
Abstract
Introduction:
While surgical intervention for benign prostatic obstruction (BPO) is traditionally recommended alongside bladder stone removal in males, recent studies have questioned the necessity of this approach. This study aims to evaluate the long-term outcomes of bladder stone removal without concomitant BPO surgery.
Methods:
We conducted a retrospective analysis of males with BPO who underwent bladder stone removal without concomitant BPO surgery in our institution between 2017 and 2024. Clinical and functional variables were collected, and our primary endpoint during the study period was future BPO surgery (BPO surgery-free survival). Secondary outcomes included BPO-related complications, medical therapy burden, and significant increase in post-void residual (PVR). Kaplan–Meier curves, receiver operating characteristic curves, and Cox regression models were used to analyze the results and identify predictors for future BPO surgery.
Results:
Our cohort consisted of 63 patients with median follow-up of 34 months. During the study period, 13 patients (22%) underwent BPO surgery. The 1-year, 3-year, and 5-year BPO surgery-free survival rates were 90%, 78%, and 78%, respectively. Prostate volume >100 cc and PVR >93 mL were the most significant predictors of future BPO surgery, increasing the likelihood by nearly fourfold. In the absence of concomitant BPO surgery, 94% of patients managed their BPO with medication, and 57% experienced BPO-related adverse outcomes.
Conclusion:
Bladder stone removal without concomitant BPO surgery offers a high likelihood of avoiding future BPO surgery in the intermediate-term. However, careful patient selection and management of BPO-related risks are crucial. Prostate volume and PVR should be considered in the shared decision-making process.
Introduction
Benign prostatic obstruction (BPO) is a prevalent cause of lower urinary tract symptoms in elderly men, often leading to the formation of bladder stones due to urinary stasis secondary to bladder outlet obstruction (BOO). 1,2 Bladder stones may originate from the kidneys and become trapped in the bladder because of obstructed outflow or may form directly in the bladder. 3,4 For patients with both bladder stones and BPO, advancements in endoscopic and minimally invasive surgical techniques have provided the possibility of treating both conditions simultaneously, 2 though these procedures carry risks such as bleeding, urinary incontinence, erectile dysfunction, and retrograde ejaculation. Medical management of BPO is varied, encompassing alpha-blockers, 5-alpha reductase inhibitors, β3 agonists, antimuscarinics, and phosphodiesterase-5 inhibitors, and offers an effective, noninvasive approach to treat BPO and prevent its complications. 5
There is ongoing debate regarding whether concomitant BPO surgery alongside bladder stone removal is essential to prevent the recurrence of bladder stone formation and to facilitate future stone expulsion. 6,7 Some studies have shown that cystolitholapaxy combined with medical therapy, without BPO surgery, can lead to significant symptoms improvement and resolution of bladder stones. 7 Therefore, this study aims to investigate the long-term postoperative outcomes in males following bladder stone removal without concomitant BPO surgery.
Methods
Study design
This is a retrospective study of patients who were treated by our service for bladder stones between August 2017 and June 2024. We reviewed electronic medical records and identified all patients who underwent bladder stone removal surgeries at our institution. The diagnosis of bladder stones was primarily based on imaging modalities (ultrasound, CT, KUB) or cystoscopy. For patients with a history of recurrent bladder stones, their first surgery for bladder stones with our service was considered for study purposes. All patients had at least one bladder stone over 1 cm according to our standard selection practice for treating bladder stones in the operative room, and all underwent transurethral or percutaneous endoscopic treatment. Exclusion criteria were established to ensure that the primary etiology of bladder stones was BOO secondary to BPO, and included: female patients, history of urinary diversion, history of bladder reconstruction surgery, neurogenic bladder, indwelling foreign bodies in the urinary system, history of radiation, and history of urethral or prostatic surgeries. Patients who underwent any concomitant bladder outlet procedures during the bladder stone removal surgery were also excluded.
After the procedure, if a catheter was placed, it was removed 0–3 days postoperatively, and patients were scheduled for a follow-up visit 1–2 months later. Stone analysis and metabolic evaluation were conducted, and patients received appropriate treatment based on the findings. Routine follow-up consisted of visits every 6–12 months, during which blood tests, urine analyses, post-void residual (PVR), uroflowmetry, and imaging studies (ultrasound, CT, KUB) were performed as deemed necessary.
