
Abstract
Retzius-sparing robot-assisted radical prostatectomy (RS-RARP) is a technically challenging procedure, which can confer benefits of early return to urinary continence. This article describes the indications, relative contraindications, preoperative preparation, surgical steps, and postoperative care of patients who undergo RS-RARP. In addition, we highlight several scenarios where RS-RARP can be attempted, such as anterior tumors, large median lobes, previous bladder outlet operation, pelvic lymph node dissection, previous inguinal hernia mesh procedure, salvage operation, and renal transplant recipients.
Background
The first documented series of 200 patients who underwent Retzius-sparing robot-assisted radical prostatectomy (RS-RARP) was published in 2013 by Galfano and colleagues. 1 By preserving all the anterior supports of the bladder, endopelvic fascia, and puboprostatic and pubovesical ligaments, the team from Milan was able to achieve high early continence rates of 92% with low 1-year biochemical recurrence rates. Within the next decade, this technique, although initially technically challenging, has been steadily adopted by numerous robotic urologists all over the world. In 2022, a systematic review and meta-analysis comparing RS-RARP with standard RARP was performed, including four randomized controlled trials and six prospective observational studies. 2 This found that immediate continence and continence at 3 and 6 months were significantly better among those who underwent RS-RARP compared with standard RARP. However, positive surgical margin rates were more common in both ≤pT2 and ≥pT3 patients who underwent RS-RARP compared with standard RARP.
Indications
The indications for RS-RARP are the same as for standard RARP. Any patient newly found to have D’Amico intermediate- or high-risk prostate cancer who is a surgical candidate and has been informed on the risks, benefits, and alternatives to radical treatment options can be eligible for RS-RARP.
Some relative contraindications for RS-RARP include large anterior tumors, large prostate volumes (e.g., >100 cc), or locally advanced tumors.
Preoperative Preparation
As with any RARP, patients should have biopsy-proven prostate cancer and a recent serum total prostate-specific antigen within 3 months of the procedure. In addition, cross-sectional imaging should be obtained for both local and systemic staging. A MRI of the prostate, with or without contrast, is helpful to ascertain the anatomy of the prostate, prostate volume, membranous urethral length, and tumor foci. This can be helpful for surgical planning, help in preoperative counseling, and for the surgeon to decide if certain steps can be safely performed. For example, one might omit nerve sparing if there is a clear capsular bulge on the ipsilateral side with biopsy-proven high-grade cancer present. Particularly when considering a patient for RS-RARP, a preoperative MRI showing a large anterior tumor will be a yellow flag and certainly not one for novices in this approach to attempt RS-RARP.
Patient Positioning
Typically, the patient undergoing RS-RARP will be placed in a steep Trendelenburg position, with legs apart, which can permit easy access for perineal pressure to be applied when checking for hemostasis during or after closure of the dorsal venous complex. In addition, this can allow digital rectal examination to be performed or a rectal catheter to be inserted to perform a leak test, should there be any doubt about rectal injury.
Surgical Steps for RS-RARP
Port placement
Access to the peritoneum is gained using the open Hasson’s technique with a supra-umbilical incision, where the 8 mm camera port will be introduced. We administer a transverse abdominis plane (TAP) block under direct vision in between the transverse abdominis muscle and the fascial layer superficial to it, using 20 mL of 0.375% bupivacaine on each side. The point of introduction is usually the midaxillary line, about 1 fingerbreadths below the tip of the 12th rib. The TAP block is intended to anesthetize the nerves supplying the anterior abdominal wall (T6 to L1) and reduce intra- and postoperative pain. On the left side, two robotic 8 mm ports are placed under vision at the level of the umbilicus (Fig. 1). This will be used for the ProGrasp forceps (lateral) and the Maryland bipolar forceps (medial). On the right side, one robotic 8 mm port is placed lateral to the umbilicus (used for monopolar curved scissors), a 5 mm assistant port is placed superior and between the camera and right robotic port, and finally, a 12 mm assistant port 2 fingerbreadths above the right anterior superior iliac spine. An AirSeal® device (Lawmed, ConMed) is connected to the 12 mm valveless assistant port, which helps maintain a more consistent intra-abdominal pressure during the procedure.

Patient positioning and port placement.
Posterior dissection
To gain access to the pelvis, we first divide any adhesions of the sigmoid colon. We make a peritoneum incision posterior to the bladder (Fig. 2). By staying close to the peritoneum, we continue the dissection and first encounter the vas deferens. We recommend identifying both vas deferens and tracing them down to the midline before dividing the right one (Fig. 3a), as this can prevent any misidentification of the ureter and iatrogenic ureteral injury. We then identify the right seminal vesicles (SV) and mobilize them with blunt dissections medially in the avascular plane between the vesicles and the Denonvilliers’ fascia posteriorly. Another approach is to dissect above the vas, aiming posteriorly and climbing over the seminal vesicle (Fig. 3b). Once this window is created, it can be widened and all that is left is to secure the lateral pedicles to the SV (Fig. 3c). We avoid electrocautery especially near the tip of the vesicles because the cavernosal nerves traverse closely. Dissection is completed after fully mobilizing the vesicles off the Denonvilliers’ fascia posteriorly and the attachments laterally. We then repeat this for the left side and end up with both SV and vas predissected (Fig. 3d).
