
Abstract
Background and Objective:
The incidence of stone disease in children has risen worldwide, leading to the development of more treatment options. Percutaneous nephrolithotomy (PCNL) is often the preferred approach in many pediatric cases. This systematic review aims to assess the effectiveness and safety of PCNL in children, as well as to identify future directions for improving procedural outcomes.
Methods:
For this systematic review a comprehensive electronic search was conducted in PubMed and EMBASE in August 2023. The search included patients younger than 18 with renal stones requiring any modality of PCNL, as well as to establish the deficiencies in the reports of outcomes. The search strategy adhered to PRISMA guidelines, and quality assessments were performed using the Cochrane tool and MINORS tool.
Key Findings and Limitations:
Regardless of age, PCNL is safe and efficient in children, with stone-free rate above 85% and complication rate below 7%. However, neither the definition of stone free nor the way of reporting complications is homogeneous among studies. In addition, aspects such as diagnostic imaging, antibiotic prophylaxis, postoperative drainage, metabolic study, or follow-up are not systematically or uniformly reported in the studies.
Conclusions and Clinical Implications:
PCNL maintains its efficiency and safety even when the working tract caliber is reduced. However, the lack of standardization when describing pre-, peri-, and postoperative aspects creates a gap that does not allow grouping outcomes and highlights the lack of clear guidelines when implementing this surgical procedure.
Introduction
Over the past two decades, the incidence of urinary stone disease has surged, making pediatric urolithiasis an increasingly recognized issue worldwide, with considerable health care costs. 1 Because of common underlying metabolic and anatomical abnormalities, children are also considered a high-risk group for stone recurrence, with up to 50% experiencing recurrence within 3 years. 2 Thus, effective treatment of pediatric stone disease is critical.
Percutaneous nephrolithotomy (PCNL) was first introduced as a novel treatment for kidney stones in children by Hulbert et al. in 1985, replacing open surgery as the only option for patients with a high stone burden. 3 Since its implementation, the use of PCNL in pediatric patients has steadily increased—from 15.7% in 2001 to 26.6% in 2014—demonstrating its rising prominence. 4 Today, PCNL is a fundamental procedure for pediatric renal stones, recommended as the first-line treatment for stones ≥2 cm, staghorn stones, and stones ≥1 cm located in the lower pole calix, as per the European Association of Urology (EAU) guidelines. 5 However, the American Urological Association (AUA) guidelines recommend PCNL only for renal stones ≥2 cm. 6
Despite its increasing application, many critical preoperative, intraoperative, and postoperative aspects of pediatric PCNL remain underexplored. This systematic review by the EAU Young Academic Urologists Working Group Pediatric Urology aims to address questions regarding preoperative imaging, antibiotic prophylaxis, patient positioning, puncture techniques, dilatation practices, stone-free status, and complication rates. Our goal is to assess the current effectiveness and safety of PCNL in children and to identify future directions for improving the outcomes of this surgical technique.
Materials and Methods
Literature search
For this systematic review (PROSPERO ID: CRD42023456315), a comprehensive electronic search of PubMed and EMBASE was conducted in August 2023 using Medical Subject Headings terms, as outlined in Supplementary Table S1. All types of studies involving pediatric PCNL were considered, without restrictions on publication date, but only in English or Spanish. Original research, including randomized trials, cohort studies, and case series, was eligible for inclusion. When repeated cohorts of patients from the same authors were identified, the study with the largest number of patients and the clearest outcomes was chosen.
The search strategy adhered to PRISMA guidelines. Initial screening of titles and abstracts was independently performed by two authors (Y.Q.M. and L.A.‘t.H.), followed by a full-text review by all authors. Discrepancies were resolved through discussion or consultation with a third author (M.I.D.). Studies with fewer than 20 patients, nonoriginal studies, and studies involving adults were excluded.
Selection criteria
The search was guided by the Patient, Intervention, Comparison, Outcome (PICO) framework: P: Children (<18 years) with upper urinary tract stones requiring surgery. I: PCNL in all variations, with any lithotripter. C: Comparisons between different PCNL techniques (standard, mini, ultramini, supermini, micro). O: Effectiveness (stone-free rate, SFR) and safety (intra- and postoperative complications). As secondary outcomes, we evaluated the limitations of the studies when reporting their results, to propose recommendations to improve the quality of the evidence of PCNL in the pediatric population.
