
Abstract
Introduction and Objectives:
Aquablation (Aqua) is a novel technique for treating benign prostatic hyperplasia and lower urinary tract symptoms. This study compares Aqua to simple prostatectomy (SP), analyzing functional urinary outcomes, adverse events (AE), and retreatment rates.
Methods:
A single-institution retrospective chart review was conducted for men undergoing open/robotic SP or Aqua from 2017 to 2023 for prostates >80 mL. Data collected included blood transfusions, AE, retreatment rates, postoperative medication use, and International Prostate Symptom Score (IPSS) with quality-of-life (QOL) indicator. To address differences in baseline characteristics, including prostate size, we applied inverse probability of treatment weighting (IPTW). Statistical analyses were performed using R 4.4.0. Results are presented as IPTW-adjusted comparing SP to Aqua using Fischer’s exact test and analysis of variance reported as beta (B) for continuous variables and odds ratios (OR) for categorical variables with 95% confidence intervals (CI).
Results:
In total, 172 patients were studied: 111 Aqua and 61 SP. Groups were well-matched for body mass index (Aqua 28.77 vs SP 28). Aqua patients were older (73.04 vs 68.89), had smaller prostates (135.46 vs 186.53 mL), and lower preoperative urinary retention (21.8% vs 47.5%). Baseline characteristics between groups were adjusted using IPTW. SP outperformed Aqua in 1-year IPSS scores (B = –3.4, CI: −5.7, −1.1, p = 0.005), whereas QOL was comparable (B = –0.46, CI: –1.3, 0.33, p = 0.2). SP patients continued alpha-blockers less often postoperatively (B = −0.27, CI: –0.39, −0.41, p = 0.001). SP showed higher blood transfusion rates (OR = 4.22, CI: 1.64, 13.2, p = 0.006), longer hospital stays (B = 1.7, CI: 1.0, 2.4, p < 0.001), and longer operating times (B = 119, CI: 101, 135, p < 0.001). SP had lower retreatment rates (OR = 0.46, CI: 0.23, 0.87, p = 0.019). AE were not significantly different (p = 0.8).
Conclusions:
Aqua outperformed SP for blood transfusions, hospital stay, and operative time. SP outperformed Aqua for retreatment rates, IPSS scores at 1-year follow-up, and reliance on alpha-blockers.
Introduction
Benign prostatic hyperplasia (BPH) is the most common benign urological disease in men. 1 Moderate-to-severe lower urinary tract symptoms (LUTS) from BPH affect 30% of men over 50 2 and medical treatment often fails for men with moderate-to-severe symptoms, leading them to seek surgical options. 3 The 2023 American Urological Association (AUA) guidelines recognized the emergence of minimally invasive alternatives, including Aquablation (Aqua), for patients with LUTS/BPH and prostate volume (PV) 30–80 g.23 Transurethral resection of the prostate (TURP) remains the gold standard for prostates less than 80 g; simple prostatectomy (SP) remains the standard for larger prostates. Aqua is a novel BPH procedure that may be used for both small and large prostates from 50 to 150 mL. 4 Although TURP has been compared with Aqua extensively, there is a gap in the literature regarding the direct comparison of Aqua to SP. SP, while a well-established operation, is an invasive procedure associated with a relatively high complication rate. 5,6 Aqua potentially offers an endoscopic solution for men with large prostates.
Holmium laser enucleation of the prostate (HoLEP) is a contemporary alternative to SP. 7,8 Although HoLEP may have an improved safety profile compared with SP, it is time-consuming, technically challenging, and complex to learn and implement. 5,6 Aqua, in contrast, has the shortest prostate tissue resection time compared with other minimally invasive approaches and a relatively short learning curve. 9 Aqua provides improved urinary outcomes, better preservation of sexual function, shorter operative times, and lower complication rates compared with TURP. 10 –12 Furthermore, the semi-automation of Aqua allows for better reproducibility among surgeons, reducing intra- and interprocedure variability, and increasing overall treatment efficacy. 13
Aqua was first described in 2015, and several studies have compared Aqua to TURP, Aqua for larger prostate size to Aqua for smaller prostate size, and Aqua to other novel minimally invasive BPH surgeries. 14,15 Despite the absence of comparative studies between Aqua and SP, Aqua appears to have lower transfusion rates (3.9% vs 4.1%–16.1%), 6,19 and shorter operating times (40–55 minutes vs 123–198 minutes) 6,19 than SP. The reported reoperation rates for both appear to be similar (3.0%–4.3% vs 2.1%–4.3%). 16,17 Further, 0.9%–5.9% of patients who have undergone Aqua will require further medical therapy; rates of resuming medical therapy after SP have not been reported. 16 Although previous studies have demonstrated Aqua’s feasibility, safety, and efficacy in larger PVs, a direct comparison of these two surgical methods has not been performed.
