
Abstract
Objective:
To optimize thulium fiber laser (TFL) settings for effective stone fragmentation although minimizing thermal injury in confined ureteral spaces using a three-dimensional ureter model.
Materials and Methods:
A hydrogel-based ureter model was maintained at 37.2 ± 0.5°C, with a cylindrical BegoStone (10 × 10 mm, 1.00 ± 0.07 gm) occluding the ureter. Ureteroscopy was performed using a 150 µm TFL fiber for 3 minutes with room temperature irrigation and differing rates (0, 20, 40 mL/min) and power settings (6.4 to 20 W). Maximum sustained temperature (MST) and cumulative thermal dose (cumulative equivalent minutes at 43°C) were assessed against a 120-minute safety threshold. We also evaluated the effects of ureter volume and irrigation temperature. Stone mass treated was calculated by subtracting the mass of residual fragments >3 mm from the initial mass.
Results:
At 6.4 and 10 W, MSTs were below body temperature, and thermal doses were under 1 minute, indicating minimal thermal risk. At 20 W with 20 mL/min irrigation, MST exceeded 43°C within seconds, and thermal doses surpassed 120 minutes. Treatment efficiency was highest at 20 W (1.58 mg/s), followed by 10 W (1.15 mg/s) and 6.4 W (0.78 mg/s). Among 10 W settings, 1.0 J/10 Hz was more efficient than 2.0 J/5 Hz and 3.0 J/3 Hz. Safe settings produced 95.5% fine dust, whereas high-energy pulses 2–3 J produced significantly more fragments (1–3 mm) compared with settings with pulse energy 0.5–1.0 J. Increasing irrigation to 40 mL/min or using 15°C irrigation effectively reduced MST and improved efficiency, particularly at 20 W.
Conclusion:
Our study demonstrates the risk of thermal injury with 20 W TFL treatment. Conversely, 10 W settings at 2.0 J/5 Hz are safe and effective for fragmentation. Future research will focus on validating these optimal settings for human stone treatment.
Introduction
Despite the significant clinical interest in new laser technologies, a consensus among urologists regarding optimal settings for thulium fiber laser (TFL) in laser lithotripsy (LL) remains elusive. 1,2 Recent in vitro studies 1,3,4 and clinical investigations 5,6 have demonstrated effectiveness of TFL, particularly in stone dusting, positioning it as a viable alternative to the current gold standard, the Holmium (Ho):Yttrium-Aluminum-Garnet (YAG) laser. 7 However, concerns persist regarding fragmenting power of TFL, especially for treating hard stones such as brushite and calcium phosphate (melting temperature = 1670°C) in the ureter. 4,8 This is potentially related to lower peak power of TFL compared with Ho:YAG. Unlike the Ho:YAG laser, high water absorption of TFL may precipitate rapid temperature increases during ureteral stone treatment, especially amplified in more confined spaces, such as when treating immobilized and impacted stones. This thermal escalation has been associated with risks of thermal injury and ureteral strictures after ureteroscopy with TFL, 8,9 prompting a Food and Drug Administration recall for software updates to mitigate these risks during LL procedures. 8
This study aims to determine the TFL settings that maximize treatment efficiency and fragmentation while minimizing the risk of thermal injury in ureteral stone lithotripsy, utilizing an in vitro benchtop model. In addition, the effects of ureteral diameter, irrigation flow rate (IFR), and irrigation fluid temperature were evaluated.
Materials and Methods
Artificial stone and ureter model preparation
Experiments were conducted in an anatomically realistic three-dimensional ureter model (Fig. 1b) made from synthetic ballistic gel (Humimic Medical, SC) to simulate renal tissue. 10 Cylindrical BegoStone phantoms (10 × 10 mm, 1.00 ± 0.07 g) were prepared with a 5:2 powder-to-water ratio and soaked for 24 hours. 11 The experimental setup (Fig. 1a, c) involved placing a stone in the ureter model such that it fully occluded the ureteral lumen. The model was submerged in a 37.2 ± 0.5°C water bath, replicating clinical conditions using a heater. A ureteroscope was inserted through an 11/13 Fr access sheath (Boston Scientific Corporation, Marlborough, MA, USA), with irrigation managed via a peristaltic pump (Masterflex®) to control thermal buildup and ensure visibility during the procedure. Pulse energy was verified using a Vega ROHS energy meter (Ophir Optronics Solutions Ltd., USA) before each treatment.

