
Abstract
Purpose:
Although the reported incidence of ureteral strictures following ureteroscopy (URS) is low (0.3%–3%), we hypothesize the risk may rise as the depth of ureteral injury increases.
Materials and Methods:
Between 2018 and 2022, 550 patients underwent URS for upper tract calculi; each of these patients had a postureteroscopic lesion scale (PULS) grading and follow-up imaging 3–6 months after a surgical procedure. Patients with preexisting strictures, or strictures formed at the site of an impacted stone, were excluded.
Results:
With a median follow-up of 23 months, de novo stricture rates for the 550 patients were 0.73% (4/550). More specifically, while strictures among patients with PULS 0 and 1 were minimal, 0% (0/235) and 0.48% (1/208), respectively. However, the stricture rate increased to 1.1% (1/92) for PULS 2 and jumped to 13.3% (2/15) among those patients with PULS 3 injuries. On a Firth penalized logistic regression analysis, we found that when urothelial splitting (i.e., PULS 2 or higher) or periureteral fat (i.e., a PULS 3 transmural injury) was visualized, the odds of developing a stricture were 13 and 40 times higher, respectively. Based on these findings, we sought to simplify the existing ureteral injury grades and improve ureteral stricture prognostication by creating a novel dichotomous injury scale.
Conclusions:
Iatrogenic ureteral stricture rates rose sharply when ureteral wall integrity was disrupted. This was most notable for a transmural injury, which resulted in a stricture rate of 13.3% (2/15 patients). Using a simplified two-stage scoring system (University of California, Irvine [UCI] 0, 1, or 2), clinicians may be better able to identify patients (i.e., UCI 2) at high risk for post-URS stricture formation.
Introduction
The global rise in nephrolithiasis has coincided with notable advances in treatment, positioning ureteroscopy (URS) as a leading minimally invasive approach for stone disease. 1 –3 Although URS has a lower complication profile compared with percutaneous stone removal, concerns over postoperative ureteral strictures persist. Although the reported cumulative stricture rate following URS is 0.3%–3%, we hypothesize that this risk may be higher when stratified by the postureteroscopic lesion scale (PULS) grades, which range from 0 (no visible injury) to 3 (transmural tear with periureteral fat noted).
To evaluate post-URS ureteral wall injury, the following two scales have been proposed: the Traxer ureteral injury scale (TUIS: grades 0–4) and PULS (grades 0–5) (Table 1). 4 –6 The main distinction between these scales lies in their classification of high-grade lesions. 4 –6 In the PULS system, injuries involving the submucosa are categorized as low-grade, whereas the TUIS considers these same injuries high grade, although both classify the injury as grade 2. 4 –6
The clinical significance of post-URS stricture formation has yet to be assessed based on specific PULS or TUIS grades. This is critical given the inconsistent application of these grading systems across institutions and the variations in defining “high-grade” injury. Therefore, our study aims to determine ureteral stricture rates across ascending grades of injury at a single, high-volume center that routinely uses the PULS system.
Side-by-Side Comparison of the Most Commonly Used Ureteral Injury Systems, the Postureteroscopic Lesion Scale, and the Traxer Ureteral Injury Scale
 Mucosa;
Mucosa;  Muscularis;
Muscularis;  Lamina propria;
Lamina propria;  Adventitia
Adventitia
Materials and Methods
The University of California, Irvine (UCI) Institutional Review Board approved a REDCap database for patients undergoing a minimally invasive procedure for urolithiasis. Patients who underwent flexible URS (fURS) for upper tract urinary calculi between 2018 and 2022 were prospectively enrolled. Four attending endourologists, all routinely using the PULS grading system, participated in this study. Intraoperative data, including patient demographics, surgical laterality, ureteral access sheath (UAS) specifications, laser settings, and scope type, were recorded. Following fURS, a flexible digital ureteroscope was used to inspect the ureter, and observed lesions were graded using the PULS system.