We defined our primary endpoint as eventually undergoing a BPO surgery during the study period (BPO surgery-free survival). Secondary outcomes during the study period consisted of patients’ health outcomes compared with their preoperative baseline: 1 BPO-related complications including emergency department visits or hospitalizations due to hematuria, urinary tract infection, urinary retention, recurrence of bladder stones, or subacute creatinine increase of 33%–50%, 2,8 increase in BPO medication burden, and 3 significant PVR difference of more than 100 mL. 9 For the statistical analysis of endpoints and outcomes, the most recent follow-up data were used. Patients who were lost to follow-up or had insufficient data were excluded, or their outcomes were assessed based on the data available from their last follow-up visit.
Statistical analysis
After finalizing our cohort, we collected baseline and postoperative follow-up data, including demographics (age, body mass index), clinical and functional variables (medical history, prostate volume, creatinine levels, prostate-specific antigen (PSA), PVR, peak flow rate (Qmax), and stone characteristics (size, number, composition). Prostate volumes were documented from the results of ultrasound, CT, or MRI. PVR and Qmax were obtained from ultrasound and uroflowmetry studies. Stone size was recorded as the radiological diameter (in mm) of the largest stone, and composition was determined based on the main material identified in the stone analysis.
Categorical variables were described as frequencies and percentages, while continuous variables were expressed using medians and interquartile ranges (IQRs). A Kaplan–Meier curve was generated to depict BPO surgery-free survival, along with 1-, 3-, and 5-year rates. Receiver operating characteristic (ROC) curves were employed to evaluate the performance of continuous variables across various cutoff points for predicting future BPO surgery, with optimal cutoffs determined using the Kolmogorov–Smirnov test. Univariate and multivariate Cox regression models were utilized to assess the association between preoperative baseline characteristics and the likelihood of future BPO surgery, reporting hazard ratios (HRs) and 95% confidence intervals (95% CIs). Factors significant in univariate analysis and those known to influence BPO severity were included in the multivariate analysis. All statistical tests were two-sided, with significance set at p < 0.05. Statistical analyses were conducted using SPSS software (IBM SPSS Statistics, Version 29, IBM Corp., USA, 2022).
Results
The study cohort comprised 63 male patients with BPO who underwent bladder stone removal surgery at our institute, without concomitant outlet procedures and without exclusions based on our criteria (Fig. 1). Table 1 outlines the baseline characteristics of the patients, including clinical, functional, and stone-related variables. The median age was 69 years (IQR 63–74), and 71% of the patients were receiving at least one medication for BPO. The median prostate volume was 74 mL (IQR 50–106), and 33% had a history of previous bladder stone surgery. Data for PSA, PVR, and Qmax were missing for 25, 20, and 44 patients, respectively, with median values of 2.9 ng/dL (IQR 1.8–4.8), 45 mL (IQR 7–153), and 9 mL/sec (IQR 7–11), respectively. The majority of patients (63%) had multiple stones, with uric acid stones being the most common composition, accounting for 54% of cases. All patients underwent endoscopic surgery, 26% via transurethral approach and 74% via percutaneous approach. The median operative time was 45 minutes (IQR 33–64), and the 30-day complication rate was 25%, with all complications being minor (Clavien–Dindo grades 1–2). Minor complications included hematuria in three patients, persistent pain in three patients, urinary tract infection in one patient, temporary urinary retention in nine patients, prolonged urinary retention in one patient, and other minor complications in two patients.
