
Abstract
Background:
There is an urgent need for a seamless clinical system for tracking implants deployed transiently in patients, to reduce the morbidity related to omission of timely removal. Using a ubiquitous implant of ureteral stents as a pilot project, we developed a novel system (Automated System for Tracking, Recording, and Reminding of Implants [TRACER]) that allows seamless tracking and deployment of reminders to clinicians, without the need for excessive infrastructural overhaul of existing hospital processes.
Patients and Methods:
Briefly, TRACER comprises the following: (1) a two-pronged trigger during implant (stent) insertion to associate implant, patient, and physician details; (2) data field verification by an automated algorithm; (3) automated delivery of reminders to clinicians at a predefined time period if needed; and (4) cessation of reminders upon stent removal. To evaluate the efficacy of TRACER, the records of all stents placed between January 2022 and December 2023 were reviewed and compared between manual stent log entries, electronic operative records, and the TRACER dataset.
Results:
A total of 1056 ureteral stents were placed through 927 procedures in 713 patients. Fifteen stents could have been omitted from tracking owing to an incomplete trigger during stent insertion (logged by one party rather than two) but were detected by the TRACER system during data validation. Sixty-one (5.9%) stents were identified by TRACER as not removed past the predefined time period; 41 patients (3.9%) were contacted and successfully returned for stent removal. Aside from eight patients transferred to other hospitals for care, the demise of seven patients, and five tumor stents not due for change within the study period, all stents were removed on time.
Conclusions:
TRACER is effective, safe, and viable and provides significant savings on manpower. It demonstrates high potential to be scaled and expanded to all implantable devices.
Introduction
Medical implants are routinely deployed in a wide variety of clinical indications, and some implants require timely removal to avoid complications related to prolonged retention. A ubiquitous example includes ureteral stents deployed for a wide variety of scenarios. 1 However, there is a tangible risk of a retained (forgotten indwelling) ureteral stent, which can lead to morbidities of severe urinary tract infection, encrustation leading to complicated removal, and ureteral obstruction with consequent renal parenchymal loss. 2,3 As high as 12% of ureteral stents can be retained, 4 arising from noncompliance to follow-up, and compounded by the lack of an effective system to remind clinicians in the event of a forgotten stent.
The existing stent tracking systems in clinical use rely on manual processes for logging 5 and reminders of overdue stents, and almost all described systems rely on a single individual or party to trigger implant/stent tracking, which can intrinsically lead to a higher risk of human errors and omission of tracking. 6 This use of manual processes also places an additional burden on manpower, which may already be strained in public health care systems with high patient volumes, and can be associated with incremental costs to the institution, which may hinder widespread adoption. To account for this, a variety of stent tracking systems have been described, including the use of ureteral stent cards, 7 integration with institutional electronic medical records (EMR), 8 tracking of billing codes linked to stent insertion or removal, 9 or development of a patient-centric mobile phone application. 10 Although these systems have an advantage over completely paper-based records, they are still limited by a need for largely manual processes of data entry, verification, and reminders.
To overcome the heavy reliance on manual stent monitoring, we designed a novel system for the Automated System for Tracking, Recording, and Reminding of Implants (TRACER) of medical implants, based on barcode tracking, storage of implant information on an EMR database, and automated email reminders that are sent to clinicians when stents are overdue. We report our experience, validating its use as an effective tool to ensure that ureteral stents are removed on time.
Patients and Methods
Development of the TRACER system
The ideal system for implant tracking would comprise the following processes: A trigger for tracking upon implant insertion, with a cross-checking mechanism to ensure no omissions. Association and verification of critical clinical details to permit downstream activation of triggers for tracking, tracing, and reminders. Reminders to correct clinicians at a defined time period, if implant/stent removal has not been performed. Cessation of reminders once removal of implant/stent is completed. Automation of all steps to reduce manpower reliance, while allowing manual verification of individual patient entries when necessary, for audit or verification. Minimal modifications to existing clinical workflows to maximize compliance and sustainability of the system. Minimal costs to the institution for implementation and need for an infrastructural upgrade.
We designed a novel system for TRACER medical implants, with internal processes that fulfill most of the aforementioned criteria. Its processes are summarized in Figure 1. Currently, TRACER is partially automated as it requires manual inputs to trigger implant tracking and for cessation of reminders upon implant removal.