A retrospective review of our prospectively collected database assessed the long-term risk of de novo ureteral stricture formation post-URS. Stricture formation was defined on follow-up imaging 3–6 months after a surgical procedure by one or more of the following: new hydronephrosis on CT or ultrasound (US), a postoperative nuclear medicine scan with a T 1/2 >20 minutes, and/or endoscopic evidence of a de novo ureteral stricture distant from the original stone site during a subsequent ipsilateral procedure. Patients with suspected strictures on US or nuclear scans were further evaluated with noncontrast CT to confirm the diagnosis. Patients were excluded if they had preexisting strictures, strictures at the site of a previously treated impacted stone, or a history of endoureterotomy or balloon dilation.
Data analysis was performed using IBM SPSS Version 29.9 (IBM Corp, Armonk, NY) and R Version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria). Normal distribution of continuous variables was assessed using the Kolmogorov–Smirnov test. Data were described as mean (standard deviation) for normally distributed data and median (interquartile ranges) for non-normal distributions. Paired or unpaired t-tests were used for comparisons. Categorical variables were expressed as percentages, with chi-square testing used to examine associations between variables and outcomes.
Because of the rarity of ureteral strictures following URS, small-sample bias could complicate the analysis of binary variables using standard logistic regression models. This introduces the potential for complete/perfect separation to occur, where a covariate either consistently aligns with or rarely corresponds to the binary outcome. Given the low-event rates of ureteral strictures, to minimize the coefficient estimate’s bias, a penalized Firth’s logistic regression model was employed. This approach allowed for a robust analysis of minor urothelial splitting vs complete ureteral tears with periureteral fat, and their respective roles in stricture formation. 7
Results
Among 684 patients undergoing urolithiasis-related fURS at our institution between January 2018 and December 2022, 550 had a follow-up US or CT scan within 3–6 months postprocedure. Among these patients, 54% (298/550) were male, 28% were presented before an operation (156/550), and a UAS was used in 76% (417/550) of cases. Laser settings varied across cases, with both thulium and holmium lasers being used (Table 2).
Baseline Characteristics of the Studied Population
IQR = interquartile range; UAS = ureteral access sheath.
Among these 550 patients, ureteral inspection at the end of the procedure revealed the following: 235 (42.7%) PULS grade 0, 208 (37.8%) PULS grade 1, 92 (16.7%) PULS grade 2, and 15 (2.7%) PULS grade 3. There were no PULS grade 4 or 5 injuries. In the TUIS system, the PULS grade would be similar to grade 0, 1, 2, or 3 lesions in 235 (42.7%), 208 (37.8%), 92 (16.7%), and 15 (2.7%) patients, respectively.
De novo ureteral stricture rates were stratified by PULS grades. No strictures were observed in patients with PULS 0 (0/235), whereas PULS 1 had a stricture rate of 0.48% (1/208), and grade 2 had a rate of 1.1% (1/92). In contrast, PULS 3 had a markedly higher stricture rate of 13.3% (2/15). Strictures occurring at the stone or laser activity sites were excluded from the analysis. None of the four identified strictures had calcifications at the stricture site. All de novo strictures were managed endoscopically: one patient only had an endopyelotomy stent placed, two patients underwent balloon dilation with the placement of an endopyelotomy stent, and one underwent laser endoureterotomy. Importantly, none of the balloons used was coated with paclitaxel or any other agent that could potentially affect healing at the site of the stricture. At a median follow-up of 23 months, three out of four patients had complete resolution of hydronephrosis and normalization of renal function. However, one patient did not achieve resolution and is currently managed with a yearly indwelling Resonance stent, having declined ureteroplasty.
A two-tailed unpaired-sample t-test revealed no statistically significant difference in operative time between patients who developed postoperative strictures and those who did not (142.7 ± 81.3 minutes vs 148.9 ± 84.7 minutes, p = 0.4253). Among the four patients with de novo strictures, two were presented and two were not. None of the four patients had CT evidence of stone fragments in the bed of the stricture.