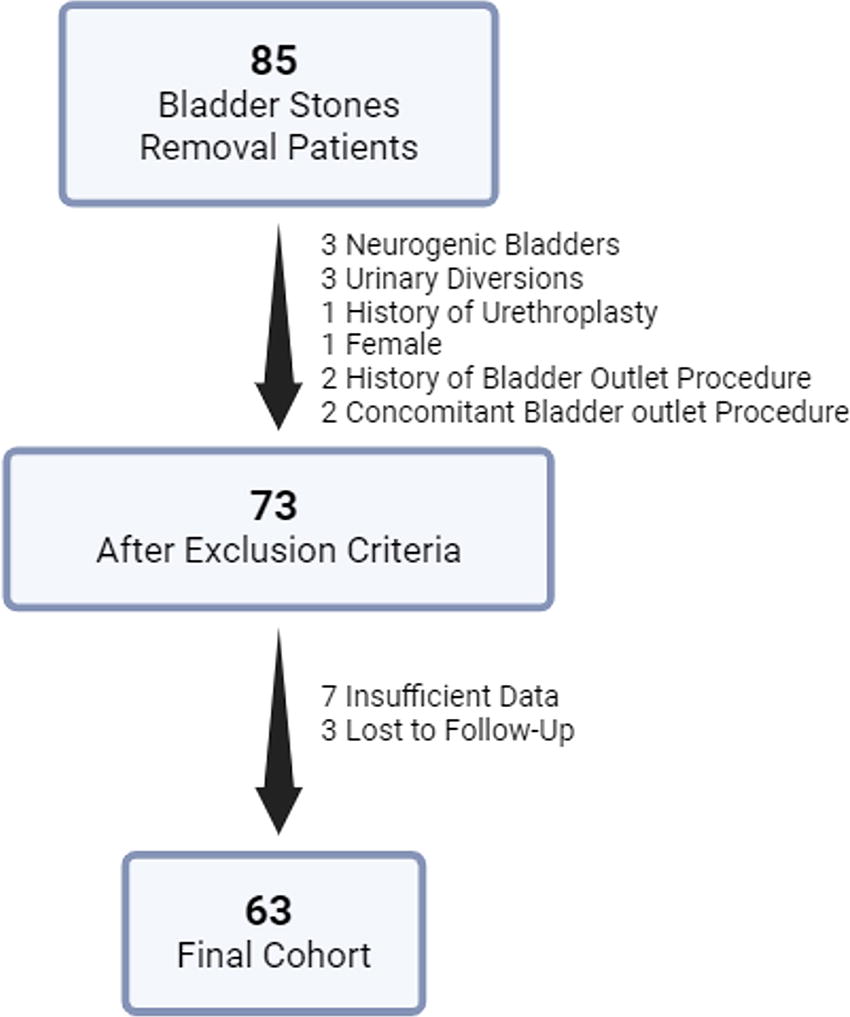
Study flowchart.
Patients’ Baseline Characteristics
5-ARI = 5 alpha reductase inhibitors; BMI = body mass index; BPH = benign prostatic hyperplasia; IQR = interquartile range; PSA = prostate specific antigen; PVR = post-void residual; Qmax = peak flow rate.
Over a median follow-up of 34 months (IQR 11–66), 13 patients eventually underwent BPO surgery, including transurethral prostate resection, holmium laser enucleation of prostate, Aquablation, and simple prostatectomy. Two patients were censored at the time of death, and two others were censored at the time of radical prostatectomy. The 1-year, 3-year, and 5-year BPO surgery-free survival rates were 90%, 78%, and 78%, respectively (Fig. 2), with a median time to BPO surgery of 24 months (IQR 7–31). ROC curve analysis for continuous variables identified prostate volume and PVR as the most promising predictors, with optimal cutoffs set at prostate volume >100 cc and preoperative PVR >93 mL (Fig. 3). Cox regression models revealed that a prostate volume >100 cc (HR = 3.47, 95% CI: 1.14–10.52, p = 0.03) and preoperative PVR >93 mL (HR = 3.82, 95% CI: 1.07–13.67, p = 0.04) were the most significant predictors for future BPO surgery. All other preoperative factors were not found to have a statistically significant association with the primary outcome, including age, BMI, creatinine levels, BPO medications, previous bladder stone surgery, PSA, multiple stones, stone burden, mode of access and main composition. In multivariate analysis, after adjusting for baseline characteristics, prostate volume >100 cc and preoperative PVR >93 mL remained the strongest predictive factors (Table 2).
