
Abstract
Purpose:
Urine cultures are routinely used to inform preoperative antibiotic choice and duration prior to endourologic surgery. The presence of mixed flora in preoperative urine cultures holds unclear clinical significance. This study examines infectious outcomes after ureteroscopy in patients with preoperative mixed flora urine cultures.
Materials and Methods:
A retrospective cohort study was conducted on adult patients who underwent ureteroscopy with laser lithotripsy between January 2014 and June 2024 who had urine cultures performed within 60 days preoperatively. Patients were categorized into cohorts based on their preoperative urine culture: mixed flora, negative, or positive. Postoperative urinary tract infection rates within 30 days were compared between cohorts, and logistic regression was performed adjusting for demographic and clinical variables.
Results:
We identified 5166 patients who underwent ureteroscopy with laser lithotripsy (2139 mixed flora, 1525 negative, 1502 positive). Preoperative antibiotics were used more often in the mixed flora cohort (29%) than in the negative cohort (24%, p = 0.007) but less frequently than in the positive cohort (57%, p < 0.001). Postoperative infections were visualized in 165 patients (8%) in the mixed flora cohort, compared with 88 (6%) in the negative cohort (p = 0.067) and 237 (16%) in the positive cohort (p < 0.001). Multivariable logistic regression demonstrated that positive cultures were associated with an increased risk of infection (odds ratio [OR] = 1.95, 95% confidence interval [CI] = 1.49–2.55, p < 0.001), but negative cultures had a similar risk of infection compared with mixed flora (OR = 0.79, 95% CI = 0.56–1.11, p = 0.177). Within the mixed flora cohort, preoperative antibiotic treatment was not associated with decreased postoperative infection (OR = 0.99, 95% CI = 0.66–1.47, p = 0.964).
Conclusions:
While patients with preoperative mixed flora urine cultures received preoperative antibiotics more often than patients with negative urine cultures, they were not at higher risk for postoperative infection. Routine preoperative antibiotic use in patients with mixed flora cultures may not be effective in reducing infectious complications after ureteroscopy.
Introduction
Ureteroscopy with laser lithotripsy is the standard of care for many patients with ureteral and renal calculi. 1 Postoperative urinary tract infection (UTI), sometimes manifesting as sepsis, is a significant source of morbidity after these surgeries. 2,3
It is widely recognized that patients with positive preoperative urine cultures are at increased risk of infection and sepsis. 4 –7 However, there is no consensus regarding the perioperative management of patients with bacteriuria. In the absence of a symptomatic infection, the current best practice statement from the American Urological Association (AUA) recommends a single dose of perioperative antibiotics for patients undergoing ureteroscopy. 8 While not specifically recommended by the AUA, most endourologists report prescribing an extended course of preoperative antibiotics in patients with asymptomatic bacteriuria prior to ureteroscopy, though the duration is variable. 9
The optimal perioperative management of patients with urine cultures growing mixed flora (MF) is particularly uncertain. MF cultures are sometimes associated with specimen contamination but may also represent true bacteriuria with pathogenic potential. 10 –12 The clinical significance of MF in the perioperative setting is unknown, as is the potential benefit of preoperative antibiotic treatment in these patients. The objective of this study is to investigate the risk of postoperative infection after ureteroscopy in patients with MF cultures and to assess whether there may be benefits for preoperative antibiotic therapy.
Materials and Methods
We queried retrospective patient data within the Duke University Health System between January 2014 and June 2024. 13 Patients at least 18 years of age with a Current Procedure Terminology code for ureteroscopy with laser lithotripsy (52353, 52356) were included. Pregnant patients, those undergoing concurrent percutaneous nephrolithotomy (50080, 50081), or patients on chronic antibiotic prophylaxis for transplants or recurrent UTIs were excluded. Additionally, patients without a urine culture result available within 60 days before ureteroscopy were excluded. We collected patient demographics and medical history; the burden of comorbid conditions was summarized by calculating the Elixhauser Comorbidity Index. 14
Preoperative characteristics
Preoperative urine cultures within 60 days were captured. Patients were categorized into cohorts based on their preoperative urine culture: MF, negative, or positive. Positive cultures were defined as bacterial growth of over 10,000 colony-forming units (CFUs) per high-power field. If multiple urine cultures were performed with different results, the patient was assigned to the presumed higher-risk group (positive > MF > negative). Patients were defined as having received preoperative antibiotics if they received antibiotics within the 7 days leading up to surgery, not including the day of surgery. Each patient also received guideline-concordant preoperative antibiotic prophylaxis at induction. Most recent preoperative urinalysis counts for white blood cells within 60 days were also collected. Pyuria was defined as urine white blood cells exceeding 10 per high-power field, based on institutional guidelines. Placement of a stent (52332) or nephrostomy tube (50432, 50435) within 60 days preoperatively was noted.