Strictures were found to be more frequent in the PULS 3 subgroup, compared with the PULS 0 (13.3% vs 0%, p < 0.0001), PULS 1 (13.3% vs 0.48%, p < 0.0001), and PULS 2 (13.3% vs 1.1%, p = 0.008) subgroups. No statistically significant differences were noted between the stricture rates of PULS 1 and PULS 0 subgroups (p = 0.288). In addition, there was no statistically significant difference in stricture occurrence between PULS 2 vs PULS 1 or PULS 0 (p = 0.552, p = 0.1101, respectively); however, PULS 3 had a statistically significant higher rate of ureteral stricture when compared with PULS 0, 1, and 2 (p = 0.0001, p = 0.0001, p = 0.008, respectively) (Table 3).
Head-to-Head Comparison of Ureteral Stricture Rates Across Ascending Grades of Ureteral Wall Injury
All p-values resulted from two-tailed chi-square testing. Blue tabs indicate statistical significance.
Firth’s penalized logistic regression analysis revealed that the presence of urothelial splitting (PULS 2 or higher, TUIS 2 or higher) increased the odds of ureteral stricture formation by 13-fold (p = 0.028) (Table 4). Furthermore, visualization of periureteral fat (i.e., PULS 3, TUIS grade 3) was associated with a 40-fold increase in the odds of developing a ureteral stricture (p = 0.0002) (Table 4).
Evaluation of the Likelihood of Developing a Ureteral Stricture Based on Two Intraoperative Binary Parameters, as Assessed by Multiple Penalized Logistic Regression Models (i.e., Intact Urothelium vs a Tear in the Urothelium (Partial Tear vs Complete Tear)
CI = confidence interval; OR = odds ratio.
Discussion
De novo ureteral stricture rates following URS are rare, ranging from 0.3% to 3%. 8–9 This low rate of post-URS strictures has been interpreted by some as showing that even transmural ureteral tears have a sanguine outcome. The present analysis takes exception to this stance; indeed, in our review, a transmural ureteral tear increased the likelihood of stricture formation 40-fold, with an incidence of 13.3%. Moreover, we would like to emphasize that although the rate of 16 Fr UAS size use in our study was higher (41.2%) compared with the general endourologic community (2.7%), our observed stricture rates were not significantly higher than those previously reported in the literature (0.77%, 4/550). 8
Ureteral strictures are often difficult to resolve without a formal surgical repair. Indeed, nearly half of cases managed with endoscopic intervention fail, and in one series, 37.5% of patients ultimately required a reconstructive surgical procedure. 9,10 Early diagnosis is critical, as much as 25% of patients with post-URS strictures eventually require nephrectomy. In our series, one of four patients with a post-URS stricture now requires a permanent indwelling Resonance stent and has experienced a reduction in ipsilateral renal function (11%), highlighting the importance of early detection and timely intervention in managing ureteral strictures.
Interestingly, the clinical relevance of the PULS and TUIS classifications has been addressed in only one study by Stern and colleagues, which followed 56 patients with high-grade injuries (TUIS grade 2 or higher) caused by the passage of a 14 Fr UAS over 3 years, using US and CT scans. 11 They reported just one de novo stricture (1.80%). In contrast, our cohort noted three novel strictures in the high-grade (PULS 2 and 3) injury group (2.80%). The 95% confidence interval (CI) (−0.07%–0.05%) for the difference in stricture rates between the study by Stern et al. and ours does not indicate a statistically significant difference. Notably, Stern’s study did not examine stricture rates in patients with low-grade injuries, a limitation gap addressed in our study, which includes a large cohort of PULS 0 (235 patients) and PULS 1 (208 patients).
In our review of PULS lesions among 550 patients, there was a statistically significant association between the depth of injury and the subsequent risk of stricture formation. The risk grew exponentially with the depth of the injury, ranging from 0.48% in those with only minor urothelial layer involvement (PULS 1) to 1.1% in patients with a trans-urothelial, submucosal injury (PULS 2), and then escalating to 13.3% when the injury was transmural (PULS 3).