Experimental models
The primary model used a 6.6 mm ureter with room-temperature irrigation (20–22°C) at 20 mL/min. Secondary experiments studied the effect of ureter diameter (4.4 mm), irrigation rates (0–40 mL/min), and irrigation fluid temperature (∼15°C). The dimensions, including the length, diameter, and the ratio of the upper to lower ureter diameter relative to the stone, were chosen based on the data provided in literature. 12 The maximum irrigation rate tested was 40 mL/min, which represents the upper limit of clinically relevant irrigation rates during ureteroscopy at irrigation pressure of 200 cmH2O with a laser fiber in the working channel. 13
Thermal injury risk assessment
Temperature was monitored every 0.2 second (response time) using PFA K-type thermocouples (TCs) (OMEGA, Norwalk, CT, USA) (Fig. 1b). The measurement locations (Supplementary Fig. S1) included TC1 (distal to the stone, assessing model control during impacted stone treatments), TC2 (between the stone and the ureteral lumen wall), TC3 and TC4 (proximal to the stone, near the fiber tip, positioned 1 < D < 3 mm from the initial stone surface), and TC5 (within a body-temperature water bath). During the impacted stone treatments, TC1 is expected to remain at bath temperature, as no irrigation fluid should reach this location. For each experiment, the maximum sustained temperature (MST) was recorded, defined as the highest temperature maintained for at least 3 seconds. MST values were compared against safety thresholds of 43°C, where cell death may begin, and 50°C, at which widespread necrosis is likely to occur.
14
Thermal injury risk was assessed by calculating the cumulative equivalent minutes at 43°C (CEM43°C), using the following thermal dose formula,
15
with a safety threshold of 120 minutes:
16
Laser treatment
A TFL system (TFL-50/500-QCW-AC, IPG Photonics, Oxford, MA) was used. A flexible ureteroscope (Dornier AXISTM, 3.6 F working channel, Munich, Germany) with a 150 μm core-diameter fiber was operated by an experienced endourology fellow. Stones were fragmented, starting near the center of the stone and working outward with the goal of breaking the stone into fragments
Summary of the Thulium Fiber Laser Parameters Employed during the Laser Lithotripsy Experiments, Including Pulse Energy, Frequency, Full-Width Half Maximum Pulse Duration (
For simplicity in presentation, the 3J/3 Hz combination is grouped in the 10W power category.
Statistical analysis
Multigroup statistical comparisons were made using one-way ANOVA. Pairwise comparisons were made between individual TFL settings using Student’s t-test. Sample size was calculated to detect differences in efficiency between settings. A sample size calculation was performed based on prior studies showing differences in efficiency between settings ranging from 0.98 to 0.49 mg/s. 1 Assuming normal distribution, we would need 3 trials at each setting to have a 95% power to detect a similar change in efficiency between settings with alpha 0.05. p-Values below 0.05 were considered statistically significant. Statistical analysis was performed using Stata 18.0 (StataCorp, College Station, TX, USA).