MF definition
At our institution, urine cultures with two or more organisms are designated as MF and reported as “mixed urogenital flora, probable contaminant” if either of the following criteria is true: All organisms are nonsignificant or not known uropathogens. One of the organisms is considered a significant uropathogen but in 10-fold lesser quantity than the concentration of nonsignificant organisms. For example, 1000 CFUs per milliliter of a significant uropathogen compared with 10,000 CFU per milliliter of nonsignificant organisms.
Postoperative characteristics
Outcomes were defined using the International Classification of Diseases codes documented within 30 days after ureteroscopy. The primary outcome was postoperative UTI, which included codes for UTI (N39.0, 599.0), urosepsis (A40.0 to A41.0, R65.2, R65.20, R65.21, 038.9, 995.91), cystitis (N30.00; N30.91; N30.80; N30.0; N30.01; N30.90, N30.9, N30.8, 595.0; 595.9; 595.89, 590.9), pyelonephritis (N10, N13.6, 590.10; 590.11, 590.8, 590.1), fever (R50.9, R50.82), or bacteremia (R78.81, 790.7).
Statistical analysis
Demographics and preoperative characteristics were compared between cohorts using chi-squared tests, analysis of variance tests, or Mann–Whitney U tests, as appropriate. Where analysis of variance tests demonstrated significance, pairwise Mann–Whitney U tests were applied with Bonferroni correction. Multinomial logistic regression assessed the association between preoperative culture and the primary outcome, adjusting for demographic and clinical variables, such as Elixhauser comorbidities and preoperative antibiotic use. Analysis was performed in R version 4.4.1 (The R Foundation for Statistical Computing) using the stats 15 and rstatix 16 packages, with p-values less than 0.05 indicating significance.
Results
Overall cohort characteristics
In total, 5166 adult patients met inclusion criteria (Fig. 1). Median age was 59 (interquartile range 45–69) years, and 2697 (52%) patients were female (Table 1). Preoperative cultures were MF in 2139 (41%) patients, negative in 1525 (30%), and positive in 1502 (29%). Significant variation existed between cohorts in age, sex, body mass index (BMI), and Elixhauser Comorbidity Index. Pairwise analysis suggested that compared with negative culture patients, mixed (p = 0.002) or positive (p = 0.001) cohorts had varying racial composition. Preoperative stent or nephrostomy differed among positive compared with either mixed (p < 0.001) or negative (p < 0.001) culture patients. Additionally, pyuria was less common in the negative culture cohort (18%) and more common in the positive culture cohort (52%) compared with MF (26%, both p < 0.001). Preoperative antibiotics were less common in the negative culture cohort (24%, p < 0.001) and more common in the positive culture cohort (57%, p < 0.001) compared with MF (26%). Among patients prescribed preoperative antibiotics, 52 (8.4%) MF, 31 (8.3%) negative culture, and 165 (19.1%) positive culture patients developed infectious outcomes.