Although we find the PULS and TUIS grading systems useful for guiding stent duration and the timing of repeat URS, their practical application presents certain challenges. The classification of injuries often relies on subtle distinctions that can vary with the surgeon’s experience and thoroughness. Moreover, the labor of evaluating injuries or removing instruments can exasperate the injury, adding further complexity. Given the delicate nature of the ureter, particularly in the upper part where its wall thickness may be less than 2 mm, differentiating minor injury depths offers limited clinical value when significant damage is present. 12 Focusing on such nuances may detract from a simpler evaluation, where a binary classification system would provide clearer guidance for treatment. Therefore, we propose a two-tier, binary approach for assessing the ureter post-URS (Fig. 1).
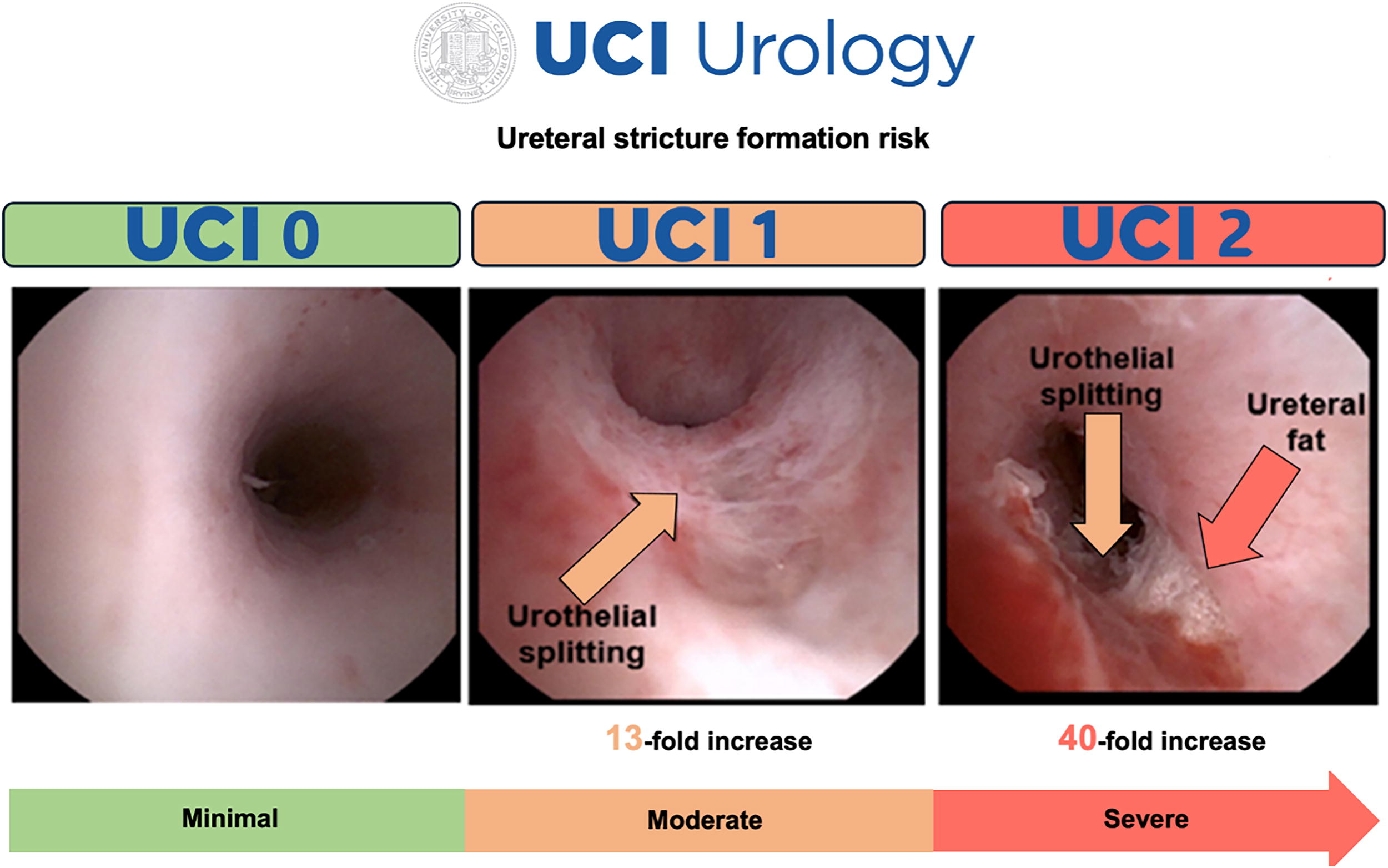
Endoscopic representation of the proposed alternative two-tier system for assessment of postureteroscopic injury. The first criterion is the presence or absence of urothelial splitting (orange arrows). The second criterion is differentiating between minor urothelial splitting (i.e., mucosal lesion into the submucosa, or muscularis)—UCI 1 and complete splitting of the ureteral wall with visualization of periadventitial ureteral wall fat (yellow arrow) (i.e., PULS grade 3 or higher; TUIS grade 3 or higher)-UCI 2. PULS = postureteroscopic lesion scale; TUIS = Traxer ureteral injury scale; UCI = University of California, Irvine.