Summary of TRACER ureteral stent tracking system. Step 1, separate data entry by nurses and surgical team. Step 2, data consolidation by the eHINTs system. Step 3, data cross-checking. Step 4, upload of stent information onto the online database. Step 5, automated email reminders to surgeons to ensure stent removal within a predefined time period. Step 6, deactivation of email reminders if stents are removed. eHINTS, electronic health intelligence system; EMR, electronic medical records; REDCap, Research Electronic Data Capture platform; TRACER, Automated System for Tracking, Recording, and Reminding of Implants.
To trigger implant tracking, TRACER first receives data inputs from two independent sources as a cross-checking mechanism to minimize potential risks of omission inherent to a single-party trigger process. This two-pronged trigger requires independent inputs from both nursing and surgical teams concomitantly. The nursing team utilizes an existing system for tracking the movement of reusable instruments in the operating theater (T-DOC 2000 Supply Management System, Getinge, Gothenburg, Sweden). This process is part of the routine workflow and records information including patient and physician particulars, implant lot number, date of insertion, and number and laterality of stents inserted (Fig. 2). The surgical team leverages the EMR to enter both operative findings and stent details. The latter is coded in a standard manner and requires manual entry of a short keyword (“StentL” to represent a left ureteral stent) to indicate laterality, number of stents, and intended duration for stent removal. Both parties therefore provide inputs that are used for subsequent cross-checking and verification. Key data logged include the date of implant insertion, patient identifiers, number and laterality of stent(s), clinician-in-charge, and date for implant (stent) removal.
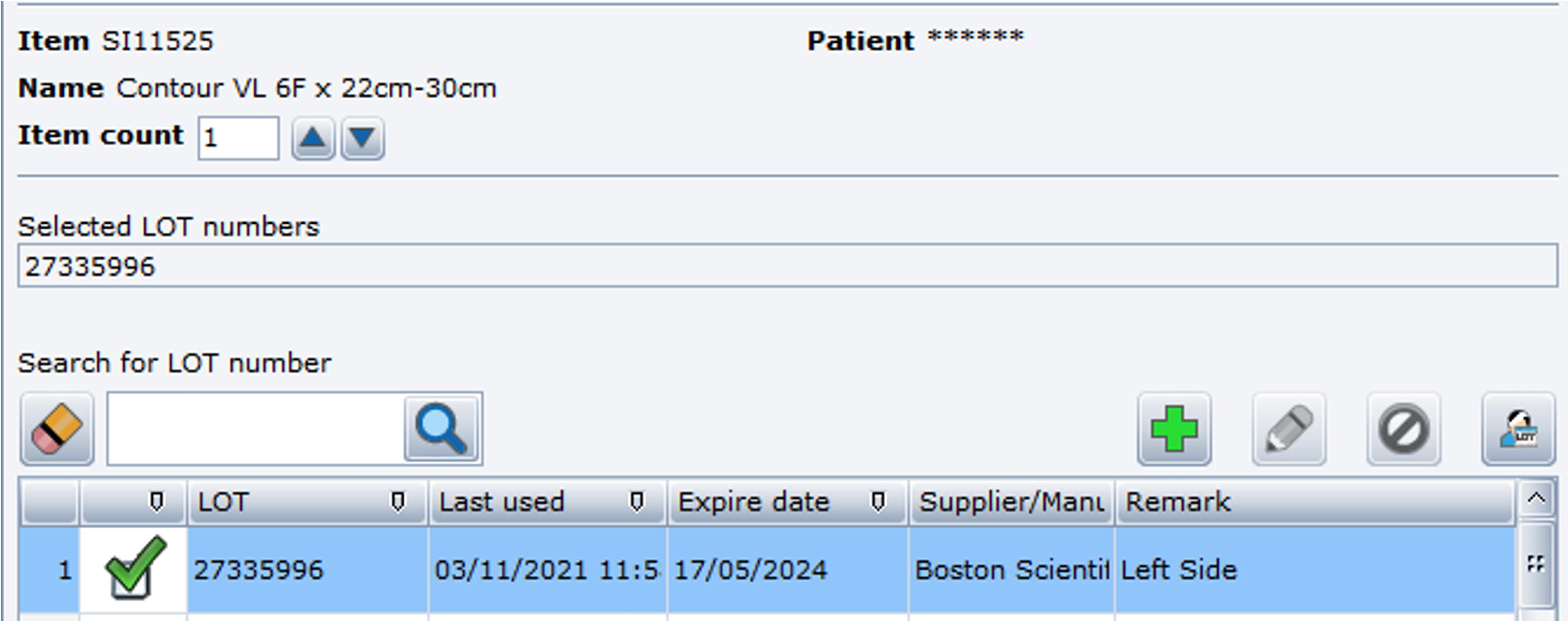
T-DOC instrument tracking system. Lot number of the implant, date of use, and laterality (left/right side) are documented by nurses prior to use.