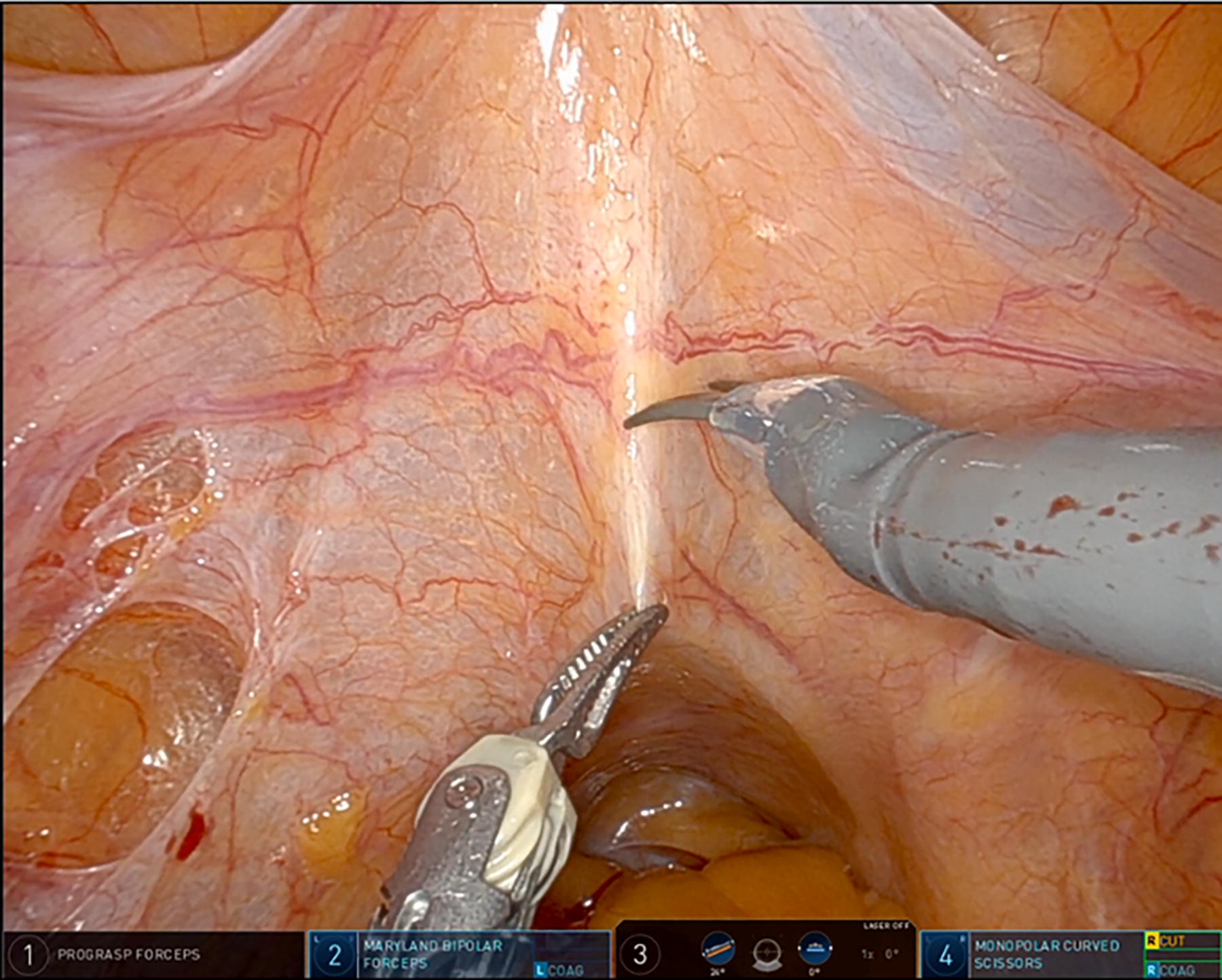
Peritoneal incision.