Results
Thermal injury potential
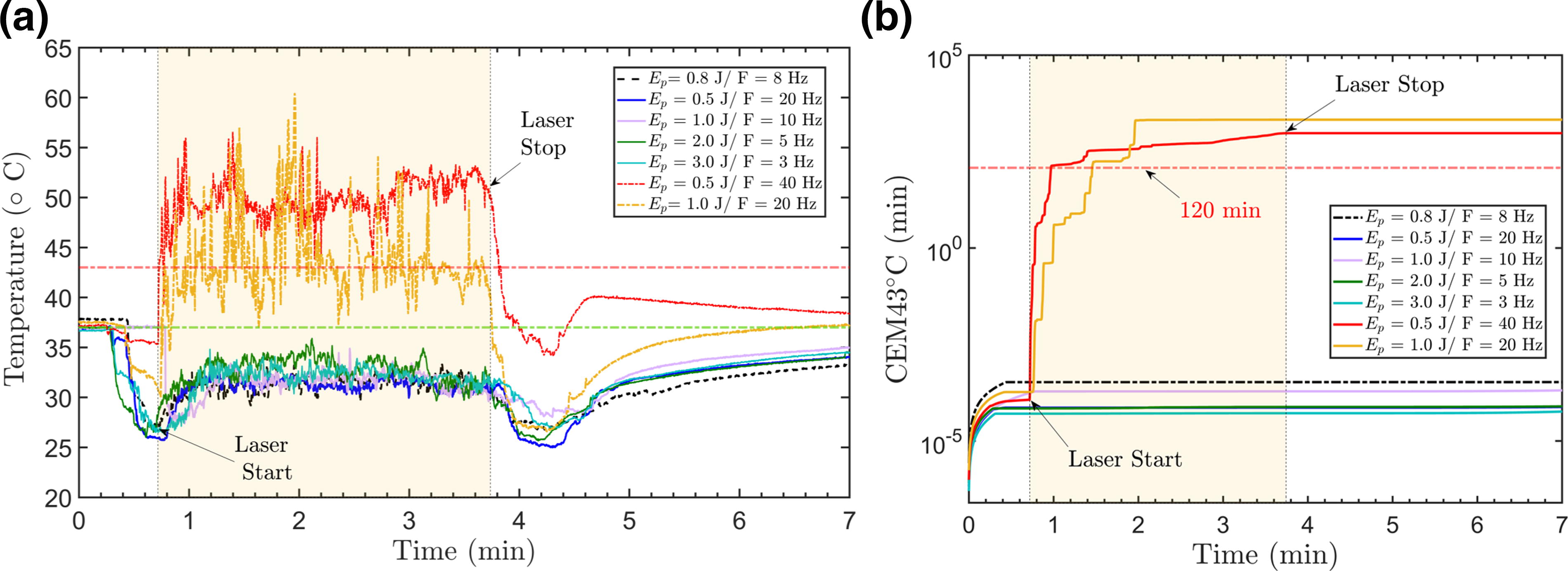
A total of 33 experiments were performed using the primary experimental model. At 6.4 W and 10 W, MST remained below body temperature, and thermal doses were under 1 minute (Fig. 2a, b, Table 2). At 20 W, MST exceeded 43°C, and thermal doses surpassed 120 minutes, with thresholds exceeded after 87.6 seconds at 0.5 J/40 Hz and 58.4 seconds at 1.0 J/20 Hz. MST differed significantly between power levels (p < 0.001), being higher at 20 W (46.9 ± 4.1°C) compared with 6.4 W (31.3 ± 1.0°C, p < 0.001) and 10 W (32.0 ± 1.8°C, p < 0.001). Among the 10 W settings, there was no significant variation in MST (p = 0.478). There were no significant pairwise differences found among the 10 W settings (all p > 0.05). At 20 W, MST was higher with 1.0 J/20 Hz (50.0 ± 2.5°C) compared with 0.5 J/40 Hz (43.8 ± 2.6°C, p = 0.038).
Comparison of Maximum Sustained Temperature, Maximum Cumulative Thermal Dose (CEM43°C, Min), and Time to Safety Threshold, Where the Safety Threshold is Cumulative Equivalent Minutes at 43°C >120 Min, for Different Settings at a Constant Irrigation Rate of 20 mL/Min in the 6.6 mm Ureter Model
These data correspond to the TC3 thermocouple, which is approximately D ≤1 mm from the stone surface on the distal side and nearest to the fiber tip during the treatment.
CEM43°C = cumulative equivalent minutes at 43°C.