Key topics of interest included age, success prediction, diagnostic imaging, urine culture, patient positioning, puncture techniques, miniaturization of PCNL, tubeless vs standard PCNL, SFR, complications, metabolic evaluation, and long-term follow-up. The quality assessment of included studies was performed with the Cochrane tool for randomized clinical trials (RCT) and MINORS for cohort (maximum score 16 points) or comparative studies (maximum score 24 points). 7,8
Statistical analysis
The statistical analysis conducted was descriptive, focusing on means and percentages. A meta-analysis was not performed because many of the included studies could not be analyzed quantitatively because of the heterogeneity in the presentation of their results. In addition to the variability in outcomes, the definitions of success, complications, and the tools used to measure them differed significantly across studies. This lack of consistency made it difficult to aggregate the data.
Results
Characteristics of included studies
A total of 1394 articles were identified. After deduplication and abstract screening, 146 full-text articles were reviewed, and 80 publications involving 7174 patients were included in the final analysis (Fig. 1). The studies were grouped according to the PCNL techniques used, with Figure 2 illustrating the sheath size classifications. We classified sheaths ≤ 20Fr as minimally invasive. 9,10 Thus, the articles were grouped into standard-PCNL (Supplementary Table S211–30), mini-PCNL (Supplementary Table S331–60), ultramini-PCNL, and supermini percutaneous nephrolithotomy (SMP) (Supplementary Table S461–73), and microperc (Supplementary Table S574–80). Studies comparing PCNL with other lithiasis treatment modalities were included if PCNL characteristics and outcomes could be extracted separately. Articles comparing different types of PCNL with each other were analyzed separately (Supplementary Table S6 9,10,11 –18 ). In total, 9 RCTs 18 –26 and 71 cohort studies (16 prospective) were analyzed.

PRISMA flow diagram of the studies included in the systematic review.

Classification of PCNL according to the sheath size. PCNL = percutaneous nephrolithotomy; Fr = French; SMP = supermini percutaneous nephrolithotomy.
Although the diameter of the percutaneous tract overlaps between ultramini-PCNL and SMP, the difference is regarded as the latter has an integrated negative pressure system and therefore has a separate classification. 27
Risk-of-bias assessment
Using the Cochrane tool, all RCTs showed an uncertain or high risk of bias (Fig. 3). The average MINORS score for noncomparative cohort studies (n = 53) was 7/16, whereas comparative studies (n = 18) averaged 14/24.

Risk-of-bias assessment using Cochrane risk-of-bias tool in randomized clinical trials (RCTs).
Discussion
Does age alter the outcomes?
Only two of the selected studies performed subanalyses by age group, both concluding that age does not limit the safety and efficacy of PCNL, even in preschool-aged children. 28,29 Patil et al describe their results of mini-PCNL in 24 infants younger than 1 year, with an SFR of 91% and complications of 8.3%, all minor. What is striking about this study is its follow-up for more than 10 years, where they performed glomerular filtration rate and renal scintigraphy controls, demonstrating that the performance of a PCNL did not develop long-term complications for renal function. 30 Six other studies included only children younger than 3 years, with a high SFR (>83%) and mostly mild complications, confirming the feasibility of PCNL in young children. 18,31 –35
In a study by the CROES group comparing 107 children with adults, further subdividing children into preschoolers (0–4 years) and school-aged children (5–14 years) revealed no significant differences in baseline characteristics, success rates, operative times, or complications. 36 Similarly, a single-center study from Turkey involving 186 children younger than 6 years found no significant outcome differences between infants (<36 months) and preschoolers (>36 months to 6 years) aside from the preference for standard PCNL in older children. 37 These findings suggest that PCNL can be safely performed across all pediatric age groups when conducted in experienced centers.
Do nomograms help to predict the success of PCNL in children?
Several nomograms developed for adults, such as the S.T.O.N.E. score and Guy’s Stone Score (GSS), have been evaluated for use in pediatric patients. One of the included studies evaluated the S.T.O.N.E. nomogram. Although it proved useful for predicting surgical complexity, the study found it would be more effective if stone sizes and tract lengths were better matched to pediatric patients. 38 Meanwhile, the GSS shows promise in predicting SFRs in pediatric cases but does not adequately address the anatomical complexities often encountered in this population, limiting its effectiveness in predicting complications. 39 –41
To address this gap, the Stone/Kidney Score (SKS) was developed, using the stone/kidney index calculated by dividing the stone’s length by the kidney’s length and the number of stones. Higher SKSs correlated with lower SFRs and higher complication rates, suggesting this tool’s superiority over adult-based scoring systems. 42
Another nomogram, the Capital Medical University Nomogram (CMUN), was introduced by Zhang et al. in 2021 for predicting SFR based on stone mass, operation duration, irrigation, stone location and operation type. 43 However, further external validation is needed for both SKS and CMUN.