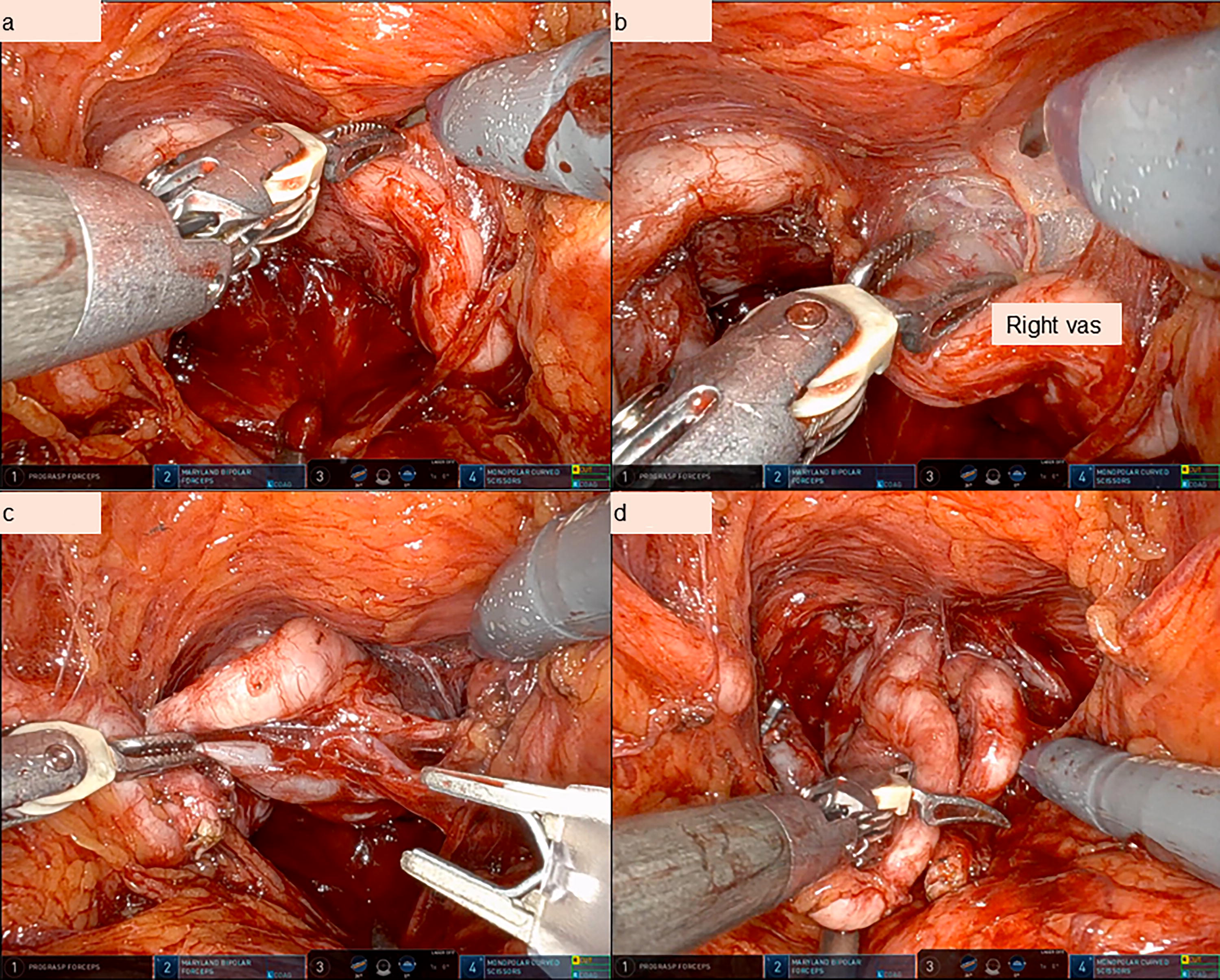
Vas and seminal vesicle dissection.
Subsequently, we continue the posterior dissection further down behind the seminal vesicles. To set up, we hold both seminal vesicles with the ProGrasp forceps and lift up anteriorly (Fig. 4). We sharply cold divide the Denonvilliers’ fascia. Extrafascial dissection proceeds between the Denonvilliers’ fascia anteriorly and the prerectal fat posteriorly. Interfascial dissection proceeds between the prostatic fascia and