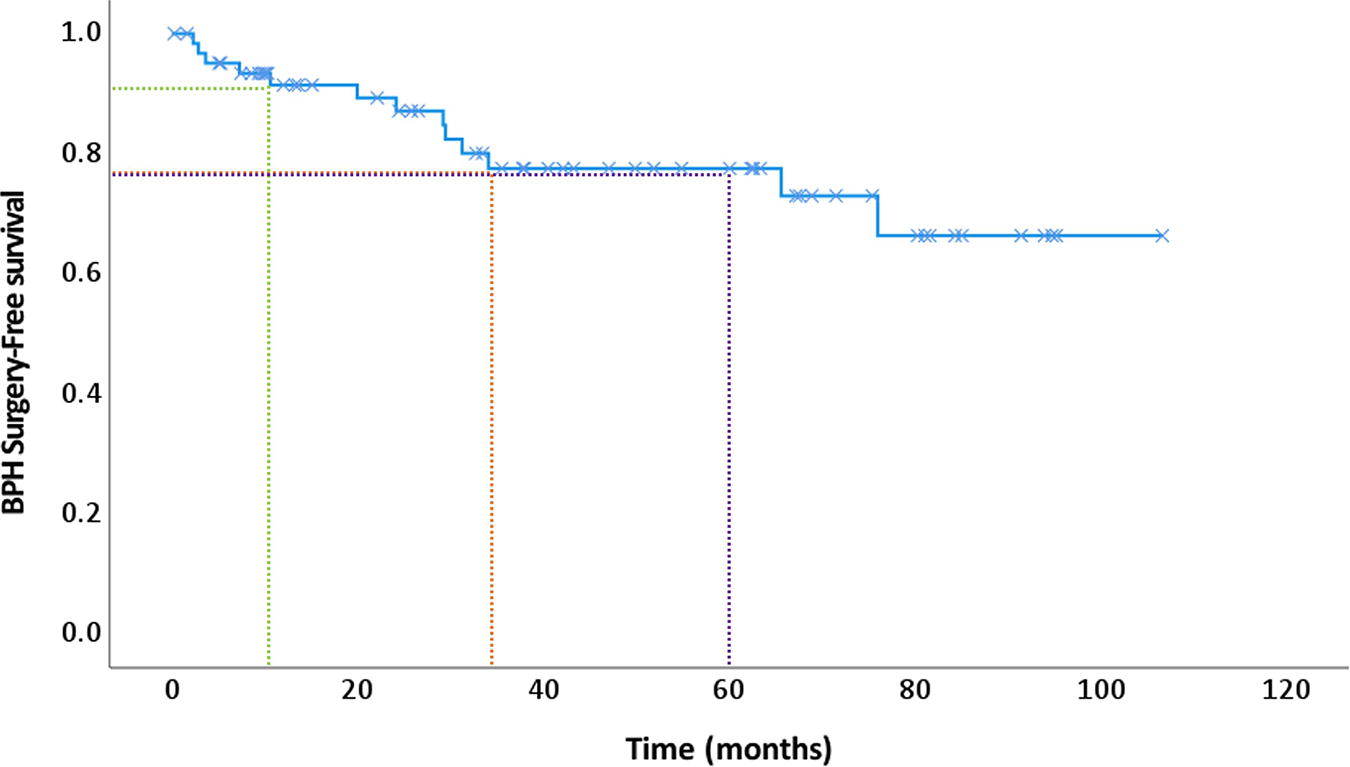
Kaplan–Meier curve for BPO surgery-free survival. Green, orange, and purple dashed lines represent 1 year, 3 years, and 5 years, respectively. BPO = benign prostatic obstruction.

Receiver operating characteristics curves of preoperative PVR and prostate volume for prediction of future BPO surgery. BPO = benign prostatic obstruction; PVR = post-void residual.
Univariable and Multivariable Cox-Regression Models for Future BPO Surgery
BMI = body mass index; BPO = benign prostatic obstruction; CI = confidence interval; HR = hazard ratio; PSA = prostatic specific antigen; PVR = post-void residual; Qmax = peak flow rate.
Overall, 36 patients (57%) experienced at least one secondary outcome during a median follow-up of 34 months. The rates of BPO complications, increased burden of BPO medications, and increase in PVR >100 mL were 35%, 32%, and 6%, respectively (Table 3). Among the 18 patients who were initially managed with watchful waiting and lifestyle modifications, 14 (78%) eventually began BPO medical therapy, leaving four patients (6% of the overall cohort) who remained untreated medically during the study period.
Secondary Outcomes
BPH = benign prostatic hyperplasia; ED = emergency department; PVR = post-void residual.
Discussion
Historical data suggest that BOO due to BPO is a major risk factor for the development of bladder stones, leading to the prevailing belief that managing bladder stones should always be accompanied by surgical treatment of BOO. 10,11 The presence of bladder stones in males with BPO has traditionally been considered an absolute indication for surgical management of the bladder outlet. However, over the past decade, the necessity of concomitant BPO surgery in patients with bladder stones has been questioned. In 2004, a study investigating urodynamic findings before and after the management of bladder stones found that only half of the patients exhibited urodynamic evidence of BOO. 12 In addition, Philippou et al. published a prospective study in 2011 that reported improvements in both objective and subjective outcomes following bladder stone removal alone, with a BPO surgery-free survival rate of 67%. 7 More recent literature remains controversial. Some studies suggest that bladder stones secondary to BPO do not always necessitate BPO surgery, with appropriate medical management potentially preventing surgery in 50% of patients. 13 Conversely, other studies have found that concomitant BPO surgery yields better clinical outcomes. 14
In our study, we observed that among males treated for bladder stones without concomitant BPO surgery, there is a low probability—approximately 20%—of requiring BPO surgery over an intermediate-term period of 3 years. The most predictive factors for future BPO surgery are prostate volume >100 cc and preoperative PVR >93 mL, both of which nearly quadruple the probability of future BPO surgery. Without BPO surgery, most males with bladder stones are managed chronically with medications (94% of the cohort) and experience some BPO-related adverse outcomes (57% of the cohort).