Methods
Patient population
This retrospective study was approved by the institutional ethics committee (IRB # 2022-208). Men with moderate-to-severe LUTS because of BPH with prostates >80 mL who underwent either open/robotic SP or Aqua between January 2017 and October 2023 were included. The Aqua procedure was performed on the Procept Biorobotics AquaBeam System.
Outcome measures
Variables were collected retrospectively and included preoperative demographics (age, ASA scores, body mass index [BMI], PV, urinary retention); operative outcomes (Operating) time, length of stay [LOS], blood transfusions); and postoperative outcomes (adverse events [AE], medication [Med] discontinuation, retreatment rates, follow-up time, IPSS with quality of life [QOL], and maximum urinary flow rate [Qmax]). Qmax was removed from the analysis given only one SP patient had postoperative Qmax recorded. Retreatment was defined as any return to the operating room for bladder outlet obstruction more than seven days postop.
Statistical analysis
To address the differences in baseline PV between the Aqua and SP groups, we performed inverse probability of treatment weighting (IPTW). IPTW is a statistical method in which a pseudo-population is created to make the treatment groups comparable based on their baseline characteristics. Propensity scores were calculated using race, ethnicity, BMI, age, preoperative hemoglobin (Hgb), preoperative urinary retention, ASA score, and PV. This allows us to assess the causal effect of the different surgeries more accurately.
Significance was set at p ≤ 0.05. Statistical analyses were performed using R 4.4.0. Results are presented as IPTW-adjusted comparing SP to Aqua using Fischer’s exact test and analysis of variance reported as beta (B) for continuous variables and odds ratios (OR) for categorical variables with 95% confidence intervals (CI).
Results
Baseline characteristics
172 men were included in the study, of which 111 underwent Aqua and 61 underwent SP (Table 1). Among the SP cases, 61% (n = 3) were performed robotically, whereas 39% (n = 24) were performed using an open approach. Groups were well-matched for BMI (Aqua 28.77 vs SP 28.81) and ASA scores (2.56 vs 2.61), but Aqua patients were on average older (73.04 vs 68.89) and had smaller prostates (135.46 vs 186.53 mL). More Caucasians underwent Aqua (79.3% vs 62.3%), whereas SP was performed more frequently on African American men (31.1% vs 11.7%). On average, the Aqua group had a lower preoperative urinary retention incidence (21.8% vs 47.5%) (Table 1).
Preoperative Patient Demographics for Aquablation vs Simple Prostatectomy
Bold p-values are statistically significant based on α = 0.05. Numbers represent mean values with standard deviation in parenthesis unless indicated otherwise.
BMI = body mass index; preop = preoperation.
Perioperative outcomes
Raw data for outcomes are summarized in Table 2, and results from IPTW-adjusted statistical analyses are presented in Tables 3 (categorical data) and 4 (continuous data). Retreatment rate was lower in the SP group, with an adjusted odds ratio (OR) of 0.46 (CI: 0.23–0.87, p = 0.019), whereas the odds for a blood transfusion were significantly higher in the SP group (OR = 4.22, CI: 1.64–13.2, p = 0.006) (Table 3). Postoperative Hgb drop remained significantly higher in the SP group, with an adjusted mean difference of 0.93 g/dL (CI: 1.5–0.36, p = 0.002) (Table 4). In addition, SP was associated with longer hospital stays by 1.7 days (CI: 1.0–2.4, p < 0.001) and longer operating times by 119 minutes (CI: 101–135, p < 0.001) (Table 4).
Outcomes of Aquablation vs Simple Prostatectomy
Numbers represent mean values with standard deviation in parenthesis unless indicated otherwise.
Med = medication; postop = postoperation.
Categorical Outcomes of Aquablation vs Simple Prostatectomy, Adjusted Using IPTW
Bold p-values are statistically significant based on α = 0.05. OR > 1 indicates greater risk for SP, OR < 1 indicates greater risk for Aqua.
CI = confidence interval; IPTW = inverse probability of treatment weighting; OR = odds ratio.