the Denonvilliers’ fascia, with the assistant retracting the tough Denonvilliers’ fascia posteriorly with the suction device inserted through the 5 mm port, the left hand Maryland retracting the prostate anteriorly. Intrafascial dissection proceeds just under the prostatic fascia (Fig. 5). Dissection is carried on till the apex of the prostate caudally.
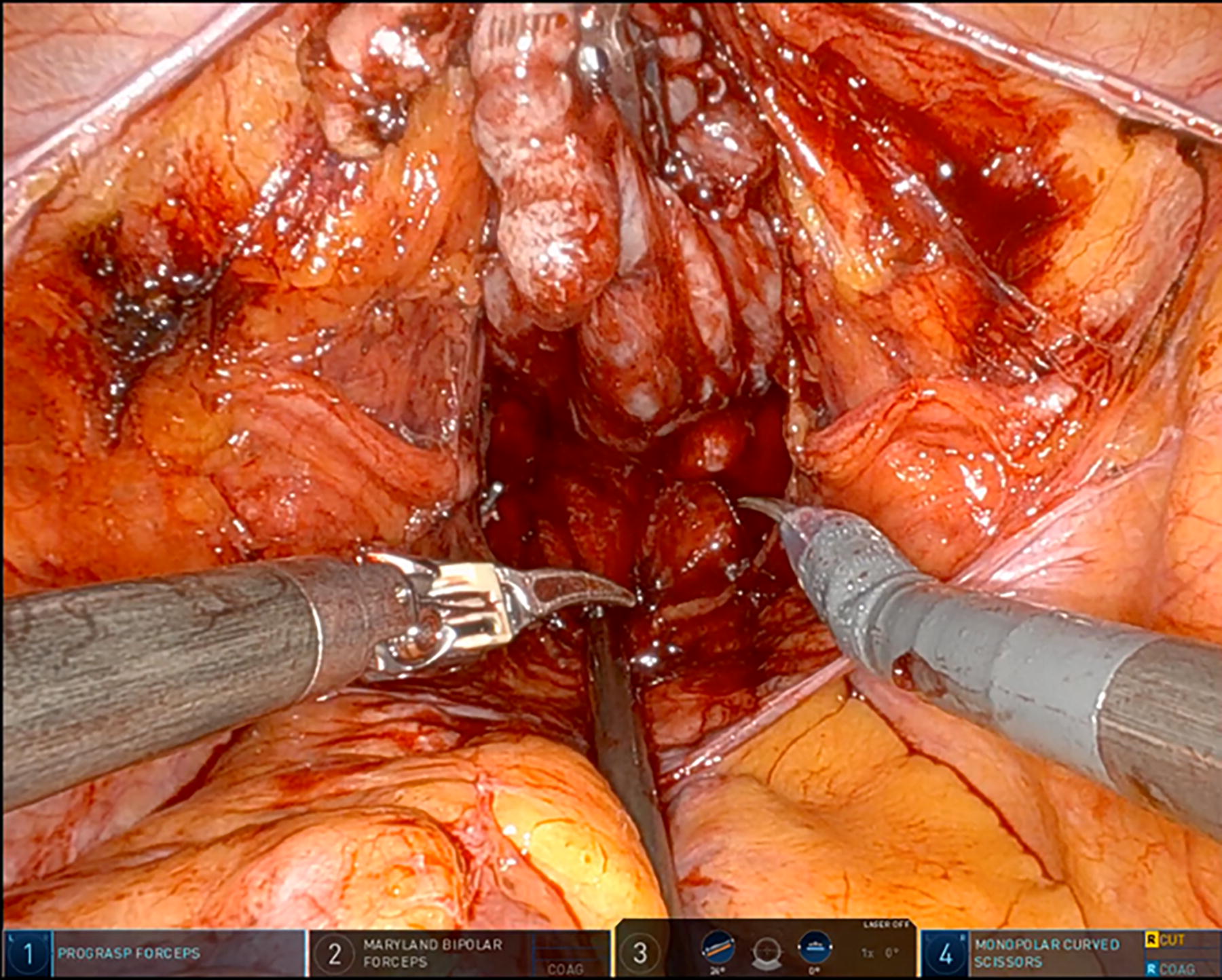
Posterior dissection.
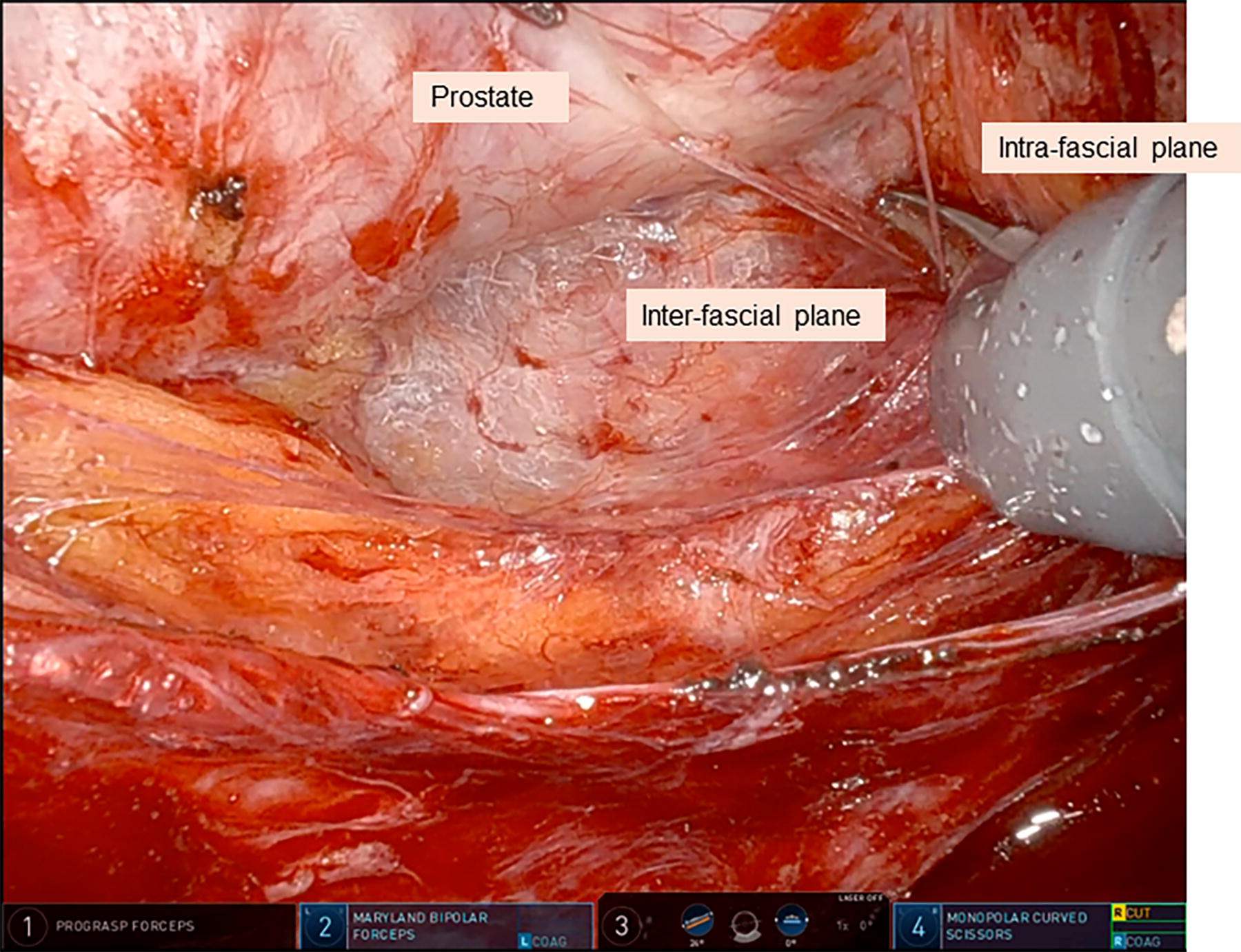
Circumferential pedicle dissection.