Preoperative assessment
Imaging
In this review, 55% of publications used CT scans for preoperative diagnosis, 11,12,16 –18,20 –23,25,26,28 –32,34,35,38,44 –68 whereas 30% used CT selectively without specifying the criteria for its use 9,10,13 –15,19,24,69 –85 . Six studies utilized combinations of ultrasound (US), kidney, ureter, and bladder radiograph (KUB), or intravenous pyelography (IVP) 86 –91 ; five studies did not report the diagnostic image 33,92 –95 and one study used US exclusively. 96
According to the EAU guidelines, CT should be reserved for cases where US or KUB is inadequate for diagnosis. 5 AUA guidelines advocate for low-radiation CT scans as they better define stone burden and anatomy while allowing the use of predictive nomograms with acceptable radiation exposure. 6 However, there are no pediatric studies that compare US with CT in the preoperative setting. A single study comparing CT with IVP in 50 children found no significant differences in operative times or SFRs, suggesting that IVP may be a viable alternative when CT is not available. 97
Preoperative urinary culture
A majority (72.5%) of studies in this review mentioned preoperative urine cultures or the use of prophylactic antibiotics, typically cephalosporins, based on institutional protocols. 9 –18,20,22,26,28 –30,32 –35,45 –47,50,52,54 –60,62 –68,70 –73,75 –81,83,84,87 –89,91,92,94 None addressed intraoperative sampling or stone cultures. Both EAU and AUA guidelines recommend preoperative urine 81 cultures and prophylactic antibiotics for PCNL, emphasizing their role in reducing postoperative infections and sepsis. 5,6,98 However, a quarter of the pediatric studies did not adhere to these recommendations.
Patient position
In 83.3% of the publications reviewed, PCNL was performed in the prone position. In contrast, only eight studies used the supine position, with two of these using both supine and prone positions. 21,26,50,51,53,57,68,87 In five studies, the patient’s position was not described at all. 69,74,86,89,92 Among the included articles, only one study focused on comparing both positions and found no differences in SFR, complication rate, or hospital stay. The only difference was surgical time, which was shorter in the supine group. 26
A recent meta-analysis in adults also found no differences in SFR between the two positions, but noted lower operative times and complications in the supine group. 99 However, evidence in pediatric populations remains sparse, with prone positioning continuing to be favored.
Percutaneous puncture
Fluoroscopy vs US
Of the included publications, 83.8% used fluoroscopy for percutaneous puncture. Fluoroscopy time (FT), a key determinant of radiation dose, was reported in only 41.3% of these studies, 9,13,20 –26,30,33,34,45,49,51,53,57,60,65 –67,73,75 –80,82,84,85,91,96 whereas 42.5% did not mention it. 10 –12,14 –16, 19,28,29,44,46 –48,50,52,55,56,58,59,61,62,64,69 –72,74,81,83,87 –90,95 The average FT in this review was 2.85 minutes, with a range of 0.33 to 7.68 minutes. In addition, 11.2% of the studies relied solely on US, 17,31,32,35,38,54,63,68,94 whereas ten studies utilized a combination of both imaging techniques. 16,34,66,72,74,78,79,83,91,96
Minimizing FT and radiation exposure is particularly critical in pediatric populations because of long-term risks. They will need more diagnostic and follow-up studies, and probably more interventions during their lifetime, there is a greater chance that the harmful effects of radiation will manifest after exposure. The increasing use of US for puncture and tract dilation, in line with the ALARA (As Low As Reasonably Achievable) principles, is noteworthy. 96,100 A recent systematic review of radiation doses in endourologic procedures in adults and children showed that while doses from PCNL, extracorporeal shockwave lithotripsy, and retrograde intrarenal surgery were below harmful levels (50mSv), they exceeded natural background radiation (2.4mSv). The cancer risk from these doses, particularly for PCNL, was assessed as minimal to low according to the International Commission on Radiological Protection guidelines. 101
Puncture site
Few studies detailed puncture site selection. One article demonstrated the safety of upper calix puncture in children, achieving an 86.6% SFR with low complication rates. 81 The vast majority of the studies included here do not even report the puncture site. Although supracostal puncture has been associated with increased risk of pleural injury, studies indicate that both supracostal and subcostal approaches can achieve high SFRs with careful technique. 102,103
Miniaturization of PCNL
Of the 80 studies reviewed, 52 focused on specific PCNL techniques, 17 compared PCNL with other lithotripsy modalities, and 10 compared different PCNL variants. Over time, miniaturized PCNL approaches, such as mini, ultramini, and micro-PCNL, have become more prevalent, with adult instruments still occasionally used in pediatric settings. When grouped by the size of the percutaneous approach, they were grouped as shown in Figure 4. The distribution of published articles over time according to the size of the percutaneous approach is presented, showing how different approach sizes have been reported throughout the years, in Figure 5.