Outcomes of Continuous Variables for Aquablation vs Simple Prostatectomy Using IPTW
Beta values indicate the unit increase (positive) or decrease (negative) for simple prostatectomy group in comparison to aquablation group.
Ari = 5-alpha-reductase inhibitor; IPSS = International Prostate Symptom Score.
No statistically significant difference was seen in AE and average Clavien–Dindo scores between the two treatment groups (Fig. 1, Table 3). However, SP had a higher incidence of grade 2 and 3 AE than Aqua (Table 5). After Aqua, noted complications were the inability to insert the Aqua device needing to convert to TURP (2 patients), bladder injury with perforation (1), bladder injury without perforation (3), and rectal perforation (1). For simple prostatectomy, there was one episode of refractory bleeding necessitating operative repair and one conversion from robotic to open prostatectomy.
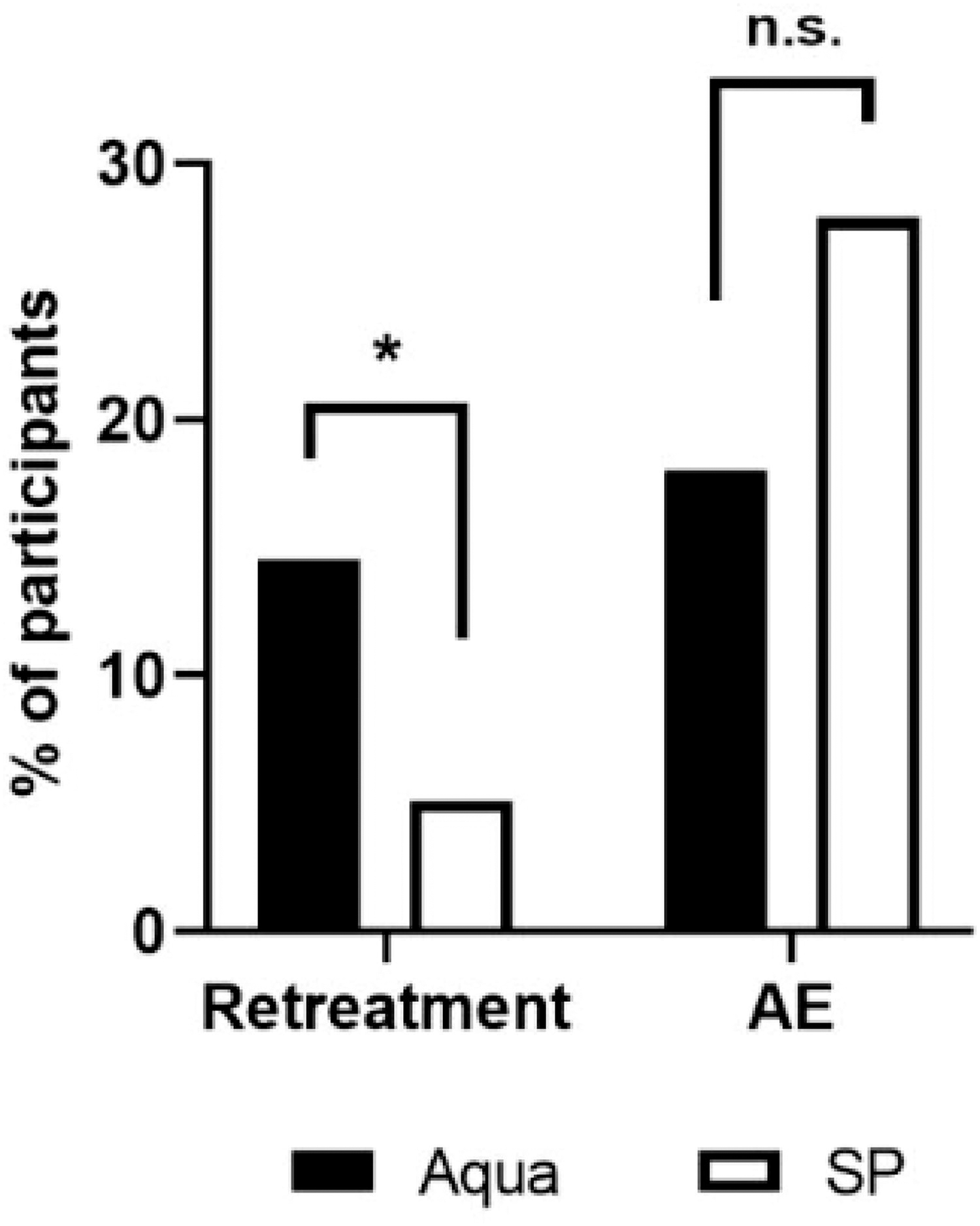
Trends in higher operative retreatment rates and lower adverse events seen in Aquablation compared with simple prostatectomy. The percentage of participants necessitating reoperation or experiencing an adverse event after Aqua or SP was reported. *p < 0.05. Aqua = Aquablation; n.s. = not significant; SP = simple prostatectomy.