Treatment efficiency and fragment size distribution
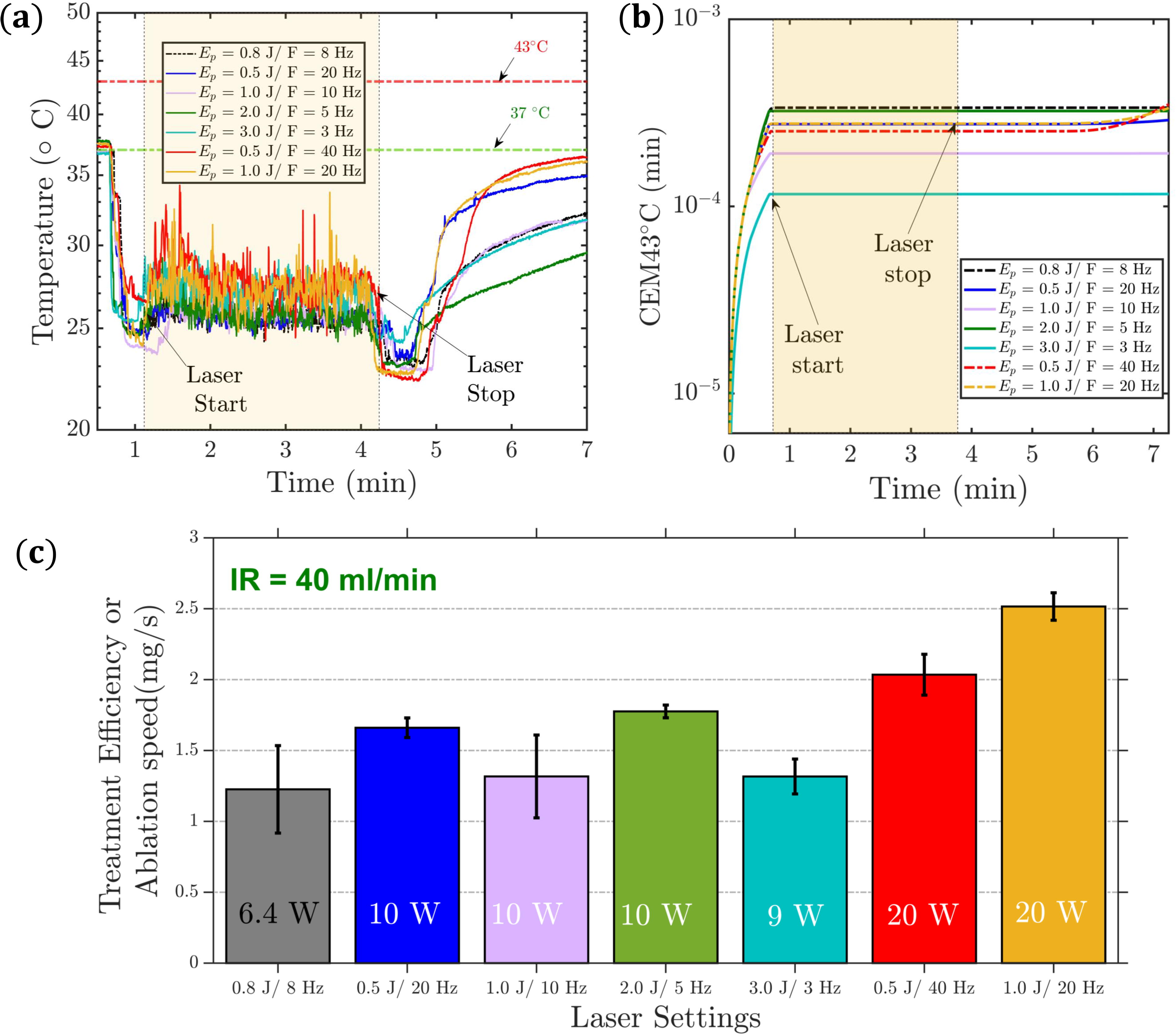
Across all settings, an average of 21.0% ± 5.6% of the stone mass was treated, with treatment efficiency (mg/s) differing by power level (p < 0.001). Pairwise comparison showed that 10 W (1.15 ± 0.25 mg/s) was more efficient than 6.4 W (0.78 ± 0.17 mg/s, p = 0.023), whereas 20 W (1.58 ± 0.19 mg/s) was superior to both 6.4 W (p < 0.001) and 10 W (p < 0.001) (Fig. 3A). Within 10 W settings, 1.0 J/10 Hz (1.34 ± 0.28 mg/s) was more efficient than 2.0 J/5 Hz (0.99 ± 0.10 mg/s, p = 0.016) and 3.0 J/3 Hz (1.00 ± 0.06 mg/s, p = 0.015), with no other significant differences (all p > 0.05). No difference in efficiency was observed between 20 W settings (0.5 J/40 Hz vs 1.0 J/20 Hz, p = 0.888). Across all settings, 95.0% ± 4.0% of the treated mass was fine dust, 2.3% ± 1.5% was dust (0.25–1 mm), and 2.7% ± 3.0% were stone fragments (1–3 mm). Among the 10 W settings, the percentage of 1 to 3 mm fragments differed (p = 0.017) (Fig. 3b). Specifically, 2.0 J/5 Hz (5.1% ± 3.2%) had a higher percentage of fragments than both 0.5 J/20 Hz (1.6% ± 2.0%, p = 0.042) and 1.0 J/10 Hz (0.8% ± 0.8%, p = 0.009). Similarly, 3.0 J/3 Hz (4.9% ± 3.6%) produced more fragments than 1.0 J/10 Hz (p = 0.022), with no significant difference between 2.0 J/5 Hz and 3.0 J/3 Hz (p = 0.902). High-energy settings were observed to demonstrate increased burning and charring.

Comparison between 6.6 mm vs 4.4 mm in an anatomical ureter model:
Effect of ureteral diameter
We repeated the experiments for the 10 W settings using a 4.4 mm diameter model and compared the thermal injury risk and treatment efficiency metrics to those from the 6.6 mm model. Irrigation was maintained at 20 mL/min at room temperature.
Treatment efficiency showed no significant difference between the smaller (1.03 ± 0.36 mg/s) and the larger ureter (1.15 ± 0.25 mg/s, p = 0.277) (Fig. 3a). In addition, there was no significant difference in percentage of 1–3 mm fragments between the smaller (2.5% ± 4.2%) and the larger ureter (3.1% ± 3.2%, p = 0.629) (Fig. 3b, c). However, average MST was higher for the smaller (34.9 ± 2.1°C) compared with the larger one (32.0 ± 1.8°C, p < 0.001), although it remained below body temperature with minimal thermal doses for all 10 W settings (Table 3).