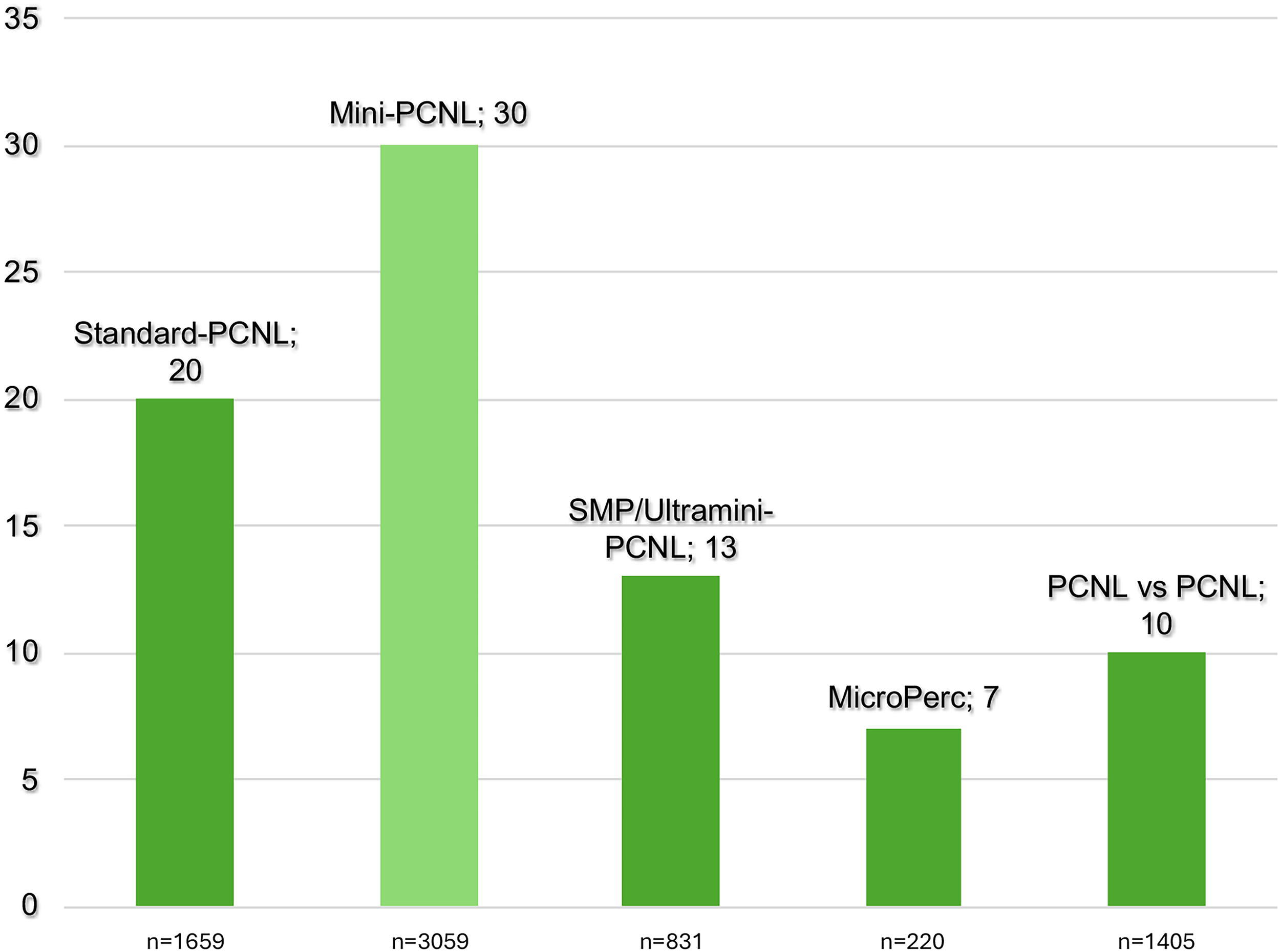
Distribution of the included studies regarding sheath size. SMP = supermini percutaneous nephrolithotomy.