Clavien–Dindo Grades Comparing Aquablation and Simple Prostatectomy
Linear by linear association test; bold p-values are statistically significant based on α = 0.05.
Postoperative outcomes
Long-term functional and QOL urinary outcomes improved significantly for both treatments (Fig. 2). However, SP patients had greater improvements in IPSS scores in 12 months with a mean score difference of −3.4 (CI: −5.7 to −1.1, p = 0.005) (Table 4). There were no significant differences in postoperative QOL measures. SP patients relied on alpha-blockers postop less than Aqua patients (B = −0.27, CI: –0.39 to –0.14, p < 0.001) (Fig. 3, Table 4). SP had lower surgical retreatment rates (OR = 0.46, CI: 0.23, 0.87, p = 0.019) (Table 2), most commonly necessitating TURP for prostatic lobe fusion or residual tissue. Four SP patients faced reoperations for bladder neck contracture (Table 6). Median follow-up was longer for SP compared with Aqua by 401 days (CI: 237–565, p < 0.001) (Table 4).

Urinary function subjective and objective improvements after Aquablation and simple prostatectomy.
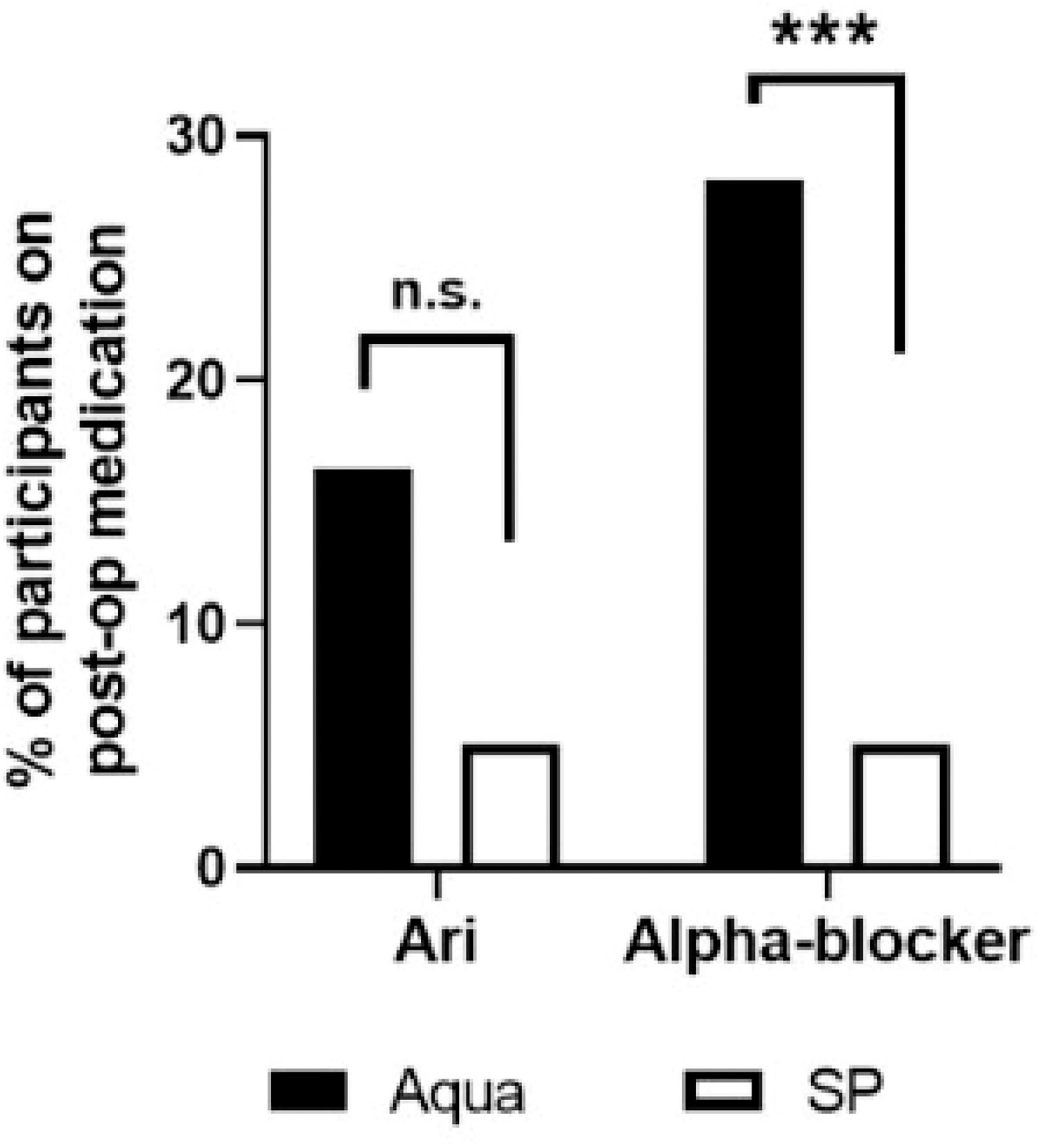
Aquablation has higher postoperative 5-alpha reductase inhibitor (Ari) and alpha-blocker use compared with simple prostatectomy. Percent of men that were using Ari or alpha-blockers after Aqua and SP. ***p < 0.001.
Comparing Etiologies of Need for Reoperation Between Aquablation and Simple Prostatectomy
Bold p-values are statistically significant based on α = 0.05. Numbers represent mean values with standard deviation in parenthesis unless indicated otherwise.
Discussion
This study, using retrospective community data, suggests that Aqua is safe and effective in treating larger prostates, although with higher retreatment rates and IPSS scores at 1 year postoperatively when compared with SP.
Our institution recorded a lower surgical retreatment rate for SP compared with Aqua (OR = 0.46, CI: 0.23, 0.87, p = 0.019) (Table 2). The 14.5% retreatment rate after Aqua in this study is much higher than previously reported in the literature (3.0%–4.3%). 18 SP patients relied on alpha-blockers postoperation (postop) less than Aqua patients (B = −0.27, CI: –0.39 to –0.14, p < 0.001) (Fig. 3, Table 4). Reliance on alpha-blockers after Aqua of 28.2% was greater than what is reported in the literature (0.9%–5.9%). 16