Comparison of Maximum Sustained Temperature and Maximum Cumulative Thermal Dose (CEM43°C, Min) for Different 10W Settings at Constant Irrigation Rate = 20 mL/min between Bigger and Smaller In Vitro Ureter Models (Diameter = 6.6 mm vs 4.4 mm)
CEM43°C = cumulative equivalent minutes at 43°C; Dia. = Diameter of ureter model.
Effect of irrigation rate
Experiments for all settings were repeated at different irrigation rates (0 mL/min and 40 mL/min) using a 6.6 mm model and room temperature irrigation. Without irrigation (0 mL/min), all treatments exceeded 70°C, leading to early termination, with the 43°C threshold surpassed within 4 seconds. Higher laser power reduced the time to exceed thermal safety thresholds (Fig. 4, Table 4). At 10 W, no significant differences were observed in the times to reach thermal thresholds (43°C, 50°C, and 70°C) between the 1 J/10 Hz and 2 J/5 Hz settings (p = 0.158, p = 0.580, and p = 0.724, respectively). At 6.4 W, the 50°C threshold was reached in 5.7 ± 0.6 seconds and the thermal dose threshold in about 9.5 seconds. At 10 W, these times were 4.7 ± 0.9 seconds and 6.8 ± 0.5 seconds, respectively, and at 20 W, they were 2.0 ± 0.4 seconds and 3.4 ± 0.3 seconds. Significant differences in these times were confirmed by one-way ANOVA (p < 0.001). Efficiency calculations were not performed because of early termination.

Comparison of Time to Reach Maximum Sustained Temperature T °C >43°C, T °C >50°C, T °C >70°C, Maximum Cumulative Thermal Dose (CEM43°C, Min), and Time to Safety Threshold, Where the Safety Threshold is Cumulative Equivalent minutes at 43°C >120 Min, for Different Settings at no Irrigation Flow in an In Vitro Ureter Model (Ureter Diameter = 6.6 mm)
These data correspond to the TC3 thermocouple, which is approximately D ≤1 mm from the stone surface on the distal side and nearest to the fiber tip during the treatment.