Specifically, only two key questions need to be answered as follows: (1) Is there any injury to the ureteral wall and (2) if so, is periureteral fat visualized? Injuries are classified as simple urothelial splitting (UCI 1) or transmural with fat present (UCI 2). Urothelial splitting increases the odds of a postoperative stricture by 13-fold (95% CI: 1.320–124.549), whereas transmural injuries with fat (PULS 3 or TUIS 3) raise the risk 40-fold (95% CI: 5.274–309.265). Of note, although the penalized logistic regression model minimizes the impact of low-outcome prevalence on coefficient outputs, the CIs remain wide because of the persistent degree of uncertainty. Nonetheless, even in the most conservative scenario, considering only the lower bounds of the 95% CI for the odds ratios, superficial urothelial splitting (UCI 1) or visualization of periureteral fat (UCI 2) significantly increases the risk of stricture by 32% and 427%, respectively. When using the proposed binary UCI system among our 550 patients, 107 (19.45%) had urothelial splitting, with 15 (2.72%) sustaining a transmural injury revealing periureteral fat. This simplified approach reduces subjective variability, enabling clinicians to more consistently assess and manage ureteral injuries while complementing traditional grading systems and aiding in decisions regarding stenting and definitive treatment strategies.
Unfortunately, at present, at many centers, post-URS ureteral wall assessment is not routinely recorded. 4 We contend that adopting a simplified, dichotomous system with only three scores (i.e., UCI 0, UCI 1, and UCI 2), focusing less on nuanced differences between grades and ureteral layers, would assist surgeons in formulating more informed and effective follow-up care plans, particularly given the escalating risk of strictures when there is a transmural urothelial tear (UCI 2). Hopefully, the proposed simplified system would encourage more urologists to assess ureteral integrity at the termination of each URS procedure and thus lead to judicious stenting and follow-up imaging.