Subsequent processes include the consolidation of data using a data repository, the Electronic Health Intelligence System (eHINTS), which also allows automated verification and cross-checking of all logged data. This is followed by data upload to a digital database—the Research Electronic Data Capture (REDCAP) platform—to trigger email reminders to clinicians if stent removal was not performed within a pre-defined time. In the event that one party omits the entry of stent-related data, this error will be detected during verification and cross-checking, and the incomplete data packet will not be uploaded to REDCAP. The administrator would be informed of this error, and the relevant clinical party would be notified for rectification.
In the REDCap database system, when a stent is found to be retained beyond a predefined time interval, an automated reminder is sent via email to the clinician on a weekly basis (Fig. 3). Removal of the stent and update of the relevant data field will subsequently deactivate these email reminders. When required for audit or manual verification of data in eHINTS, T-Doc, or REDCAP, the administrator maintains controlled access for this specific purpose.
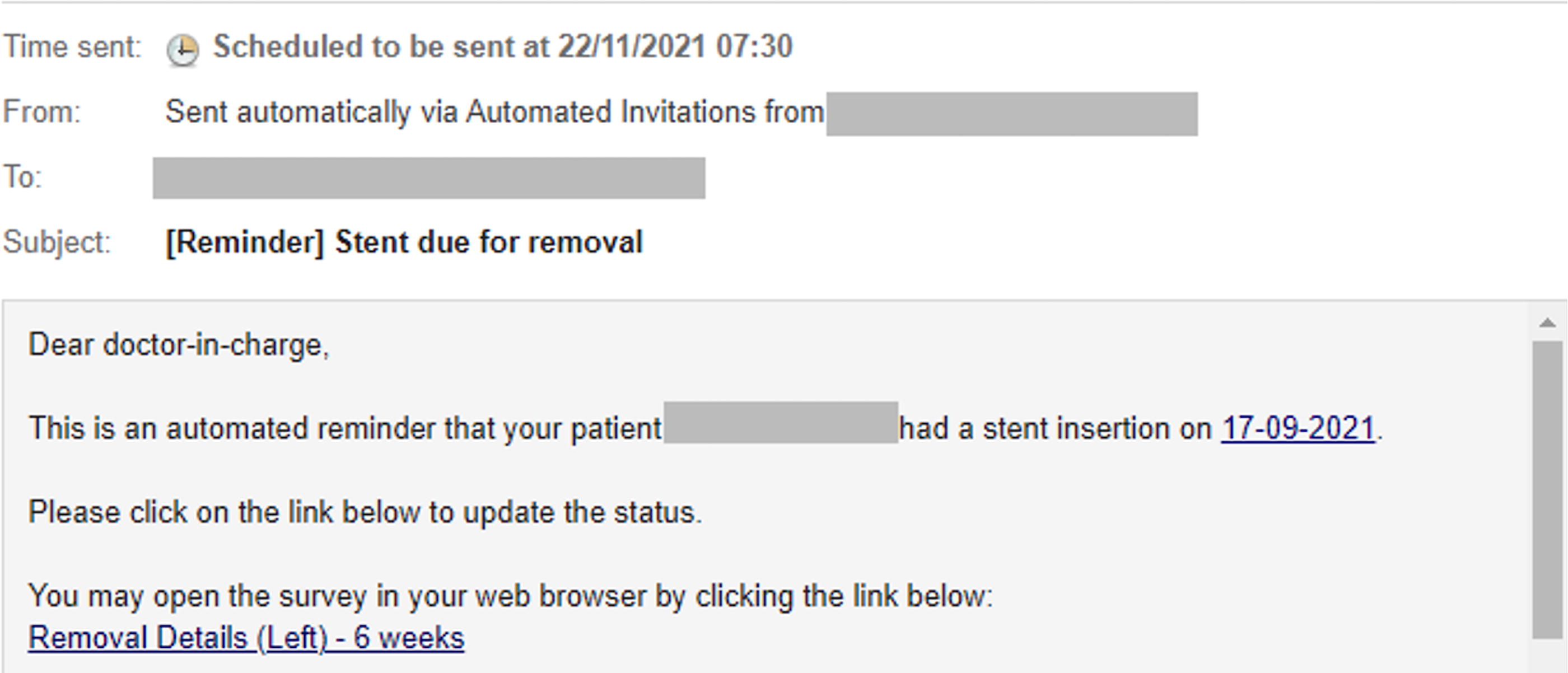
Automated email reminders sent to clinicians past a pre-defined date to ensure overdue stents are removed.
