 3 In this approach, the prostatic adenoma is separated from the prostatic capsule and extracted using a special device called a morcellator. 4 The two morcellators with the most evidence available are the VersaCut© (Boston Scientific, Marlborough, Massachusetts, USA) and the Piranha© (Richard Wolf, Knittlingen, Germany), with the latter often considered the gold standard for morcellation quality. 5 In recent years, several new morcellators with promising features but limited scientific evidence have entered the market. One of this new morcellators is the Multicut© (Jena Surgical, Thuringia, Germany).
Both Piranha and Multicut present oscillating blade movement and a two-pedal system for suction only and suction and morcellation. Their main differences are that whereas the Piranha produces suction via a vacuum generator, the Multicut uses a peristaltic pump. Also the Piranha uses disposable blades with a serrated inner blade and a sharp outer blade, whereas the Multicut uses 10-use reusable blades with a sharp inner blade and a serrated outer blade (Fig. 1).

Piranha and Multicut morcellators.
The main objective of the study was to demonstrate the noninferiority of the morcellation efficiency (ME) of the Multicut morcellator compared with the Piranha morcellator following AEEP.
Patients and Methods
The present study is a prospective, randomized, controlled, and single-center trial. Patients with an indication for obstructive prostate surgery via AEEP were prospectively included in the study. The study was approved by our institution’s ethics committee (Reference: C2023/28).
Male patients aged 50–95 years with indication for AEEP because of LUTS were included. All patients underwent preoperative radiologic evaluation, and only patients between 50 and 250 g of adenoma were selected. Standard assessment was done by prostate-specific antigen (PSA) and MRI (when indicated) to rule out prostate cancer.
Exclusion criteria included the following: simultaneous bladder stone endoscopic treatment during AEEP, concomitant urinary neoplasia, previous diagnosis of prostate cancer, or a history of prostatic urethral implants (i.e., prostatic urethral lift) or any device that could complicate the morcellation process.
Patients were randomly assigned to one of the two morcellation groups: using either the Multicut or Piranha, with a 1:1 ratio. Randomization was performed at the time of procedure scheduling using a computerized list. 6
Sample size was calculated based on the primary outcome of “ME (g/minute).” In this noninferiority clinical trial, a minimum noninferiority limit of 0.7 g/minute was estimated when comparing both devices. Accepting a 5% alpha risk and a 20% beta risk in a one-sided test, a total of 120 patients were needed (60 patients per group). A dropout rate of 10% was anticipated.
Morcellation was always performed by the same experienced surgeon (I.S.) who had experience with both morcellators, at least 20 cases each. Standard practice in our institution is to perform laser hemostasis before enucleation until achieving good visibility; if needed, bipolar hemostasis is applied. Four bags of irrigation fluid are connected through two irrigation systems to ensure an adequately full bladder. The suction power and blade rotation speed settings were initially those recommended by the commercial representatives. Maximum suction power was used in both morcellators. The Multicut was initially set at 1600 rotations per minute (rpm), whereas the Piranha was set at 950 rpm, with rpm increased if the adenoma adhered well and decreased if it frequently detached from the blades, which is standard clinical practice.
To assess ME, the time in minutes required for morcellation was recorded, defined as the time from the first contact of the morcellator with the enucleated prostatic adenoma until the aspiration of the last fragment of prostatic tissue. The weight in grams of morcellated prostatic tissue was recorded according to the pathology report. A comparative analysis of ME was also performed between cases with >60 g and <60 g of morcellated tissue. During the procedure, the need for auxiliary procedures to complete morcellation (adenoma resection with loop, use of trident, use of forceps), device malfunctions, bladder mucosal injury, obstruction by adenoma fragments requiring saline injection through the handpiece to resolve, the number of “drops” (unintentional detachments of the adenoma from the morcellator requiring the procedure to be paused to regrasp the adenoma), and the incidence of “beach balls” (small, tough, and fibrotic prostatic tissue nodules that keep on bouncing off the morcellator) were recorded.
Results
A total of 137 patients were included, 68 in the Multicut group and 69 in the Piranha group, recruited between June 2023 and May 2024. Table 1 shows the baseline characteristics of patients, with no significant differences between the groups regarding age, prostate volume, incidence of acute urinary retention before the procedure, use of anticoagulant or antiplatelet medications, International Prostatic Symptom Score, or PSA level.
Baseline Population Characteristics
AUR = acute urinary retention; BPH = benign prostatic hyperplasia; IPSS = International Prostate Symptom Score; N = number of cases; PSA = prostate-specific antigen; QoL = quality of life; SD = standard deviation.