CEM43°C = cumulative equivalent minutes at 43°C.
With 40 mL/min irrigation, MST was lower than with 20 mL/min irrigation (Fig. 5a, b, Supplementary Table S1). At 6.4 W, MST was 25.6 ± 1.1°C (p = 0.003); at 10 W, it was 26.1 ± 0.8°C (p < 0.001); and at 20 W, it was 27.6 ± 0.7°C (p < 0.001). Thermal doses remained minimal, even at 20 W. Compared with 20 mL/min irrigation, average treatment efficiency was higher with 40 mL/min irrigation at 10 W (1.52 ± 0.27 mg/s, p = 0.036) and 20 W (2.28 ± 0.30 mg/s, p = 0.001) (Fig. 5c), with no significant difference at 6.4 W (1.23 ± 0.38 mg/s, p = 0.135).
Effect of irrigation temperature
To further mitigate thermal injury risk without increasing flow rate, we repeated the 20 W experiments using 15°C irrigation with the 6.6 mm model and 20 mL/min flow rate. This lower temperature irrigation decreased MST for 20 W settings to 36.20 ± 3.57°C compared with room temperature irrigation (p < 0.001). In addition, treatment efficiency increased significantly to 1.93 ± 0.14 mg/s with 15°C irrigation vs room temperature irrigation (p < 0.001) (Table 5).
Comparison of Treatment Outcomes for 20W Thulium Fiber Laser Settings at Room Temperature 20–22 °C with a Constant Irrigation Rate = 20 mL/Min vs Cold Irrigation (∼15 °C) in an In Vitro Ureter Model (Diameter = 6.6 mm)
CEM43°C = cumulative equivalent minutes at 43°C; Ep = pulse energy in Joules (J); RT = Room temperature 20–22 °C.
Discussion
Several in vitro studies have highlighted the risk of thermal injury during TFL treatments, although many did not incorporate stone ablation, a crucial aspect of clinical LL. 17,18 Evidence suggests that thermal effects are more pronounced in experiments with calculi, indicating that previous studies might have overestimated clinically safe power thresholds. The unique anatomy and confined volumes of the ureter 19 necessitate careful laser setting selection to ensure thermal safety and minimize the risk of postoperative ureteral stricture. 20 This is especially crucial for proximal or impacted ureteral stones with TFL, given its strong absorption in water. 21,22
Our in vitro experiments measured fluid temperature changes during TFL lithotripsy. The resulting temperature curves qualitatively agreed with previous studies, 3,23 showing temperatures rising after the initiation of laser activation to reach a stable, elevated MST value, before decreasing after the laser was switched off. Our study also exhibited a higher temperature increase in the smaller ureter compared with the regular ureter models, highlighting the challenge of thermal management in confined anatomical conditions and underscoring the importance of considering ureteral volume and treatment location. 23 In the primary model, the 2 J/5 Hz setting at 10 W exhibited a nonsignificant trend toward higher peak temperatures (32.8 ± 1.5°C) compared with the 1 J/10 Hz setting (31.7 ± 1.6°C, p = 0.212). Although the difference is not statistically significant, the observed pattern suggests that pulse energy influences thermal dynamics, even when the total power is held constant. This effect is likely attributed to longer pulse durations and the absence of thermal confinement. 24 As reported by Chan and associates, 24 variations in pulse duration can affect the extent of thermal diffusion, warranting further investigation. Rapid temperature increases at high power settings, especially with compromised irrigation, align with clinical reports of increased thermal injury risk under similar treatment scenarios. 8,23
Significant temperature increases occurred without irrigation, surpassing 43°C in under 4 seconds even at low power. This finding is concerning, as pausing irrigation is a common technique used to minimize stone movement during ureteroscopy, emphasizing the need for minimal laser activation during irrigation off periods. High-power settings (as much as 40 W) with low irrigation can lead to significant temperature elevation and potential in vivo injuries. 25,26 Increasing the irrigation rate to 40 mL/min mitigates thermal injury and enhances efficiency, especially at 20 W, corroborating the findings of Belle and coworkers. 9 However, lower irrigation rates (20 mL/min or below) are recommended to avoid high intrarenal pressure and minimize postlaser sepsis risk 17,27 while also reducing retrograde stone migration.