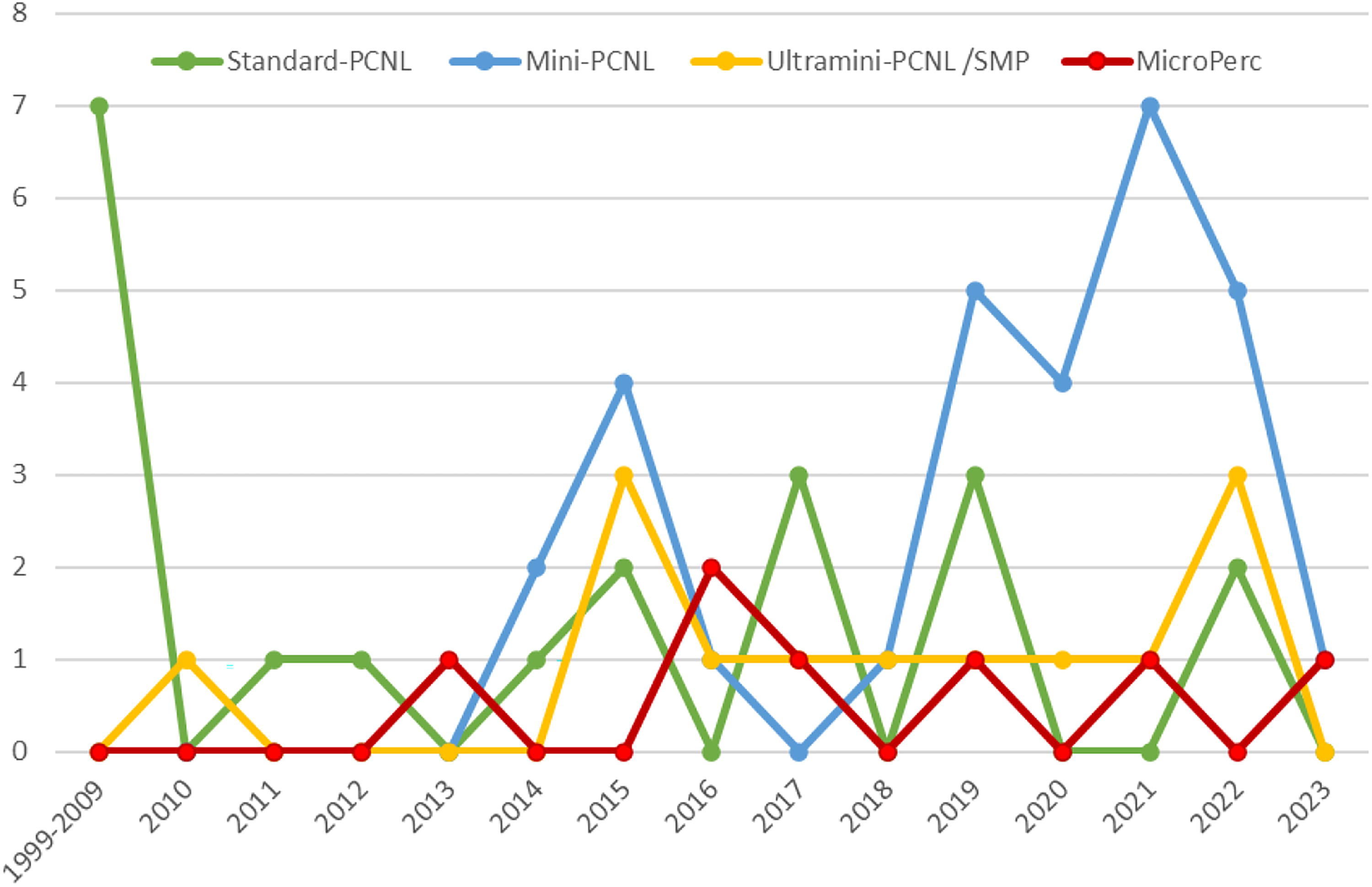
Trend of published articles over time according to the size of the percutaneous tract.