Table 2 presents the results of the variables evaluated during enucleation and morcellation. Mean morcellation time was 14.4 and 11.1 minutes for Multicut and Piranha, respectively (p = 0.094). The incidence of beach balls was slightly higher in the Multicut group than in the Piranha group, 14.7% vs 7.2% (p = 0.261), respectively. In most cases, the beach balls were morcellated by reducing the morcellation speed, but in some cases, auxiliary procedures were necessary. The Multicut group showed a higher incidence of needing auxiliary procedures during morcellation than the Piranha group, 7.3% vs 1.4% (p = 0.091), respectively.
Surgical and Morcellation Results and Complications
We observed a 4.4% incidence of bladder mucosal injury during morcellation with the Multicut (three cases). In one of these cases, an additional procedure was necessary—placement of an anterograde Double-J catheter because of suspected injury to the intramural ureter, given the inability to place it retrogradely (Clavien–Dindo IIIA). In the remaining cases, no additional procedures or extended bladder catheterization time was required. In the Piranha group, no cases of bladder mucosal injury were observed. No cases of deeper bladder injury (bladder perforation) were observed with either morcellator. All cases were managed with laser coagulation or bipolar coagulation if the bipolar was already used for prostate capsule hemostasis.
Regarding equipment malfunctions, the Multicut experienced fewer malfunctions, with only one event that allowed the procedure to continue after replacing the blades. The Piranha experienced seven malfunctions, mainly related to vacuum generation, three of which required a complete change of equipment to continue the morcellation. Despite this, no patients needed to postpone morcellation or to perform it in two stages.
Table 3 shows the ME for both groups. The average ME was higher in the Piranha group, with 9.33 g/minute compared with 7.34 g/minute in the Multicut group (p = 0.012). When analyzing cases with ≤60 g of morcellated tissue, the MEs were 7.32 g/minute for Multicut and 11.31 g/minute for Piranha (p = 0.004). For cases with >60 g of tissue, the efficiencies were 7.4 g/minute and 8.0 g/minute (p = 0.220), respectively (Fig. 2). Another subgroup analysis was the comparison inside each morcellator’s group of ME between patients with and without a history of treatment with 5ARI (5-alpha reductase inhibitor) for BPH before AEEP. In the Multicut group, ME with 5ARI was 9.2 g/minute (standard deviation [SD]: 4.6) and ME without 5ARI was 6.4 g/minute (SD: 3.9), with p = 0.008. In the Piranha group, ME with 5ARI was 9.1 g/minute (SD: 5.0) and ME without 5ARI was 9.5 g/minute (SD: 4.7), without statistical significance (p = 0.357).
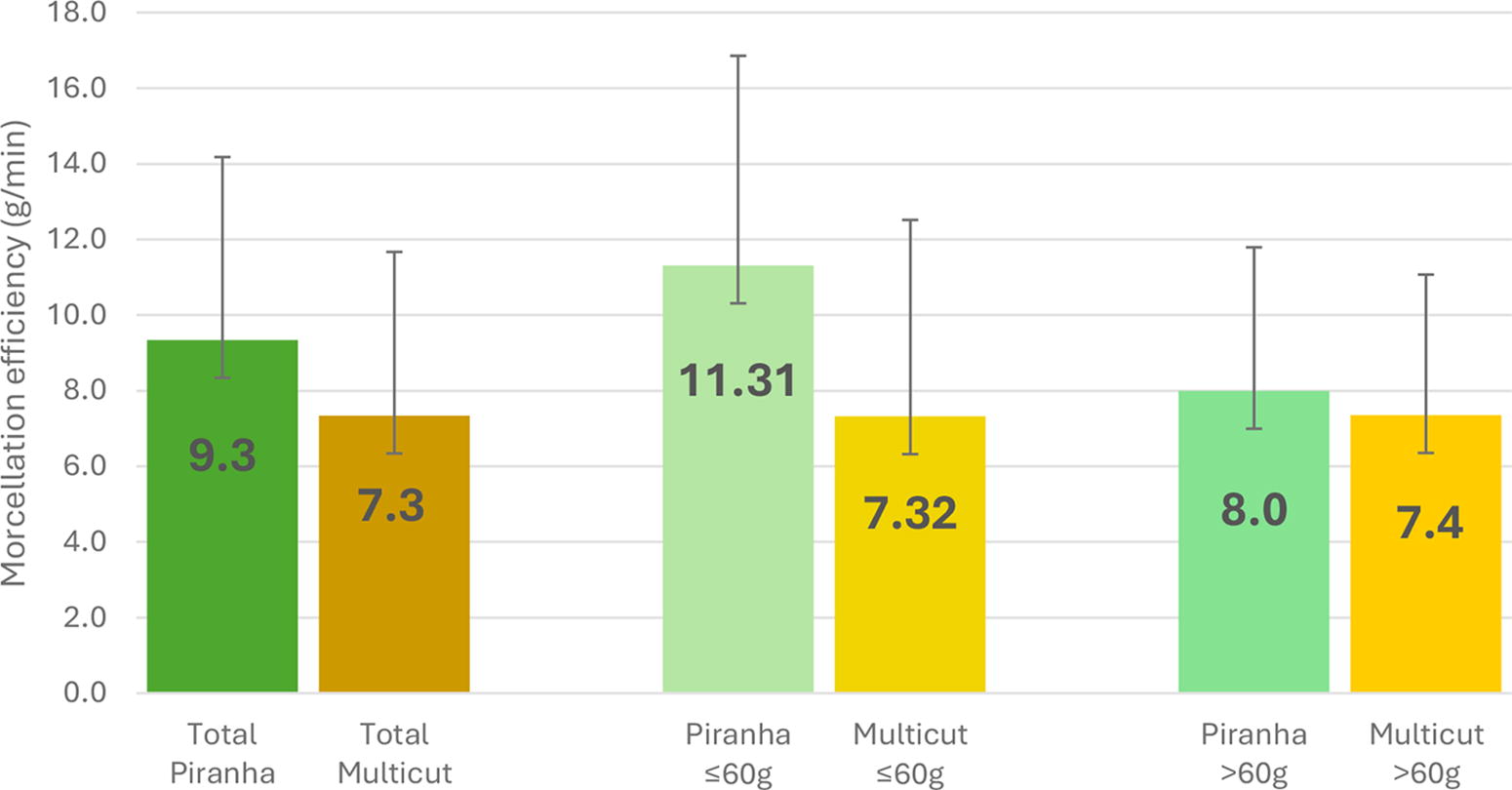