The retreatment rates and reliance on alpha-blockers postoperatively after Aqua in this study were much higher than previously reported. These differences may be partly because of the larger prostates treated in this study and differences in surgical technique and experiences at this institution. Our average PVs for Aqua (135.46 mL) were larger than previous Aqua studies for large prostates. 18 , 19 Helfand et al. studied large PV (107 mL) and very large PV (209 mL) but had no data on retreatment rates, and their follow-up was less than a year. 22 We hypothesize that large prostates, with their increased vasculature and tissue volume, have increased formation of scar tissue after Aqua treatment and electrocautery, which could lead to subsequent fusion of lateral prostatic lobes, obstruction of the prostatic urethral lumen, and necessitate residual tissue removal via TURP.
Aqua demonstrated efficacy in treating large prostates, though long-term functional outcomes were inferior for Aqua compared with SP. However, Aqua outperformed SP in immediate perioperative parameters such as LOS and need for blood transfusion. The higher transfusion rate observed in the SP group likely reflects the inclusion of open SP, which is associated with greater perioperative blood loss compared with robotic SP. This aligns with prior studies showing the increased transfusion requirements of open SP. 24
The inclusion of both open and robotic SP in a single group may contribute to the observed differences in perioperative outcomes, as robotic SP generally has lower transfusion rates, shorter hospital stays, and fewer complications compared with open SP. Although we reported the breakdown of open and robotic cases, subgroup analysis was not feasible because of the limited sample size of open cases.
Although our study demonstrated the overall safety and efficacy of Aqua, two unusual complications were observed in the Aqua group: a rectal injury and an intraperitoneal bladder perforation. The rectal injury is hypothesized to have been caused by the ultrasonography probe, which is locked in place and lacks tactile feedback when moved in and out of the rectum. The bladder perforation may have resulted from overstretching of the bladder because of blocked outflow during the procedure or blind entry into the bladder with the resectoscope after the Aqua scope was removed. The bladder perforation was managed with immediate surgical repair, and the rectal injury was managed with surgical repair after recognition on postop day 3.