Prostatic pedicles and lateral dissection
The prostatic pedicles are dissected and clipped with Hem-o-lok or metallic clips and divided with cold-cut scissors. Spot diathermy is permitted should there be any back bleeding from the pedicles. Lateral dissection is continued in the desired nerve-sparing plane. The bladder is carefully dissected off the prostate gland, from lateral to medial. A high vs low release of the neurovascular bundle (NV) can be performed and this indicates how close the bundle is divided to the prostate. The closer it is divided off the prostate, the “higher” the NV bundle release, and this is thought to confer better nerve preservation and its associated downstream beneficial effects for continence and erectile function. Of course, this is balanced against the preoperative disease characteristics from the prostate biopsy and the MRI.
Bladder neck and anterior dissection
After lateral dissection is completed, we next aim to define the prostatovesical junction through careful dissection. With the Maryland bipolar forceps holding the bladder up anteriorly, the ProGrasp forceps can be used to hold the predissected SVs to provide countertraction (Fig. 6). In this manner, the detrusor slips can be divided with a combination of cautery and blunt dissection, to delineate the urethra (Fig. 7a). A careful bladder neck-sparing dissection may partly contribute to continence recovery postoperatively. The urethra can then be divided with cautery, revealing the urethral catheter, which can be deflated and withdrawn by the bedside assistant. This will then clearly expose the anterior prostate–vesical junction (Fig. 7b), which can then permit subsequent anterior dissection over the anterior prostate surface, and staying under the bladder, until the apex of the prostate.
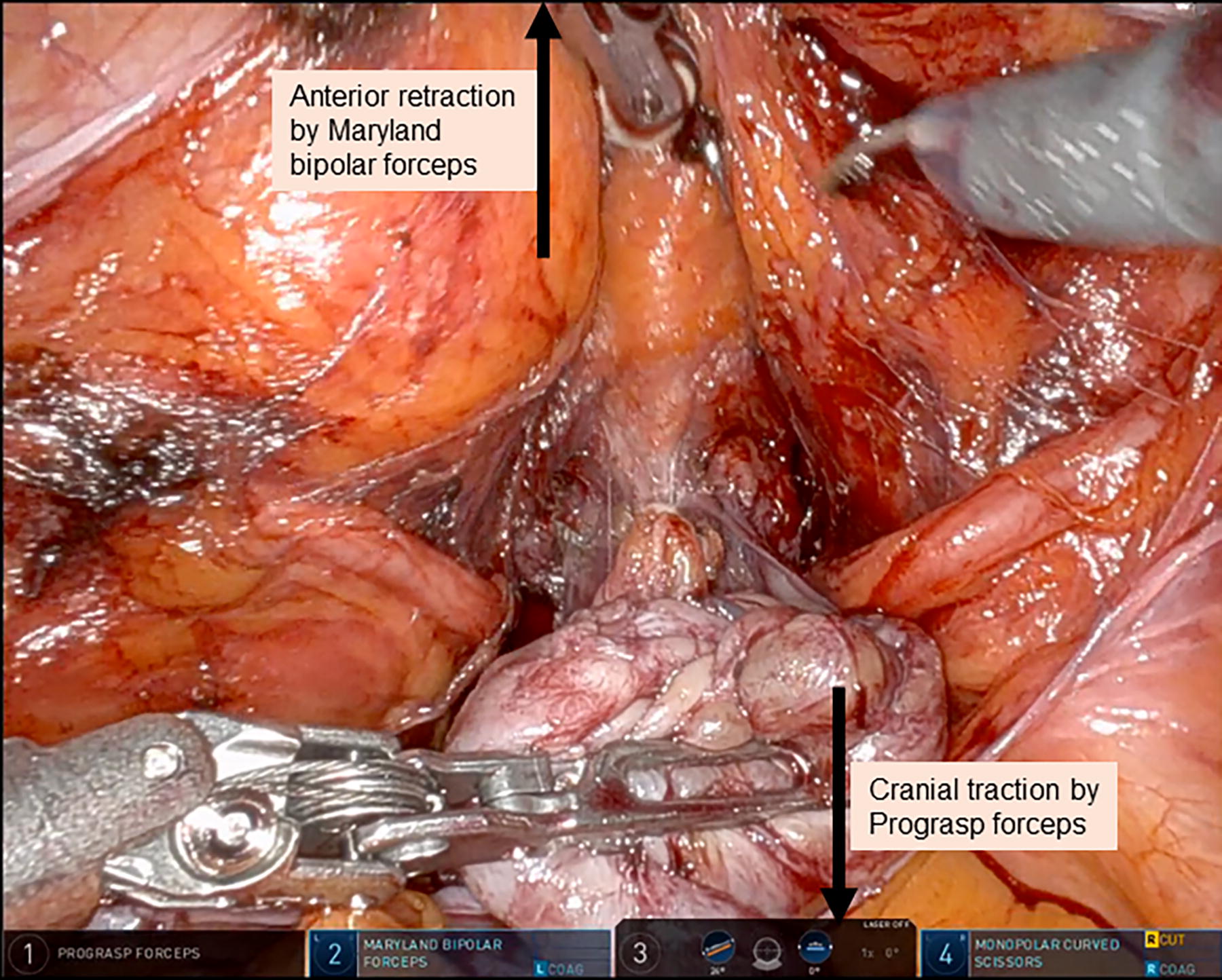
Bladder neck dissection.