Under such flow rate constraints, our study suggests that using a 20 W setting may lead to excessive temperature rises within seconds, potentially causing thermal injury. CEM43°C provides a more accurate measure of thermal impact, capturing cumulative effects and preventing overestimation from brief temperature spikes. Our findings revealed that a 0.5 J/40 Hz setting, despite a lower MST, resulted in a higher thermal dose than a 1.0 J/20 Hz setting. Even maintaining temperatures between 41°C and 43°C for over 30 minutes can cause lasting urothelial damage, making CEM43°C a critical metric for evaluating thermal safety. 28
Chilled irrigation 29,30 fluid may be a viable alternative to increased IFRs for maintaining a safe temperature profile during LL, especially at 20 W settings (Supplementary Table S2) 25 or in confined volumes. However, extreme cooling (e.g., <10°C) poses potential clinical concerns, such as risks to tissue viability, perioperative shivering, and postoperative hypothermia by decreasing the patient’s core body temperature. 31,32 Although the definitive link between irrigation temperature and postoperative complications has not been conclusively established, these risks warrant caution. To balance these considerations, we selected 15°C as a moderate, clinically feasible temperature that retains the cooling benefits while mitigating the risks associated with extreme chilling. We found that 15°C irrigation effectively lowers intraluminal temperatures and enhances treatment efficiency, likely because of enhanced laser absorption (early Moses effect). 22 This contributes to both thermal ablation and cavitation-induced damage. 33 Specifically, MST values (Table 5) were 37.45 ± 2.33°C (0.5J/40 Hz) and 34.94 ± 4.39°C (1 J/20 Hz), demonstrating significant thermal mitigation without risking hypothermia or perioperative shivering. Using optimally colder or room temperature irrigation fluids, rather than chilled (4°C) or warmed fluids (37°C), 32 minimizes the risk of hypothermia and thermal damage to the ureteral lumen during laser use. Thus, irrigation fluid temperature not only influences thermal injury risk but also affects stone photothermal ablation and cavitation bubble dynamics. 22,33,34 However, we acknowledge that the clinical feasibility and safety of chilled or cooled irrigation necessitate further in vivo porcine model studies and clinical trials investigation to evaluate the real-world applicability and impact of this approach on patient outcomes. We hypothesize that an optimal irrigation fluid temperature exists to achieve the best stone ablation efficiency while maintaining a safe temperature profile with TFL.
Exploring lower energy and power settings (e.g., 0.4–0.6 J at 4–6 Hz) may further enhance safety margins without compromising clinical efficiency, particularly for less experienced practitioners or anatomically challenging scenarios. Although not explicitly tested, trends in our results suggest that these settings could further reduce temperatures with only modest reductions in fragmentation efficiency. 8
Our examination of fragment size distribution found that 2 J/5 Hz and 3 J/3 Hz resulted in a greater proportion of 1 to 3 mm fragments compared with other lower-energy settings. This finding aligns with prior research on Ho:YAG lithotripsy, 35 although there are key differences attributable to the lower peak power, reduced retropulsion, and potentially less fragmentation power of TFL. 8 These unique characteristics of TFL may provide a clinical advantage when combining effective fragmentation with reduced stone migration. Thus, when fragmentation is a desirable result, high-pulse energies of 2–3 J combined with low frequencies may be preferable with TFL. Furthermore, our findings emphasize that 2J/5 Hz demonstrated effective stone fragmentation; however, it necessitates careful application because of the potential for thermal injury, particularly when misfired or used in proximity to the urothelium. This risk is heightened in less experienced hands or during anatomically challenging cases. Clinical implementation of high-pulse energy settings should be approached judiciously. Based on our observations, 2.0 J is most appropriate at the start of the procedure when the fiber is securely centered on the stone and the stone provides adequate shielding to the ureteral lumen in impact stone scenarios. Toward the conclusion of the procedure or as the fiber approaches the urothelium, we recommend gradually reducing the pulse energy to 0.8–0.6 J to mitigate the risk of thermal injury without significantly compromising fragmentation efficiency. In addition, slower frequencies (e.g., 5 Hz) offer improved control, allowing precise fiber positioning and reducing misfire risks. Findings from our recent porcine model study 36 support this approach, demonstrating that 2 J/5 Hz achieved effective fragmentation with no visible damage on gross examination and only mild histologic analysis injuries without severe necrosis. These results highlight the importance of balancing efficiency with safety and advocate for the controlled judicious use of TFL settings to minimize thermal complications, such as ureteral strictures.