Clinical validation
The TRACER digital registry has been utilized as a clinical service in our institution since its inception in 2021. To evaluate the performance of TRACER in stent tracking and reminders, we reviewed the records of all patients undergoing stent placement for any indication between January 2022 and February 2023.
Results
A total of 1056 ureteral stents were inserted through 927 procedures in 713 patients, and their characteristics are summarized in Table 1. Most of the stents were inserted after routine ureteroscopy and laser lithotripsy (74.3%).
Baseline Characteristics of the Cohort
IQR, interquartile range.
All stents inserted within the period of analysis were tracked by the TRACER system, including 15 (1.4%) stents that might have been omitted from tracking owing to missed barcode scanning, errors in the T-DOC system that failed to mark a stent as used, or lack of documentation of stent insertion. These were highlighted by TRACER during data validation prior to being uploaded onto the central EMR database.
The performance of the TRACER system is further shown in Table 2—a total of 1034 (97.9%) stents were removed, and the median time between insertion and removal was 18 (12–35) days. Sixty-one (5.9%) stents were identified by TRACER as not removed past the predefined time period. Forty-one of the patients (3.9%) were contacted and successfully returned for stent removal. Seven patients (0.7%) were found to be deceased prior to stent removal, and another 8 (0.8%) had their stents removed at another institution. The remaining five patients (0.5%) identified had long-term stents inserted to relieve malignancy-induced ureteral obstruction and were due for a change of stent at a later date. Most importantly, all stents inserted were accounted for within the period of evaluation.
Results from TRACER Monitoring and Follow-up After Stent Insertion
Timely removal of stent defined as 3 months for regular ureteral stents and 6 months for tumor stents.
TRACER, Automated System for Tracking, Recording, and Reminding of Implants.
Discussion
This study has shown that the TRACER is highly effective in tracking, tracing, and reminding clinicians who routinely deploy ureteral stents—out of 1056 stents inserted within our study period, a total of 61 (5.9%) were not removed within the pre-determined time but all of them were successfully accounted for by TRACER. The key advantages of the system that make this possible include (1) a two-pronged trigger to confirm insertion of a ureteral stent, (2) automated clinician reminders after a pre-determined time to ensure timely stent removal, and (3) cessation of the reminders after the stent has been marked as removed.
In TRACER, the two-party trigger reduces the omission of tracking and avoids unintentional misses. If a single-party trigger system were deployed in our study, up to 15 stents would have been potentially missed and not tracked because of human omission. Although it is arguable that duplication of tracking triggers may be unnecessary, the study team is of the opinion that the initial step in TRACER is of paramount importance and therefore fundamentally important to ensure a zero omission policy. In addition, our use of a keyword in the EMR to trigger stent tracking allows for TRACER to be adapted across different EMR systems as minimal adaptions have to be made to underlying processes.
We believe that TRACER can be scaled to other institutions without much difficulty, as the underlying concept is simple to adapt. Scanning of a barcode or radiofrequency identification tag on an implant is common practice in the operating theater for charging and tracking purposes, and TRACER leverages this practice to obtain implant information. Some minor modifications might however be required to account for different surgical device tracking systems. Furthermore, the digital database we utilized (REDCAP) to consolidate the stent information is open source and free to utilize, thus allowing TRACER to be scaled to other institutions at minimal cost while ensuring data security. There is also minimal operational expenditure for TRACER, except for a system administrator who is not required full-time as most processes within TRACER are automated, and data error verification and audits occur infrequently.