Morcellation efficiency comparison. Overall efficiency for each morcellator and comparison between bigger (> 60 g of morcellated tissue) and smaller (≤ 60 g) adenomas. g = grams; min = minutes.
Morcellation Efficiency, Total and Subgroup Analysis
ME = morcellation efficiency.
Discussion
As AEEP becomes a new gold standard treatment for BPH, technical and technological advancements continue to emerge. Just as different types of lasers and pulse modulations have been developed in recent years, new morcellators have also entered the market in an effort to facilitate this often underappreciated aspect of AEEP. 7 Morcellation can range from a monotonous and relatively simple procedure when everything goes smoothly, to a frustrating one when proper morcellation of the fragments cannot be achieved, and even to a highly stressful process if bladder or prostatic capsule injury occurs. 8 For these reasons, the potential for greater efficiency and safety with new morcellators has generated significant interest.
There is a lack of robust evidence regarding the performance of most of these new morcellators. To the best of our knowledge, this is the first clinical study to evaluate the efficiency and safety of the Multicut morcellator.
We have observed ME of 7.34 g/minute for the Multicut and 9.33 g/minute for the Piranha. Some studies report even higher efficiency for Piranha. 9,10 Despite the lack of studies analyzing the ME for Multicut, we consider the one observed in our study to be high, as it exceeds the average enucleation efficiency reported in a recent systematic review, which found 5.29 g/minute for the Piranha, 3.9 g/minute for the VersaCut, and 5.3 g/minute for the Drill Cut© (Storz Medical AG, Tägerwilen, Switzerland).
When analyzing ME in cases with ≤60 g or >60 g of morcellated tissue, we observed that the difference between the two morcellators is more pronounced in smaller prostates and less so in larger prostates. This difference could be partially attributed to the need to pause morcellation to empty the Piranha’s water reservoir. We used a 2-L reservoir, but there are 5-L reservoirs available that could potentially improve efficiency. Interestingly, the Multicut maintains stable efficiency with larger prostates. Zell et al. also observed a loss of efficiency with increasing prostate volume in both the Piranha and VersaCut. 5
Another interesting subgroup analysis was the comparison of ME between patients with and without previous treatment with 5ARI for BPH. In the Multicut group, there was a statistically significant and clinically relevant difference showing higher efficiency (44% higher) in patients with prior treatment with 5ARI. This effect was not observed in the Piranha group. It is important to point out that this study was not designed to analyze these subgroups, and so, the results should be interpreted with caution.