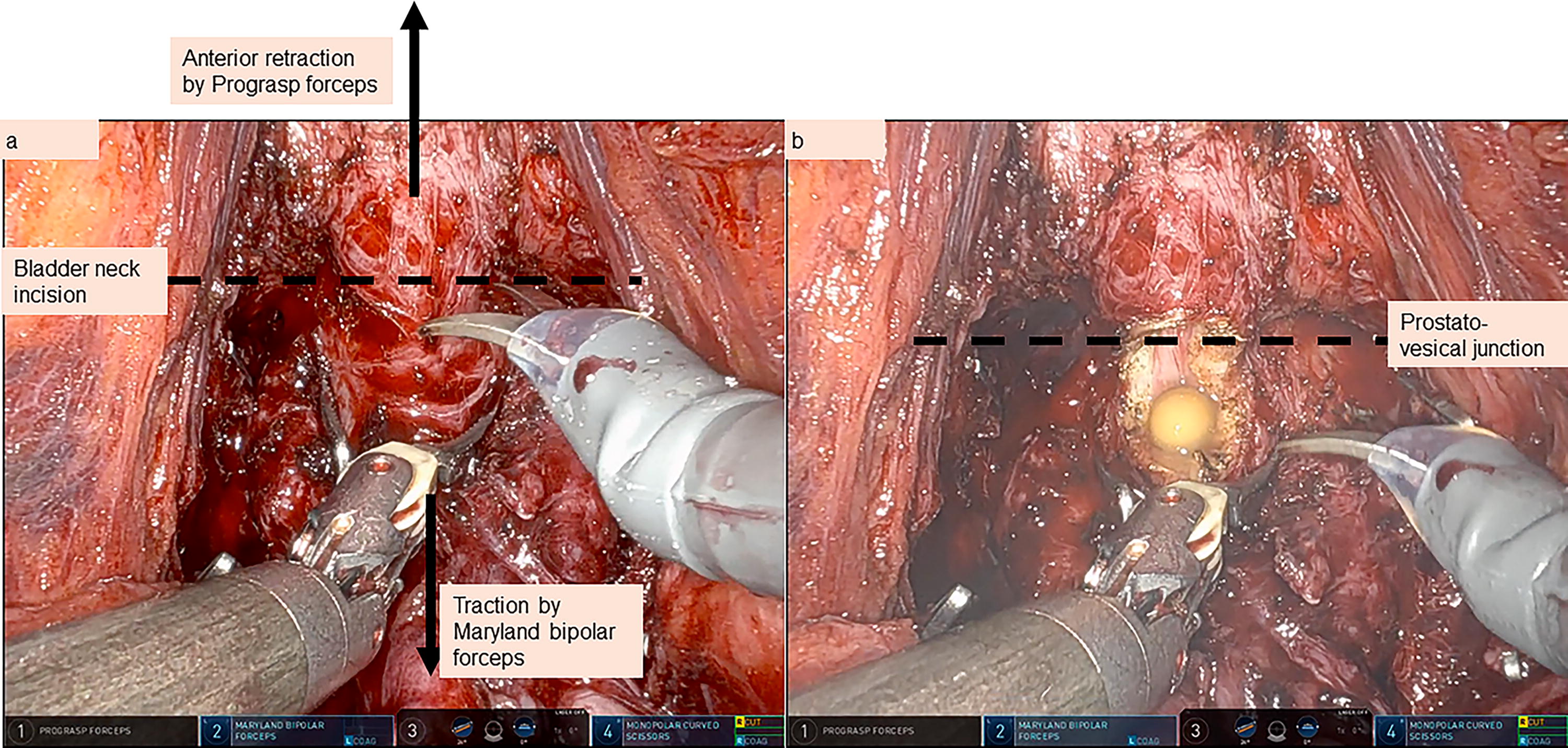
Bladder neck incision.