Management of higher grade post-URS ureteral injuries remains largely anecdotal. For patients with low-grade injuries (PULS 1—affecting only the mucosa), we and others recommend leaving a ureteral stent in place for at least a week. As shown in our study, this approach results in an extremely low stricture rate (<0.5%), allowing us to group PULS 0 and PULS 1 into a single category, UCI 0. 4,6 In contrast, patients sustaining a high-grade ureteral injury, characterized by urothelial splitting (UCI 1) and/or periureteral fat visualization (UCI 2), may require a stent for a longer duration, between 3 and 6 weeks. 4,6 This suggested time line aligns with the recommendations of both Schoentlaer et al. and Traxer et al. 4,6 ; however, the benefit of long-term vs short-term stent duration among patients with a higher grade injury is yet to be documented. Regardless of stent duration, imaging follow-up after stent removal is essential, initially within a few weeks and again after several months, to detect silent obstruction. Less vigorous and inadequate follow-up may risk partial or complete kidney function loss, as noted by others. 13
Limitations to the present study largely derive from its retrospective nature as well as the small number of affected cases. First, this study is observational, and the grading of ureteral lesions may well have varied among the four endourologists who entered patients into the study. Second, among all surgeons, the PULS grading is subjective and is often determined only by the attending surgeon, rather than by a consensus of those observing the URS inspection at the end of the procedure. Third, the method of examination at the end of a procedure may vary significantly among surgeons, with some being perhaps more cursory than others. Nonetheless, in this regard, it is worth noting that although a PULS 2 injury and the identification of the extremely thin ureteral muscle may be subtle (i.e., UCI 1), the presence of a PULS 3 injury (i.e., UCI 2), in which the split in the urothelium reveals the glimmering, gossamer of golden periureteral fat, is unmistakably obvious.
Conclusion
Post-URS, ureteral wall integrity plays a crucial role in the development of postoperative ureteral strictures. The risk rises exponentially with the depth of injury, ranging from 0%–0.48% in those with no/minimal ureteral wall lesions (i.e., UCI 0) to 1.1% for a superficial split in the urothelium (i.e., UCI 1) to 13% when a full-thickness transmural injury (i.e., UCI 2) of the ureter occurs. The current four- and five-tier grading systems are somewhat cumbersome and complex, making comparisons across institutions and practitioners nuanced and difficult; in this regard, a simpler binary system is proposed that poses only the following two questions: (1) Is the urothelium intact (UCI 0) or not (UCI 1) at the end of the procedure and (2) if the urothelium is not intact, is it superficial (UCI 1) or deep with periureteral fat (UCI 2) visualized?
Advancing Practice
De novo stricture rates following URS are rare, ranging from 0.3% to 3% in the literature. This low rate of post-URS strictures has been interpreted by some as showing that even transmural tears have a sanguine outcome. In contradistinction, our findings suggest that ureteral stricture risk rises exponentially with the depth of injury. We found that when superficial urothelial splitting occurred or when a transmural injury exposing periureteral fat was visualized, the odds of developing a de novo stricture rose by 13 times and 40 times, respectively.
Patient Summary
In this study, we looked at the long-term effects of injuries to the ureter (the tube that carries urine from the kidney to the bladder) after a ureteral or kidney stone treatment, which involved the use of a flexible visualizing instrument to view the ureter and the stone. This instrument is passed via the urethra, across the bladder, and directly into the opening of the ureter to access the stone. We found that deeper injuries to the ureter associated with passage of the visualizing instrument or from placement of an accessory access sheath were linked to a higher risk of developing a postoperative blockage of the ureter, known as a ureteral stricture. As such, for those individuals who incur these deeper injuries at the time of operation, early and repeat monitoring by radiologic imaging is indicated in order to expeditiously diagnose the development of a ureteral stricture so that it can be treated before any damage to the function of the kidney occurs.
Footnotes
Take Home Message
Ureteral stricture risk rises exponentially with the depth of the ureteral injury. Indeed, when superficial or transmural ureteral splitting occurred, the odds of developing a de novo stricture rose by 13- and 40-fold, respectively.
Authors’ Contributions
The authors confirm their roles and contributions to the article as outlined: Study conception and methodology: A.D.C., S.A.M.L., and R.V.C. Data collection: A.D.C., J.A.-V., S.A.M.L., S.S., J.C.T., and B.C. Data curation: A.D.C., J.A.-V., S.A.M.L., S.S., J.C.T., and B.C. Formal analysis: A.D.C., J.M.L., and M.E. Article preparation and review: all authors. Critical article revision: A.D.C., S.A.M.L., B.M.G., Z.E.T., P.J., R.M.P., J.L., and R.V.C. Each author conducted a review of the results and granted their approval for article submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No external grant funding was provided for the completion of any subparts of this study. Internally funded through the Curiosity and Innovation Lab Fund.