El Tayeb et al. suggested that the Piranha, being a more complex device than the VersaCut, was more challenging for both the surgeon and the operating room staff to use. 11 The Multicut has a suction mechanism more akin to the VersaCut, a peristaltic pump without reservoir. This could make it simpler to operate, offering a slight advantage during the initial cases performed by a surgical team. The same argument regarding the simpler suction mechanism could also explain the lower incidence of equipment malfunctions observed with the Multicut compared with the Piranha. Of the three previous studies comparing the VersaCut and Piranha, two reported a higher incidence of malfunctions with the Piranha, whereas the other did not observe any differences. 8,11,12
Beach balls make morcellation more difficult. 13 Their incidence, as well as the need for auxiliary procedures, was lower in the Piranha group (without achieving statistical significance). If the incidence of beach balls depended solely on the tissue characteristics of the adenoma (e.g., greater fibrosis), this finding could justify the higher incidence of auxiliary procedures. However, the randomized nature of the study suggests that the performance of the morcellator also influences the occurrence of beach balls and the ability to resolve them without auxiliary procedures. In our study, the Multicut was able to morcellate 50% of the beach balls without requiring auxiliary procedures, whereas the Piranha achieved this in 80% of cases. It is difficult though to explain exactly the source of this higher capability for dealing with beach balls. It might be to better suction, a better cutting ability from the design of the Piranha blades, or the fact that these were disposable. An extremely subjective answer in our experience is that it is probably caused by the suction mechanism or blade design. Changing used blades for new ones while using the Multicut usually does not change much how a beach ball is morcellated. Inefficiency when dealing with beach balls might also increase the risk of bladder mucosal injury.
Although extremely low in both groups, the incidence of bladder mucosal injury was higher in the Multicut group. Even though in our study there were no cases in the Piranha group, the average reported in the systematic review by Franz et al. was 1.24%. 5 However, individual studies report bladder injury incidences as high as 7.7% with the Piranha. 10 The number of drops was significantly higher for the Multicut group; this probably shows that the suction mechanism in the Piranha is more efficient. When the prostatic tissue dislodges from the morcellator’s blades, more irrigation fluid is sucked, risking emptying the bladder. This might be, at least in part, why we observed more bladder wall injuries in the Multicut group.
Handpiece obstruction is significantly higher in the Multicut group. Considering that both morcellators have a similar size blade diameter, this might be caused by having a Multicut bigger opening and thus morcellating bigger fragments, as seen in Figure 1.
Of course, there are limitations to this study. The Piranha blades are single-use, whereas the Multicut blades can be reused up to 10 times. Using disposable blades could potentially be more efficient, especially at high revolutions per minute. 14 However, these were the only blades commercially available in our region. Another limitation could be that the Multicut was a completely new device, whereas the Piranha had been in use for approximately 8 years. However, a few weeks before the start of recruitment, the Piranha underwent a complete overhaul by its manufacturer, who deemed it to be in optimal working condition.
Conclusions
Our study found that, in terms of ME, the Multicut is inferior to the Piranha. This difference appears to be more pronounced in smaller prostates. It seems that the Piranha might experience more malfunctions, whereas the Multicut might be associated with more bladder injuries and might require more auxiliary procedures.
Footnotes
Acknowledgment
The authors acknowledge the contribution of Doctor Silvia Mateu, coordinator of investigation and innovation at Fundació Puigvert.
Authors’ Contributions
I.S.: Conceptualization (lead), data curation (equal), investigation (equal), writing—original draft (lead), and formal analysis (lead). P.H.-P.: Conceptualization (equal), data curation (equal), investigation (equal), and writing—review and editing (lead). A.F.A.: Conceptualization (equal), data curation (equal), and methodology (equal). P.I.G.: Formal analysis (equal), investigation (equal), and methodology (lead). L.M.G.: Conceptualization (equal), data curation (equal), visualization (lead), and investigation (equal). M.M.: Data curation (equal). E.M.C.: Data curation (equal) and verification—validation (lead). P.D.: Data curation (lead) and methodology (equal). A.B.: Conceptualization (equal) and supervision (equal). J.P.: Methodology (equal) and supervision (lead). J.P.d.L.R.: Conceptualization (equal) and supervision (lead).
Author Disclosure Statement
The authors declare that they have no competing interests, personal financial interest, funding, employment interest, or any other type of competing interest.
Funding Information
This work has not received any funding, neither from the institution nor from the industry.