
Abstract
Background:
At present, there is a lack of cohort studies on robot-assisted laparoscopic pyeloplasty (RALP) for the treatment of ureteropelvic junction obstruction (UPJO) in infants under 3 months of age. This study aims to enhance the understanding of the safety and efficacy of RALP in this specific infant population.
Methods:
We retrospectively analyzed the clinical data of children with UPJO who underwent unilateral pyeloplasty at our center from January 2019 to June 2022. We categorized the children based on their ages: those younger than 3 months old comprised the RA group (25 cases), whereas those aged 3 months to 3 years old formed the RB group (25 cases). We collected and statistically analyzed the baseline data, perioperative details, postoperative complications, and the recovery of split renal function (SRF) along with the improvement in hydronephrosis for both patient groups.
Result:
Both age groups successfully underwent the operation without requiring conversion to open surgery. There were no significant differences observed in the operation time or postoperative hospitalization duration between the two groups (P > 0.05). Following surgery, both groups showed significant improvements in anteroposterior diameter (APD) and SRF (P < 0.05). However, there was no significant discrepancy noted in the recovery of APD and SRF between the two groups postoperatively (P > 0.05). Additionally, there were no significant variations in postoperative complications between the two groups (P > 0.05).
Conclusion:
Given the mature and stable nature of the surgical technique, RALP proves effective in treating UPJO in infants younger than 3 months, yielding favorable therapeutic outcomes.
Introduction
Congenital hydronephrosis is characterized by the enlargement of the renal collecting system in the fetus. It affects approximately 1 in 1500 newborns. The condition has various causes, with ureteropelvic junction obstruction (UPJO) being the most common in children. 1 Among the surgical interventions for UPJO, Anderson–Hynes pyeloplasty is widely recognized as the established procedure for UPJO. 2
With the advancement and refinement of minimally invasive techniques, the introduction of robot-assisted laparoscopic pyeloplasty (RALP) has truly transformed the field. RALP not only offers a minimally invasive approach but also facilitates precise anatomical procedures, 3–4 demonstrating a success rate comparable to open surgery in infants under 1 year old. 5–6 However, the average age of infants in these studies typically exceeds 3 months. Challenges arise when dealing with infants under 3 months with UPJO, including poor surgical tolerance, limited abdominal space, reduced ureteral volume, and potential postoperative complications such as anastomotic leakage and stenosis. Consequently, the feasibility of early surgical intervention in this particular age group remains a topic of ongoing debate.
To determine whether RALP can effectively address these challenges and achieve outcomes comparable with older children or adults, further investigation is necessary. It is crucial to explore whether the inherent advantages of RALP can be harnessed in the treatment of UPJO in infants under 3 months of age. This research will shed light on the potential benefits and limitations of RALP in this specific population.
Materials and Methods
The clinical data of UPJO patients who underwent unilateral pyeloplasty in the Department of Pediatric Surgery at the First Affiliated Hospital of Guangxi Medical University from January 2019 to June 2022 were analyzed retrospectively. The inclusion criteria of the cases were as follows: (1) initial surgery on the affected side. (2) Preoperative imaging (magnetic resonance imaging, ultrasound, and computed tomography) confirms the diagnosis of UPJO. (3) All children met at least one of the criteria for EAU surgery 1 : grade III and IV dilatation as defined by the Society for Fetal Urology (SFU); impaired split renal function (SRF) <40% and (time required for the radioactive tracer to be excreted from the kidneys by half) T1/2 >20 minutes; progressive deterioration in renal function, characterized by a decline of more than 10% in SRF during follow-up; progressive deterioration of hydronephrosis (and hydrops up to SFU Grade III) and manifestation of hydronephrosis symptoms (such as pain, recurrent urinary tract infections [UTIs], hematuria, and calculi). (4) Postoperative pathology confirmed that hydronephrosis was caused by UPJO. Exclusion criteria were as follows: (1) secondary surgery, (2) bilateral hydronephrosis combined with distal obstruction or other malformation, and (3) clinical data are incomplete, and the follow-up duration is <12 months.