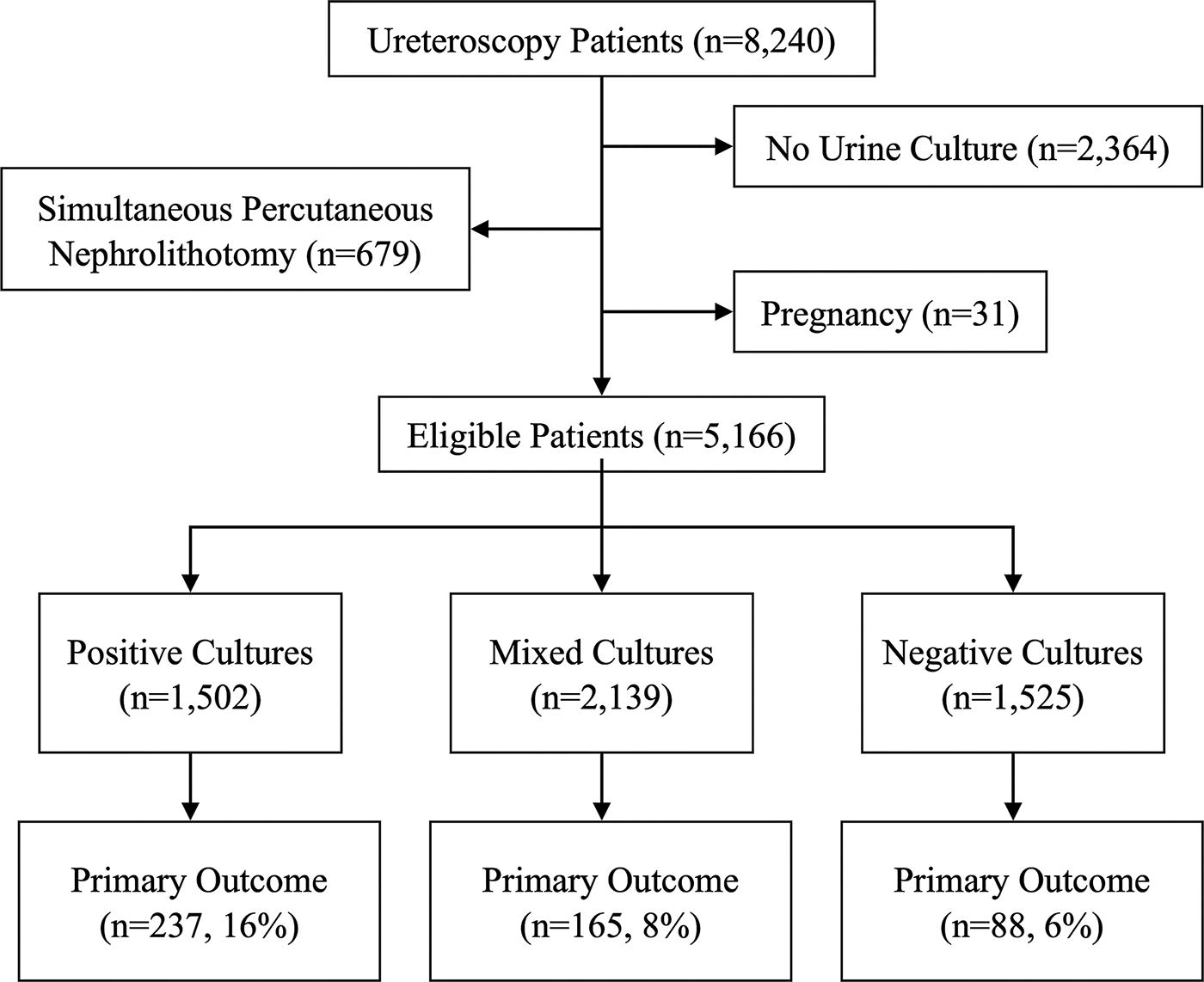
Diagram to report the flow of participants through the study.
Patient Characteristics, Summarized Among the Cohort and Stratified by Culture
IQR = interquartile range.
Postoperative infection
Postoperative UTIs were visualized in 165 (8%) patients in the MF cohort, 88 (6%) patients in the negative cohort, and 237 (16%) patients in the positive cohort (Fig. 2). The positive culture had heightened incidence compared with MF (p < 0.001) or negative (p < 0.001) cohorts, while MF and negative cohorts were similar (p = 0.067).

Outcomes were summarized among the cohort and stratified by culture. Cohort comparisons, with adjusted p-values calculated from pairwise testing using Bonferroni correction. Bars represent the percent incidence of outcomes with mixed flora (MF), negative (−), or positive (+) culture groups.