We acknowledge the study’s limitations, including the nontypical 180-second continuous lasing protocol and the use of BegoStone. Although BegoStone standardizes stone size and shape, its uniform composition and smooth edges, lacking natural fault lines, are not ideal for simulating stone fragmentation. Furthermore, although in vitro studies provide valuable insights, they cannot fully replicate the thermal behavior and tissue responses observed in clinical settings. These differences highlight the need for further validation of findings in in vivo models and clinical studies to establish safe and effective treatment protocols.
Future studies should focus on refining laser duty cycles, incorporating human stones, and validating results in porcine and other in vivo models to better define safe treatment parameters and optimal fragmentation settings. Moreover, although maintaining power below 10 W with a 20 mL/min irrigation rate or using higher flow rates and 15°C irrigation is intuitively expected to minimize the risk of thermal injury and potentially reduce the likelihood of ureteral stricture, the definitive link between these parameters and stricture formation has not been conclusively established and warrants further research.
Conclusions
This study emphasizes the critical need to balance fragmentation efficiency with thermal safety in TFL ureteral lithotripsy. Our in vitro study highlights the risk for thermal injury with 20 W TFL treatment, which generates unsafe intraureteral temperatures unless maintained at high irrigation rates (40 mL/min). Lower power settings (≤10 W) with adequate irrigation (20–40 mL/min) are recommended to minimize thermal injury and result in safe temperatures, even in the smaller ureter model. Treatment efficiency improved with higher power, and optimal stone fragmentation was observed with pulse energies of 2–3 J. Although the 2 J/5 Hz setting demonstrated effective fragmentation, its use should be approached cautiously because of the potential risks of thermal injury when misfired near the urothelium. Future clinical studies should validate these in vitro results to refine and enhance TFL lithotripsy protocols, ensuring they account for variations in ureteral volume.
Footnotes
Acknowledgments
The authors extend their gratitude to IPG Photonics for their technical assistance with the TFL system and acknowledge the support of Dornier MedTech for providing the Axis single-use flexible ureteroscope. Moreover, the senior author would like to express his gratitude to Dr. Margaret Pearle, M.D., Ph.D. of UT Southwestern for recommending the investigation of impacted ureteral stones by TFL at the 2023 ROCK Society Meeting in Boston, MA.
Authors’ Contributions
A.M., E.J.M., P.Z., and M.E.L.: Conception and design. A.M., E.J.M., A.W.S., and R.E.M.: Data acquisition. A.M., E.J.M., R.E.M., J.A., P.Z., and M.E.L.: Data analysis and interpretation. A.M., E.J.M., R.E.M., J.A., G.M.P., P.Z., and M.E.L.: Drafting the article. A.M., E.J.M., A.W.S., R.E.M., J.A., G.M.P., P.Z., and M.E.L.: Critical revision of the article for scientific and factual content. E.J.M. and A.M.: Statistical analysis. J.A., G.M.P., P.Z., and M.E.L.: Supervision.
Author Disclosure Statement
M.E.L. is a consultant for Boston Scientific. All other authors have nothing to disclose.
Funding Information
This project is supported by the National Institutes of Health (NIH) through grants 1P20DK135107-02 and 2R01DK052985-26.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Video S1
Supplementary Video S2
Supplementary Video S3
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.