This study involved a total of 50 pediatric cases, divided into 2 groups. Group RALP A (RA group) consisted of 25 infants under 3 months old, whereas Group RALP B (RB group) comprised 25 children aged 3 months to 3 years. Various baseline data were collected for both groups, including age, weight, height, sex, affected side, surgical duration, postoperative hospital stay, and complications.
All cases were followed up for a minimum of 12 months. The anteroposterior diameter (APD) of the renal pelvis was measured using ultrasound before and after surgery. Additionally, a diuretic renogram was performed to assess the SRF of the affected kidney, along with other serum renal function indicators.
This study received approval from the hospital ethics committee, and informed consent was obtained from the families of the patients (approval number: 2024-E222-01).
Surgical procedure
In our procedures, we employ the Da Vinci Xi surgical system® (Intuitive Surgical, CA, USA), utilizing three key instruments: the Micro Bipolar Forceps, Monopolar Curved Scissors, and the Mega SutureCut Needle Driver.
Surgical position
The child is positioned in the lateral decubitus on the healthy side, inclined at approximately 60 to 80. The upper limb on the affected side hangs naturally, whereas the upper limb on the unaffected side is abducted and supported by a hand support plate. The lower limb on the affected side is slightly bent backward, and the lower limb on the unaffected side is flexed downward (see Fig. 1a).
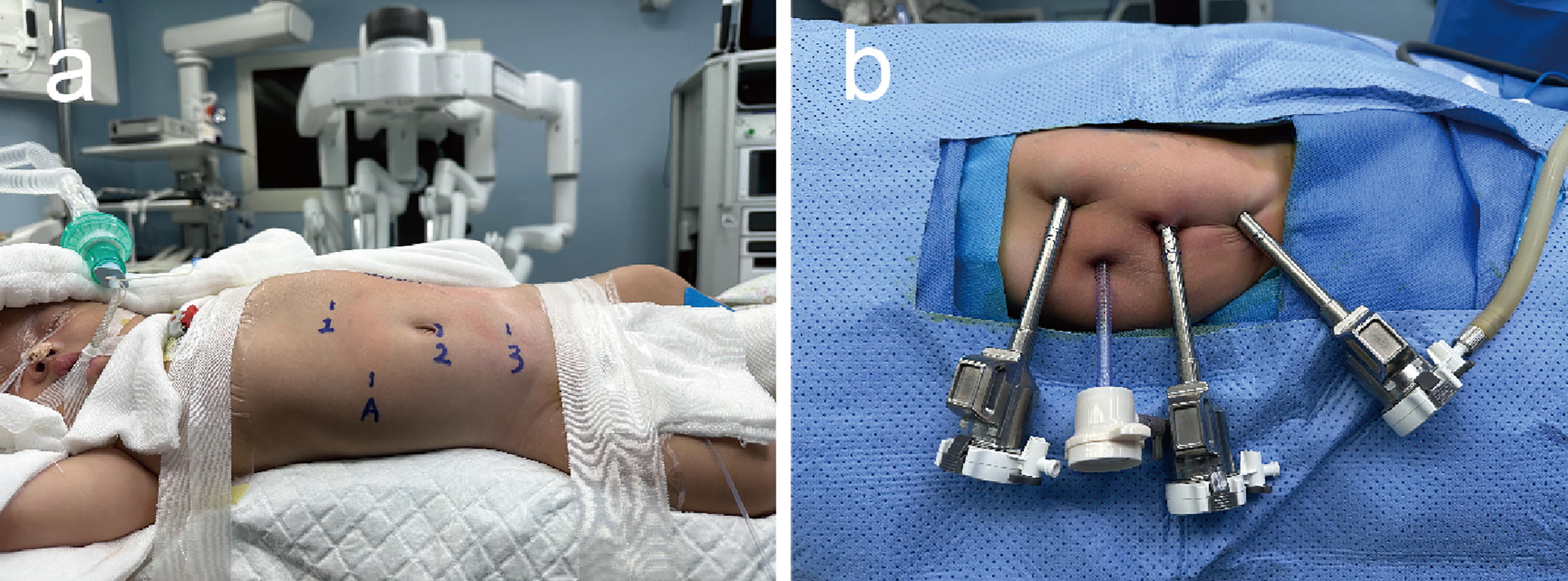
A male infant, 48 days old, has been diagnosed with left-sided UPJO.