The improvement in IPSS and QOL scores seen for Aqua in our study at 12 months postop (7.48 and 1.73, respectively) is similar to the WATER II study at 24 months (5.8 and 1.1, respectively) and other Aqua studies (6.5–7.1 and 4.6–4.8, respectively). 4,11,16,18,19 Although we did not see a statistical difference for QOL scores intertreatment, SP patients had greater improvements in IPSS scores 12 months with a mean score difference of −3.4 (CI: −5.7 to −1.1, p = 0.005) (Table 4). This is likely attributable to the residual prostatic tissue left behind with Aqua that is not seen with SP, which contributes to not only the persistence of obstructive symptoms but the higher reoperation rate.
Unlike IPSS and QOL scores reflecting previous Aqua studies, our postop Med usage was higher than previously reported. Han et al. demonstrated that age >70 years (OR = 2.474; p = 0.001) and any previous LUTS/BPH Med use (OR = 5.384; p = <0.001) were significantly associated with symptom persistency and continuing medical therapy postop. 20 Individual provider preferences may play a role in our study’s higher postop Med usage. In addition, when selecting less ideal patients than found in a clinical trial, community data often show less pronounced outcomes. 21 The high surgical retreatment rate of 14.5% for Aqua and persistent reliance on BPH Meds found in our study emphasizes the need for preoperative patient counseling regarding this risk. Improved knowledge of patient expectations on Med use and retreatment rates after operation can improve procedural satisfaction.
Patients seeking intervention at a later age may elect to have minimally invasive surgery over invasive surgery because of decreased morbidity and mortality. According to Gill et al., the population-based estimate of 1-year mortality after significant surgery among community-living older adults in the United States is 13.4%. 24 Aqua may be safer for these older adults. Our study supports the existing literature, as Aqua is less invasive, leading to significant decreases in transfusions and less precipitous drops in Hgb postop compared with SP. 10,12,13,16,19
A potential solution for men with very large prostates and multiple comorbidities who are high-risk for major surgery is a staged procedure with either two Aquas or Aqua followed by TURP. Since Aqua does not treat anterior prostate tissue, some centers now perform anterior tissue resection during bleeding control, hypothetically reducing the likelihood of prostatic fusion and retreatment.
This study’s retrospective, single-institution design may limit the generalizability of the findings. The groups had varied significantly in age, prostate size, and history of retention, affecting prognosis and recovery, which is a limitation. We were able to partially alleviate this discrepancy in prostate sizes using IPTW. Sexual function was not measured. Surgeon experience with both procedures was not accounted for; SP is well-established, but some surgeons may be less experienced with Aqua. HoLEP has been demonstrated to have lower transfusion rates and shorter hospitalizations than SP and would thus be a logical comparator to Aqua and SP for this study. 7,8 However, our institution did not have the equipment or personnel to perform HoLEP at the time of this study. Further multicenter studies are needed to generalize findings, control for surgeon experience, and intraoperative variables. Future studies could compare the long-term outcomes of a two-stage Aqua approach to SP or Aqua vs HoLEP.
Aqua therapy was superior to SP with respect to blood transfusions, LOS, and operative times. However, IPSS scores, retreatment rates, time until retreatment, and reliance on BPH Med were worse for Aqua than for SP. Aqua may be a better option for men who are higher surgical risk candidates and may not tolerate a SP; these men should be counseled on the higher likelihood that they will need surgical retreatment.
Conclusion
Aqua is safe and effective in treating larger prostates, although with higher retreatment rates and IPSS scores at one year postoperatively when compared with SP.
Footnotes
Authors’ Contributions
D.G.: Methodology, investigation, formal analysis, writing original draft supervision M.J.: Writing original draft and writing—review and editing. A.K.: Writing—review and editing, formal analysis, and investigation. J.K.: Investigation, writing—original draft. P.H.: Investigation, methodology, and data curation. G.P.: Investigation, data collection, and data curation. B.M.M.Z.: Methodology, formal analysis, visualization, writing—review and editing, and data curation. J.H.: Supervision, writing—review and editing, conceptualization, methodology. K.M.P.: Conceptualization, methodology, supervision, and writing—review and editing.
Author Disclosure Statement
The authors declare that they have no relevant or material financial interests that relate to the research described in this article.
Funding Information
No funding was received for this study.