On multivariable logistic regression, patients with negative urine cultures were not associated with a significantly different risk of infection than those with MF cultures (odds ratio [OR] = 0.79, 95% confidence interval [CI] = 0.56–1.11, p = 0.177, Table 2). Positive cultures were associated with a higher risk of infection than MF cultures (OR = 1.95, 95% CI = 1.49–2.55, p < 0.001). Pretreatment with antibiotics was associated with heightened odds of infection (OR = 1.59, 95% CI = 1.25–2.01, p < 0.001).
Multivariable Logistic Regression of Variables Associated with Postoperative Infection Among All Patients
95% CI = 95% confidence interval; kg = kilogram; ref = reference.
Increased Elixhauser Comorbidity Index was associated with a higher risk of postoperative infection (OR = 1.08, 95% CI = 1.05–1.11, p < 0.001). Other variables, including sex, age, BMI, preoperative antibiotic treatment, and pyuria, were not associated with postoperative infection.
Unplanned postoperative encounters
Unplanned encounters were reported for 165 (8%) patients in the MF cohort, 88 (6%) in the negative cohort, and 237 (16%) in the positive cohort (Fig. 2). These differences were significant on pairwise analysis. Positive culture patients presented to the ED significantly more (p < 0.001) in the postoperative period. Furthermore, relative to MF (p < 0.001) or negative cultures (p < 0.001), positive cultures required readmission more frequently. Between MF and negative cultures, neither emergency department visits (p = 0.069) nor readmission (p = 0.240) rates varied.
Risk factors for infection within the MF cohort
Within the MF cohort, multivariable logistic regression demonstrated a higher association of infection in patients with higher Elixhauser Comorbidity Indices (OR = 1.13, 95% CI = 1.07–1.19, p < 0.001, Table 3). Other variables, including gender, age, BMI, diabetes, preoperative stent/nephrostomy, preoperative antibiotic treatment, and pyuria, were not associated with postoperative infection in the MF cohort.
Multivariable Logistic Regression of Variables Associated with Postoperative Infection Within the Mixed Flora Cohort
95% CI = 95% confidence interval; kg = kilogram; ref = reference.
Discussion
In this single-institution retrospective study of more than 5000 patients who underwent ureteroscopy with laser lithotripsy, patients with preoperative MF cultures had a similar risk of postoperative infection compared with patients with preoperative negative cultures. Although patients in the MF cohort were more likely to receive preoperative antibiotics than patients in the negative cohort, they do not appear to be at increased risk of infection after adjusting for receipt of antibiotics. Conversely, patients in the MF cohort had a significantly lower infection risk than patients in the positive culture cohort. While we identified female gender and high Elixhauser Comorbidity Index as risk factors for infection in the MF cohort, preoperative antibiotic use was associated with increased infection risk and did not mitigate infections in the MF subgroup. This interesting finding may reflect preferential usage of empirical antibiotics in higher-risk patients, who are more susceptible to infection.
Postoperative infectious complications were reported in 9% of patients, similar to the 2% to 28% bounds reported in literature. 6,17,18 When controlling for other demographic and preoperative variables, the risk of infectious complications in patients with MF was similar to that in patients with negative cultures and lower than in patients with positive cultures. Also, the proportion of female patients was higher in the MF cohort, comparable with the positive culture cohorts. Theoretically, a higher incidence of postoperative infections would be expected in the MF group because of female dominance, but this was not visualized. These findings suggest that patients with MF cultures should be managed similarly to patients with negative cultures in the preoperative setting.
The presence of MF in preoperative urine cultures represents a significant challenge for urologists. A recent multicenter study asserted that MF cultures could independently nearly triple the odds of infectious complications. 19 However, interpreting MF as polymicrobial bacterial colonization may result in inappropriate overuse of antibiotics before surgery. Indeed, we visualized a higher rate of preoperative antibiotic use in the MF cohort relative to the negative cohort. However, physicians risk ignoring the presence of true bacteriuria in a potentially high-risk setting by dismissing these findings as specimen contamination. 20 This risk was highlighted in a retrospective study from Aix-Marseille University that demonstrated a higher risk of infection after ureteroscopy in patients with MF cultures. 21 Some physicians may opt to repeat MF cultures, potentially with catheterized samples, increasing the burden on the patient and laboratory.