Establishment of operation channel
An incision was made at the lower edge of the umbilicus, and an 8 mm Trocar was inserted to create an aperture for lens insertion. A pneumoperitoneum was established and maintained at 7 to 9 mmHg. Two 8 mm channels were created: one positioned below the xiphoid process parallel to the umbilicus (Robot Arm 1) and another above the pubic symphysis parallel to the umbilicus (Robot Arm 3). The distances between these channels and the lens insertion site were consistently ≥4 cm. Additionally, a 5 mm auxiliary channel was established between Arm 1 and Arm 2. Each Trocar was inserted approximately 0.5 cm deep into the abdominal cavity and securely fixed to prevent displacement during the procedure (see Fig. 1b).
Microscopic operation
The lateral peritoneum was incised along the paracolic gutter on the affected side, the colon was mobilize medially, and the perirenal fat sac was dissected. Perirenal adhesions were released to fully expose the renal pelvis and upper ureter, clearly identifying the stenotic site at the ureteropelvic junction.
Pyeloplasty operation: (1) Incision and dissection: The renal pelvis wall was incised about 0.5 cm outside the renal parenchyma, excising the dilated portion while preserving a small tongue-like valve. The distal ureter was partially incised at the stricture, leaving the proximal ureter intact. Longitudinal dissection of the ureter’s lateral border by 1 cm was performed for anastomosis; (2) Alignment and suturing: The nadir of the renal pelvis was identified based on renal axis alignment. The lowest point of the renal pelvis to the ureter was sutured using a 6-0 Vicryl suture. The ureter to the posterior wall of the tongue-like valve was sutured intermittently, typically requiring 6 to 8 stitches; (3) Ureteral stenting: A ureteral stent was inserted into the distal ureter through the anastomotic opening, with the distal end in the bladder and the proximal end in the renal pelvis; (4) Final suturing: A 6-0 Vicryl suture was used to intermittently suture the anterior wall of the renal pelvis and continuously suture both sides, completing the pyeloplasty (see Fig. 2 and the surgical video).

RALP surgical steps illustration.
Postoperative complications and management after RALP
Complications following RALP may include UTIs, hemorrhaging, ureteral stent clogged, anastomotic fistula, and anastomotic stenosis. The postoperative treatment protocol is as follows: postoperative pain assessment and management: The FLACC (Face, Legs, Activity, Cry, Consolability) scale is used to assess pain levels. Pain relief includes comforting through sucking or maternal soothing, with oral acetaminophen administered as needed. (2) Antibiotic prophylaxis: Empirical antibiotics were administered for 3–5 days. For patients with UTIs, antibiotic treatment was extended, and urine cultures were performed. An abdominal X-ray (KUB) was conducted on the third postoperative day to confirm the position of the ureteral stent. (3) Catheter management: The urinary catheter was removed between the fourth and sixth postoperative days. The drainage tube should be removed once drainage is consistently below 10 mL for three consecutive days. (4) Discharge criteria: Patients may be discharged when they have smooth urination, no fever, abdominal pain, dysuria, hematuria, or other discomforts, and satisfactory incision healing. (5) Stent removal: Cystoscopy will be performed 4 to 6 weeks postsurgery to remove the ureteral stent. (6) Follow-up schedule: Regular outpatient follow-ups will occur in the first year at 1, 3, 6, 9, and 12 months, followed by every 6 months thereafter. Follow-up assessments will include blood biochemistry, urine analysis, urinary system ultrasound, and diuretic renogram. Specifically, the results of ultrasound and diuretic renogram conducted at the 6-month postsurgery mark will be juxtaposed with the preoperative data.
Statistical analysis
The data analysis was performed using SPSS 20.0 statistical software. Normally distributed continuous data are presented as mean ± standard deviation. Between-group comparisons were conducted using the independent samples t test, whereas paired data were analyzed with the paired t test. Nonnormally distributed continuous data are reported as median and interquartile range [M (P25, P75)], and group comparisons were performed using the Wilcoxon rank-sum test. Proportions between groups were compared using the chi-square test, with statistical significance set at P < 0.05.