Given the push toward digitalization in health care, several other digital ureteral stent registries have been described in current literature. Ziemba et al. 10 published their experience using the Ureteral Stent TrackerTM, a mobile phone application co-developed by Boston Scientific that allows clinicians to log stent insertion, schedule a date of removal, and subsequently document stent removal. Use of this application allowed 3% of patients who defaulted on their scheduled stent removal appointment to be identified. Although this system has been operationalized into a mobile phone application to improve accessibility, it still requires manual entry of stent information and is dependent on the diligence of the primary surgeon to log every individual stent inserted. Wagner 8 described another system based on integration with institutional EMR, where stents scanned during insertion by nurses were marked as “implanted” on the Epic system and manually marked as explanted by the surgeon upon removal. Stents with the “implanted” status are evaluated every quarter to determine if they are overdue. In their series of 152 patients, no stents were left retained, but this method is largely manual in nature with no automated clinician reminders to ensure removal of stents. Unlike a purely automated system such as TRACER, both studies still relied heavily on manual inputs and are therefore subject to inefficiencies and human errors that a digital registry is supposed to address.
Other studies utilized billing codes as a means to fully automate the stent tracking process—Kim et al. 11 used different billing codes for stent placement, replacement, or removal; different codes were specified for left or right stents as well. For stents not removed within a predefined period of 120 days, email notifications were sent to the attending physician. This system managed to identify 3.4% of patients who might have been lost to follow-up, and all stents registered were appropriately tracked. Similarly, Lin et al. 9 also described a computerized stent monitoring system based on billing codes specified separately for unilateral or bilateral stent insertion, as well as for stent insertion, replacement, and removal. With an impressive database of more than 10,000 patients, the system successfully identified 896 (8.87%) patients who had an indwelling stent but did not return for removal, and there were no forgotten stents in the 8-year period of the study. Despite a difference in methodology, the performance of TRACER appears comparable with these studies, with the identification of 3.9% of patients who defaulted stent removal, and no cases of forgotten ureteral stents. Although the use of billing codes might be an effective method for tracking ureteral stents, there are several limitations that limit its generalizability. Firs, physician omission of charge codes during stent insertion/removal is common and accounted for 35% of the “forgotten” stents tracked by the system described by Kim et al. 11 Second, procedural billing codes tend to vary between institutions—in our practice, billing codes for stent insertions and removals do not differ by laterality, and stent replacements during operative procedures are generally not charged as a separate procedure. Such differences in the practices of charging might limit the transferability of this system between institutions but might be overcome by a system that tracks the individual stent inserted instead.
Despite the effectiveness of the TRACER system, there are some limitations. First, a manual update of stent removal is required for the deactivation of the user reminders. There is no doubt that this step can also be automated, but the current manual updates allow for all stents to be accounted for, especially for patients who have transferred care to another institution, or for those who have passed on. Second, although TRACER was developed and implemented for ureteral stents, its applicability in another implant may simply require minor modifications to data fields. In the adoption of TRACER in another work environment outside the operating theater, it is possible that minor workflow modifications may be required, and this may impact the magnitude of time savings to clinical staff.
In conclusion, this validation study shows that TRACER is an effective and sustainable system with a significant role to play in tracking and reminding clinicians deploying ureteral stents, in order to minimize the risk of a retained stent and its associated complications, while overcoming inefficiencies and omissions associated with manual tracking systems. In addition, TRACER is potentially scalable to other implant types and also to other EMR environments.
Footnotes
Authors’ Contributions
H.J.L., J.Y.J.T., and L.L.S.: Conception and design. H.J.L., J.Y.J.T., and L.L.S.: Data analysis and interpretation. S.Y., K.C.H.H., G.F.T., M.T., S.Y.C., and M.S.K.T.: Data acquisition. H.J.L., S.Y., and L.L.S.: Drafting article. P.F.K., K.C.H.H., G.F.T., M.T., and L.L.S.: Critical revision of the article. H.J.L. and J.Y.J.T.: Statistical analysis. L.L.S.: Supervision.
Author Disclosure Statement
All authors have no conflict of interest to disclose.
Funding Information
No funding was received for the purpose of this study.