MF urine cultures are highly prevalent, and efforts to decrease the rate of MF cultures through patient education have been largely unsuccessful. 22 –24 Therefore, it is essential to establish a standard approach to managing patients with these results. The interpretation of MF cultures as equivalent to negative cultures is supported by a study from our institution evaluating infection risk after urogynecologic surgery. 25 A systematic review of preoperative MF cultures by the Infectious Disease Committee of the French Association of Urology recommends that these cultures should be considered negative in most patients, but that antibiotic treatment should be considered in patients with pyuria, indwelling stent, or indwelling catheter. 26 In our study’s MF cohort, however, we did not find pyuria or indwelling stent/nephrostomy to be risk factors for infection. We also did not visualize an association between preoperative antibiotic use and postoperative infection in these supposed high-risk subgroups.
A surprising finding in our regression model was that preoperative stent or nephrostomy placement did not independently increase rates of postoperative infection. This differs from the conclusions of a recent meta-analysis suggesting that preoperative stent placement is associated with an increase in postoperative infection. 27 Yet, the stent or nephrostomy placement rate was significantly higher in the positive culture than in the MF cohort. The differences in stent usage and the disproportionate usage of antibiotics between subgroups may limit meaningful conclusions as to the association between indwelling stent and postoperative infection. An indwelling stent might be a risk factor as a foreign body susceptible to colonization or a surrogate marker for a prior infection that required stent placement. However, some patients benefit from preoperative stent placement, either by allowing drainage of upper tract bacteriuria or by facilitating placement of a ureteral access sheath, potentially decreasing infection risk via a lower intrarenal pressure. 28 The AUA guidelines strongly recommend against pre-stenting to enhance stone-free rates or reduce operative times. 29 We would not advocate for routine placement of stents before ureteroscopy unless there is a specific indication to do so.
In the analysis of preoperative urine cultures, it is essential to acknowledge the inherent limitations of these tests in guiding risk stratification and management. Bladder urine cultures have been shown to correlate poorly with stone cultures or upper urinary tract urine samples. 30 Obstructed patients may have negative cultures from the bladder despite an upper tract infection. Conversely, patients with lower urinary tract instrumentation or abnormal anatomy may have positive cultures from the bladder with a sterile upper urinary tract. Additionally, many patients with stones receive empirical antibiotics that may lead to falsely negative cultures. In all cases, preoperative urine culture should be considered within the clinical context. These limitations notwithstanding, preoperative urine cultures are repeatedly shown in the literature to be important in identifying high-risk patients. 27 This is highlighted by the high rate of infection, readmission, and intensive care in the positive culture cohort in our study.
Some limitations should be considered when interpreting results. This study is a retrospective investigation at a single institution. There may have been confounding variables that were not included in the analysis. Also, patients discharged with stents on strings are advised to retain them for 4 to 5 days before self-removing at home. Therefore, documentation on postoperative stent removal is limited. Prolonged indwelling stents may also be associated with postoperative infection. An absence of a standardized approach among all our clinicians is a limitation that in theory the statistical models account for. Routine post-stent urine cultures were not routinely obtained, which presents another limitation. Finally, there may have been patients who developed infections that were not recognized in this study, either because of the diagnosis codes used or because of patients presenting to other institutions. Despite these limitations, this study provides novel information regarding the risk assessment of patients with MF urine cultures prior to ureteroscopy. This information can guide urologists in the perioperative management of patients who present this common diagnostic dilemma.
Conclusions
While patients with MF in preoperative urine cultures were frequently given preoperative antibiotics, they were not at higher risk for postoperative infection relative to patients with negative cultures. Patients with MF cultures were at lower risk for infection than patients with positive cultures. Routine antibiotic use for patients with MF was not associated with a reduction in infectious complications after ureteroscopy.
Footnotes
Acknowledgements
Ethics Statement
This study received Institutional Review Board approval (IRB Pro00113540).
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.