Results
Perioperative characteristics
In the RA group, there were 20 males and 5 females, with 20 cases on the left side and 5 on the right. The median age was 58 days (range: 39.50–83.00), with the youngest patient being 27 days old. The average weight was 5.67 ± 0.75 kg, with a minimum weight of 4.5 kg, and the average height was 58.24 ± 4.30 cm, with a minimum height of 51 cm. All 25 cases of hydronephrosis in this group were categorized as grade III or above, with an SRF below 40%.
In the RB group, there were 15 males and 10 females, with 14 cases on the left side and 11 on the right. The median age was 746 days (range: 388.50–1082.00), with an average weight of 11.86 ± 3.72 kg and an average height of 82.64 ± 13.26 cm. All 25 cases of hydronephrosis in this group were also at grade III or above, with 23 cases having an SRF below 40% and/or continuously decreasing, and 2 cases presenting with pain or UTIs.
Statistical analysis revealed significant differences in age, weight, and height between the two groups (P < 0.05), as shown in Table 1.
Demographic Characteristics, Perioperative Data, and Complications
IQR = interquartile range; SRF = split renal function; UTIs = urinary tract infections; FLACC = Face, Legs, Activity, Cry, Consolability.
Both groups of children underwent surgeries performed by the same surgical team, and all procedures were completed smoothly without any instances requiring conversion to open surgery. The surgical time, defined as the period from skin incision to wound closure, was comparable between the two groups. The RA group having an average time of 165.64 ± 16.17 minutes and the RB group having an average time of 164.72 ± 18.94 minutes showed no significant difference. The console time was 108.25 ± 22.35 minutes for the RA group and 104.86 ± 24.19 minutes for the RB group, also showing no statistically significant difference. Postoperative FLACC pain scores were 2.14 ± 0.85 for the RA group and 2.31 ± 0.59 for the RB group, with no statistically significant distinction. Similarly, the postoperative hospitalization durations were 7.00 (6.00, 9.00) days for the RA group and 8.00 (7.00, 9.00) days for the RB group, with no statistically significant variance (P > 0.05).
In terms of postoperative complications, UTIs occurred in two cases in the RA group and three cases in the RB group. Among them, one case in the RB group was readmitted within 30 days. All cases were effectively managed through conservative treatments such as anti-infection therapy, fluid therapy, and symptomatic support. Macroscopic hematuria was reported in one case in the RA group and two cases in the RB group, with symptoms resolving after interventions including administration of vitamin K and phenylsulfonylethylamine, urine alkalization, and intensified anti-infection measures.
Regarding reoperations, one case in the RA group underwent a redo-pyeloplasty, one case in the RB group underwent a repeat redo-pyeloplasty, and one case underwent a pyelocentesis. There was no significant difference in the incidence of postoperative complications between the RA and RB groups (P > 0.05), as shown in Table 1.
The follow-up outcomes of renal hydronephrosis and SRF
In the RA group, the preoperative APD was measured to be 30.57 ± 8.98 mm, which significantly decreased to 14.72 ± 4.82 mm postoperatively (P < 0.05). Similarly, in the RB group, the preoperative APD was 34.71 ± 11.30 mm, which significantly decreased to 17.66 ± 6.78 mm postoperatively (P < 0.05). When comparing the change in APD values between the two groups before and after surgery, no statistically significant difference was observed (P > 0.05).
The preoperative SRF values in the RA group were 23.35 ± 8.24, significantly increasing to 36.83 ± 5.46 postoperatively (P < 0.05). Similarly, in the RB group, the preoperative SRF values were 21.69 ± 11.47, showing a significant increase to 33.73 ± 5.48 postoperatively (P < 0.05). When comparing the change in SRF before and after surgery between the two groups, no statistically significant difference was observed (P > 0.05).