Previous studies have identified prostate volume and preoperative PVR as risk factors for future BPO surgery following bladder stone removal, 13,14 with suggested cutoffs at 54 cc and 190 mL, respectively. 13,14 More contemporary factors such as severity of intravesical prostatic protrusion (IPP) and pressure-flow studies has been associated with BOO severity and the likelihood of future BPO surgery. 13,15 Prostate volumes and PVRs, despite neither associated directly with nor reliable to predict the severity of BOO like other urodynamic variables (IPP, pressure-flow study), are associated with BPO clinical outcomes. Higher prostate volumes and PVRs are associated with more severe symptoms and higher rates of complications such as urinary retention, infections, hematuria, and recurrent bladder stones, all of which are indications for surgery. 16,17 Thus, we hypothesize that predicting adverse clinical outcomes is the key determinant for selecting bladder stone patients for surgery with no outlet procedure. These should all be discussed with patients as part of the shared decision-making process, including considerations for medication use and BPO-related complications.
The medical and surgical management of BPO has evolved in recent years, with growing evidence supporting the benefits of new drug combinations and surgical techniques. The AUA guidelines now encourage a shared decision-making approach and advocate for a trial of medical therapy. 18 This recent trend towards a more conservative approach in the management of BOO due to BPO may also indicate the need to revise the traditional indications for surgical treatment. We believe that much like other BPO complications such as first-time urinary retention, hematuria, and urinary tract infections, bladder stones can also be managed through the initiation or intensification of medical therapy, particularly in patients with favorable BPO characteristics.
The baseline characteristics of our cohort (median age of 69 years, median prostate volume of 74 cc, 33% with previous bladder stone surgery, and 71% on medical treatment) represent BPO patients with clinically significant disease, underscoring the reliability of our study in investigating genuine BPO cases. We believe that future prospective studies focusing on male populations with better clinical and functional BPO characteristics would yield improved BPO surgery-free survival rates and influence guidelines by identifying those who can be managed for their bladder stones without concomitant BPO surgery.
The limitations of our study are derived primarily from its retrospective, single-center, and observational design. We lacked data on the specific causes of BPO surgeries and had insufficient information regarding subjective symptoms, such as IPSS. We also lacked the preoperative PVR and Qmax values in 32% and 70% of our cohort, respectively. In addition, for most of our patients, we did not have urodynamic data such as pressure-flow studies or IPP measurements, which are more contemporary and reliable for confirming and grading BOO. However, this is a “real-world” study with objective outcomes that are not subject to recall or selection biases, making it highly relevant for clinical practice. We are aware of the study limitations, preventing it from being practice-changing. It should trigger further larger prospective studies that may reinforce our results.
Conclusion
Bladder stones can be removed in males with BPO without a concomitant outlet procedure, offering a high intermediate-term probability of avoiding future BPO surgery. However, this approach may necessitate ongoing medical therapy and carries the risk of potential BPO-related adverse events. Prostate volume (>100 cc) and PVR (>93 mL), both of which are associated with the severity of BOO, may serve as predictors for future BPO surgery. These considerations should be thoroughly discussed with patients as part of the shared decision-making process.”
Footnotes
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to ethical issues and the privacy of the participants.
Ethics of Approval Statement
Ethical approval to report this study was obtained from our institutional review board.
Authors’ Contributions
Z.S., K.G., W.M.A., M.G.: Conception and design. Z.S., L.D.R., E.F., B.G.: Acquisition of data. Z.S., V.D.: Statistical analysis. Z.S., K.G., M.G.: Analysis and interpretation. Z.S., L.D.R., E.F.: Drafting of the manuscript. W.M.A., M.G.: Critical revision of the manuscript. M.G: Supervision.
Author Disclosure Statement
All authors have nothing to disclose.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.