Apex and urethra
It is important to note the anatomical location of the dorsal vascular complex (DVC), which tends to hug the prostate apex closely. Technically, it is possible to avoid cutting into the DVC, going below the veins as we approach the prostate apex. Given that more than one-third of the striated urethral sphincter’s surface area is located ventrally to the DVC, sparing the DVC during anterior dissection of RS-RARP is thought to reduce the damage to the urethral sphincter. This may therefore translate to earlier continence recovery. 3,4 However, if there is biopsy-proven anterior disease, or a visible PIRADS (Prostate Imaging-Reporting and Data System) ≥3 tumor in the anterior prostate, it would be prudent to divide the DVC to ensure a clear margin. The DVC can then be closed with V-Loc 3/0 barbed sutures to ensure hemostasis.
To ensure a good apical dissection, the prostate should be mobilized side-to-side for lateral dissection and good visualization (Fig. 8a). The urethra is divided cold to avoid any thermal injuries to the sphincter. Once the urethral catheter is exposed, it can be withdrawn by the bedside assistant (Fig. 8b). The remnant posterior attachments are divided to complete the prostatectomy. The specimen, consisting of the prostate gland, bilateral seminal vesicles, and vas, is then placed in an endobag for retrieval.

Anterior dissection and apical dissection.
Hemostasis is ensured with bipolar cautery and/or absorbable sutures, for example, Vicryl 3/0 as required.
Vesicourethral anastomosis
To start, the ProGrasp forceps is holding the bladder up in a fairly relaxed position. The vesicourethral anastomosis (VUA) starts from the 12 o’clock position, outside-in on the bladder side, with the full thickness of the bladder wall incorporated and exiting out from bladder mucosa (Fig. 9a). The sutures we use include the following: (1) V-Loc 3/0 gold sutures with a 17 mm 3/8 needle, (2) V-Loc 3/0 on a 17 mm 1/2 needle, or (3) Filbloc 3/0 on a 5/8 needle. The urethral catheter is moved in and out during the fashioning of the VUA to allow the surgeon to visualize the urethra lumen and to ensure the urethra mucosa has been incorporated by the suture (Fig. 9b). The suture directions can be changed at 3 and 9 o’clock position to inside-out on the bladder, as this can facilitate easier suturing. After the initial sutures are placed, the bladder is relaxed by bringing the ProGrasp forceps caudally so that the sutures can be tightened fully. Once the VUA is completed, a new 16 Fr urethral catheter is inserted and a leak test is performed by filling 300 mL into the bladder. Once no leak is confirmed, we instill 40 mL of 0.5% bupivacaine local anesthesia to the bladder for about 30 minutes, before free drainage is allowed postoperatively.
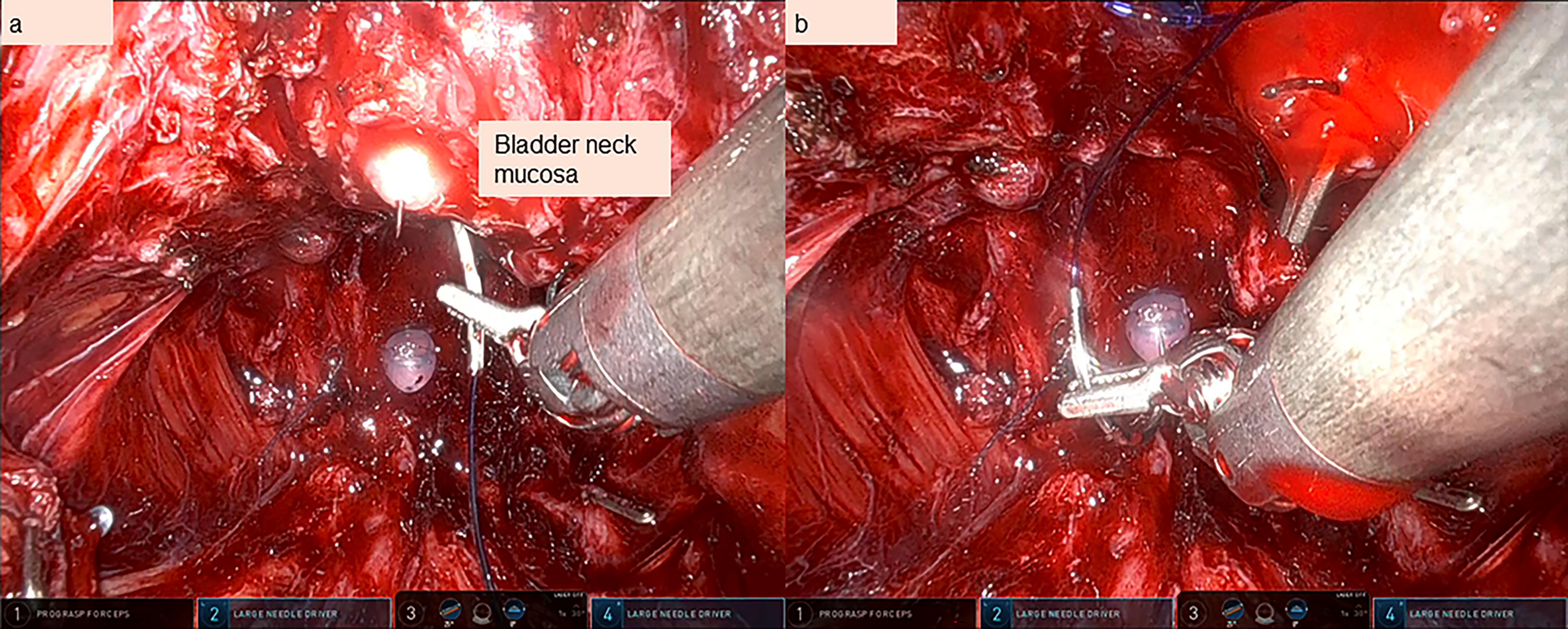
Vesicourethral anastomosis.