As per the SFU grading method, 7 a reduction in SFU grade following surgery compared with the preoperative status is deemed as improvement. Furthermore, achieving a grade Ⅱ or lower postoperatively is classified as complete remission. 8
In the RA group, among the 25 renal units, 22 (88%) were classified as grade IV, and 3 (12%) as grade III. After pyeloplasty, 24 renal units (96%) improved to grade Ⅱ or below. Only one renal unit (4%) remained classified as grade III both before and after the surgery. In the RB group, among the 25 renal units, 18 (72%) were classified as grade IV, and 7 (28%) as grade III. After pyeloplasty, 22 renal units (88%) improved to grade Ⅱ or below, whereas 3 renal units (12%) remained at grade III. Of the 18 renal units that were grade IV before surgery, 2 improved to grade III, and 16 improved to grade Ⅱ or below. Of the seven renal units that were grade III before surgery, six improved to grade Ⅱ or below, whereas one remained at grade III. Therefore, in the RB group, 2 units (8%) showed improvement, and 22 units (88%) achieved complete resolution, as shown in Table 2.
Follow-up on Hydronephrosis and Split Renal Function
APD = anteroposterior diameter; ARF = split renal function; SFU = Society for Fetal Urology.
Discussion
As of now, there are no published cohort studies on the application of RALP in infants under 3 months old with UPJO. UPJO is a common cause of congenital hydronephrosis, 9 and severe hydronephrosis in the fetal period can lead to compression of the renal parenchyma, diminished renal blood flow, renal parenchyma thinning, and progressive deterioration of renal function if the obstruction is not promptly alleviated. 10 Delaying intervention and opting for conservative treatment before pyeloplasty can also affect the recovery of kidney morphology, function, and intrinsic growth and development. 11
Currently, there is no consensus on the optimal timing and surgical approach for treating UPJO in infants and young children. 12 Most experts recommend Anderson–Hynes pyeloplasty for children older than 3 months, whereas infants younger than 3 months often undergo initial intervention involving nephrostomy, followed by staged pyeloplasty. However, performing surgical incision and anastomosis in the diminutive diameter of the ureter poses challenges and increases the risk of complications such as anastomotic stenosis and leakage. Nevertheless, compared with older children, infants and young children have a lower likelihood of experiencing UTI and stones. They also exhibit reduced inflammation at the lesion site, less adhesion with perirenal tissue, better accessibility during surgical procedures, and reduced bodily trauma. These factors contribute to faster postoperative recovery and a lower incidence of associated complications.
With the advancement of surgical techniques and the development of surgical instruments, young age is no longer a contraindication for surgery. 13–14 In a retrospective study of 80 children younger than 2 months of age with UPJO, 40 of whom received prompt open surgery upon diagnosis and 40 who underwent traditional conservative management before open surgery, it was determined that the anterior and posterior dimensions of the renal pelvis and the thickness of the renal parenchyma were better in the early surgical group compared with those in the conservative observation group followed by surgery. Furthermore, it was observed that the renal anatomy and function of the latter may deteriorate gradually during conventional conservative treatment. 15 Another retrospective study reported 66 children with UPJO in the age range of 2 to 12 months, of which 34 underwent open surgery and 32 underwent laparoscopic surgery. The study concluded that both laparoscopic and open surgeries demonstrated comparable clinical efficacy and safety. 16 However, laparoscopic pyeloplasty (LP) still presents significant inadequacies when applied to infants under 3 months old. The intra-abdominal operating space of infants is limited, necessitating a prolonged learning curve for the surgeon. Furthermore, the precision of renal pelvis cutting and pelvic anastomosis is not as optimal as that achieved through open surgery.
The advent of robotic surgery has opened a new chapter in minimally invasive surgery. In contrast to laparoscopic surgery, robotic surgery systems offer high-resolution three-dimensional views, 10× magnification, motion view zoom and tremor filtering capabilities, instrument movements that simulate wrist movements, and surgeon-controlled camera positioning, 17 which eliminates the constraints of laparoscopic surgery in pediatric urology and renders intricate reconstructive surgery safer and more viable. Currently, robotic surgery has found extensive application in various pediatric urological procedures. 18–19 In their analysis, Sun et al. 20 studied 33 children aged 0 to 36 months with UPJO, comparing outcomes of RALP and LP. Of these, 12 underwent RALP and 21 underwent LP. The study found that RALP had a significantly shorter anastomosis time at the renal pelvis-ureter junction compared with LP, with a 100% success rate in the RALP group and 95.2% in the LP group. A critical review comparing RALP and LP in pediatric UPJO treatment, based on 19 original articles and 5 meta-analyses, concluded that RALP could reduce operative time, shorten hospital stay, lower complication rates, and achieve success rates similar to LP. 21 Nonetheless, it remains constrained by the limited abdominal cavity in children, posing challenges in creating sufficient operative space. The existing instrumentation is tailored for adult patients, lacking suitable devices for pediatric, particularly infant and young children. Further investigation is warranted to explore the optimal puncture channel layout, depth assessment, and surgical instrument selection.