Finishing
We check hemostasis at low pressure of 5 mm Hg. Hemostatic agents (e.g., Fibrillar) are placed posteriorly behind the anastomosis (Fig. 10a). The 12 mm port is closed with PDS 2/0 intracorporeally (Fig. 10b). The specimen is extracted. The midline fascia is closed with PDS (Polydioxanone) 1/0, and the rest of the wounds closed with Monocryl 3/0.

Hemostasis, hemostat placement, and port closure.
Additional Considerations
Anterior tumors—how to avoid positive surgical margins
As mentioned, if there is biopsy-proven anterior disease, or a visible PIRADS ≥3 tumor in the anterior prostate, it would be prudent to divide the DVC during the anterior dissection to ensure a clear margin. Although this can cause more bleeding, this can be managed with a temporary increase in pneumoperitoneum to 20 mm Hg. The DVC can then be closed with V-Loc 3/0 barbed sutures to ensure hemostasis.
Large median lobes
Careful bladder neck dissection is required during RS-RARP especially in a patient with known large median lobe. If the bladder neck is substantially bigger than the urethra opening, bladder neck reconstruction is advisable and this can be performed in a tennis-racket manner using Vicryl 3/0 or V-Loc 3/0 sutures.
Previous bladder outlet operation such as TURP
In a patient with previous bladder outlet operation, for example, TURP (Transurethral Resection of the Prostate), a preoperative MRI is mandatory. This will help delineate the anatomy and ascertain (if any) the degree of prostatic regrowth and the width of the prostatic channel. Meticulous bladder neck dissection is required, similar to the scenario of large median lobes.
Pelvic lymph node dissection after RS-RARP
Without dropping the bladder, bilateral extended pelvic lymph node dissection (ePLND) can be performed in the same manner. In fact, because the lateral border of the bladder is held up anteriorly in the original position, ePLND can proceed by incising the peritoneum between the vas deferens and the external iliac artery (Fig. 11a). The external iliac vessels are identified (Fig. 11b). The obturator lymph nodes are then dissected off the lateral surface of the bladder, ensuring identification of the obturator nerve and vessels along the way (Fig. 11c). The anterior and posterior lymph node packets are dissected off using either cautery or Hem-o-lok clips. Finally, after completing the ePLND, we usually place hemostatic agents (e.g., Fibrillar) around the obturator and external iliac vessels (Fig. 11d).

Lymph node dissection.
Previous surgeries (e.g., inguinal hernia mesh)
In patients with previous inguinal hernia mesh repair, with a Retzius-sparing approach, there is no need to dissect anteriorly to drop the bladder and invade the space of Retzius. Therefore, there would not be any concerns of the inguinal mesh or adhesions that may be an issue during a standard anterograde RARP.
Salvage situations (previous radiation or focal therapies)
RS-RARP is possible in salvage situations when undertaken by experienced surgeons.
Renal transplant recipients
For renal transplant recipients who have their transplanted kidney either in the left or right iliac fossa, one can consider a Retzius-sparing approach. This has been found to be feasible and safe, avoiding the need to come close to the transplant kidney. 5,6
Outcomes
The key outcomes of Retzius-sparing prostatectomy, from some large series, are summarized in Table 1.
Table Summarizing the Key Outcomes of Retzius-Sparing Radical Prostatectomy from Large Series
RS-RARP = Retzius-sparing robot-assisted radical prostatectomy; sRARP = standard/conventional radical prostatectomy; PSM = positive surgical margin; NA = not available; RCT = randomized controlled trial; CD3 = Clavien–Dindo grade 3 complications; QoL = quality of life; BCR = biochemical recurrence.
Conclusions
RS-RARP is a technically challenging procedure, which can confer benefits of early return to urinary continence. We have described the indications, relative contraindications, preoperative preparation, surgical steps, and postoperative care of patients who undergo RS-RARP. By highlighting several scenarios where RS-RARP can be performed, such as anterior tumors, large median lobes, previous bladder outlet procedure, pelvic lymph node dissection, previous inguinal hernia mesh operation, salvage procedure, and renal transplant recipients, we showed that RS-RARP is a relatively versatile treatment procedure for our patients with localized prostate cancer.
Footnotes
Authors’ Contributions
S.N.: Conceptualization (lead), visualization, writing—original draft (equal), and writing—review and editing (equal). J.J.L.: Conceptualization (supporting), writing—original draft (equal), and writing—review and editing (equal). P.S.: Conceptualization (supporting), writing—review and editing (equal), and supervision.
Author Disclosure Statement
The authors have no conflicts of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.