Since 2018, our center has utilized RALP for the treatment of pediatric UPJO. Initially, we focused on children aged 3 years and above. As our surgical team gained proficiency and overcame the learning curve, we gradually expanded our inclusion criteria to include children aged under 3 months. In this study, both age groups underwent the surgery successfully, without any instances of open conversion. There were no statistically significant differences in operation duration, intraoperative blood loss, postoperative hospital stay, or the incidence of complications between the two groups. Postoperative APD and SRF significantly improved in both groups compared with the preoperative period. However, there was no statistically significant difference in the change values of these parameters between the two groups pre- and postoperation. Based on the data presented, it is evident that with mature and stable surgical techniques and proficient teamwork, RALP can achieve favorable surgical outcomes in the management of infants below 3 months of age and children above this age threshold. See Table 3 for a summary of the differences in RALP for different age groups in pediatric UPJO treatment.
Characteristics of RALP in Infants Under 3 Months and Children Aged 3 Months to 3 Years
SRF = split renal function; RALP = robot-assisted laparoscopic pyeloplasty; UTIs, urinary tract infections.
In this study, we outline our key insights from performing RALP in infants: (1) Incision approach selection: Our strategy involves opening the paracolic gutter ligament to expose the affected side’s renal pelvis and ureter. Although this method necessitates a larger incision and lateral peritoneum reconstruction, it offers the advantage of complete ureter exposure. This exposure facilitates the management of distal ureteral issues such as strictures or vascular compression. (2) Ureteral release: Straightening tortuous and adherent ureter segments is critical to prevent twisting during trimming, ensuring accurate identification of ureter walls. It is essential to maintain adequate blood supply during mobilization and avoid excessive electrocoagulation of small vessels. (3) Ureteropelvic anastomosis: Precision is key in trimming the ends of the renal pelvis and ureter to achieve clean edges. Aligning the lowest point of the ureter with the renal pelvis valve’s lowest point ensures a tension-free anastomosis. For closure, intermittent, externalized 6-0 Vicryl sutures were utilized spaced approximately 2 mm apart. Suturing the anterior and posterior walls with 6 to 8 stitches each is recommended, whereas continuous suturing can be considered for the residual renal pelvis tissue on both sides.
Conclusions
In summary, under the premise of mature and stable operation, the application of RALP in the treatment of UPJO in infants and young children is deemed safe and effective, embodying the principles of precision and minimally invasive intervention. The limitations of this study are that the sample size is small, the postoperative follow-up observation time is still short, and the long-term postoperative outcomes needs to be further investigated. Additionally, critical surgery-related factors such as the nutritional status of the child and liver function, along with other systemic evaluation indicators, were not comprehensively considered. Consequently, the conclusion is subject to certain constraints, warranting subsequent long-term follow-up or prospective in-depth research following an augmentation of the sample size in future endeavors.
Footnotes
Authors’ Contributions
Y.L., W.L., and C.C.: Study conception and design. S.X., H.Z., B.S., P.C., J.L., Z.Y., and W.L.: Material preparation, data collection, and analysis. W.L. and H.Z.: Initial article drafting. All authors reviewed and approved the final article.
Ethics Approval
This project fully considered and protected the rights and interests of the study objects. It meets the criteria of Ethical Review Committee. The Medical Ethics Committee of First Affiliated Hospital of Guangxi Medical University has approved the protocol.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This work was financed by grants from the Science and Technology Project of Guangxi Health Committee (No.S2019104) and the National Natural Science Foundation of China (no. 82160128).