Twenty studies were performed with standard percutaneous approaches (>20Fr) (Supplementary Table S2) collecting 1659 patients with an average age of 8.9 years. The mean SFR reported was 87.8% with stones of 2.6 cm (45% of studies reported in cm) and 453.2 mm2 (40% of studies reported in this unit) on average. Only two studies used laser in combination with pneumatic lithotripters. 44,90 The mean operative time was 75.4 minutes and the average hospital stay was 3.5 days.
The 30 mini-PCNL studies (Supplementary Table S3) included a total of 3059 children with an average age of 6.8 years. The mean SFR reported was 89% for stones averaging 1.9 cm (based on 76.7% of studies that provided stone size in cm). Lithotripsy energy sources were evenly divided between lasers and pneumatic lithotripters and the surgical time ranged from 32 to 150 minutes (mean 66 minutes).
In the 13 studies using SMP or ultramini-PCNL (Supplementary Table S4), 831 patients with an average age of 5.4 years were included. The average size of the intervened stones was 1.8 cm and the reported SFR was 88.3%. Only one study reported the exclusive use of pneumatic lithotripter, 58 whereas the rest used a combination with laser or laser exclusively. The mean operative time was 62.4 minutes and the mean hospital stay was 3 days.
Regarding microperc, the seven studies (Supplementary Table S5) included 220 patients with an average age of 3.8 years. The mean SFR was 86% for stones with an average diameter of 1.4 cm. All of them used Ho:YAG laser, and found no cases in which thulium fiber laser was used. The average operative time was 63.8 minutes and the days of admission ranged from 1 to 3 days (2.2 days on average).
Terms such as standard-, mini-, ultramini-, supermini-, or micro-PCNL are often used in the literature, however, there is no single recognized classification. Neither in the EAU guidelines on urolithiasis (pediatric or adults) nor in the AUA guidelines on lithiasis is there a clear classification on the size of the different percutaneous access. 5,6,98 Within the studies comparing different PCNL modalities, three were between mini-PCNL and standard, 9,15,18 two SMP vs mini-PCNL, 16,17 two microperc vs mini-PCNL, 11,13 one mini-PCNL vs mini-PCNL, 14 and the last two mini-PCNL vs standard vs ultramini or microperc. 10,12 None of them found statistically significant differences in terms of SFR when comparing results, but three studies reported shorter operative times in those techniques that required less dilatation of the percutaneous tract, 11,14,16 except for one in which patients who underwent mini-PCNL took less time than those who underwent ultramini-PCNL 16 perhaps in relation to the faster extraction of the lithiasis because of the larger sheath. With respect to the length of stay, seven studies reported important differences, always pointing to fewer days for patients undergoing surgery with smaller caliber sheaths, 11 –13,15 –18 with the exception of the study by Mishra et al. 16 for whom it was statistically lower in the mini-PCNL vs ultramini-PCNL group, but this was clearly because the calculation was made in hours, but clinically it was not different in terms of the number of days of admission.
A 2017 systematic review highlighted the effectiveness of micro- and ultramini-PCNL. For microperc, the SFR was 67.5%–92%, for 12–16 mm stones and the complication rate was 9% (of which 19% were Clavien–Dindo III). Regarding ultramini-PCNL, the review reported an SFR of 76%–91.6% for stones with an average diameter of 21 mm, with 14% of complications (of which 23% were Clavien–Dindo III). This demonstrates that minimally invasive percutaneous approaches are also highly efficient despite the decreased percutaneous tract, with a lower complication rate. 104
The studies demonstrate that, despite the miniaturization of PCNL, its efficacy and safety are preserved. Over time, with increasing experience, complication rates have decreased. Moreover, for more complex clinical scenarios, these techniques can be combined with other modalities leading to procedures such as simultaneous bilateral endoscopic surgery and endoscopic combined intrarenal surgery.
Tubeless vs standard PCNL
The postoperative drainage strategies described in this review vary widely. As percutaneous approaches have become more miniaturized, the use of nephrostomies has decreased, whereas the roles of Double-J stents, ureteral catheters (UC), and tubeless (T) approaches have increased. In the standard PCNL group, all authors used nephrostomies (70% used nephrostomy alone, Supplementary Table S2), with only two studies mentioning the use of T methods. 19,47
Conversely, in the mini-PCNL group, 40% used nephrostomy alone, 21,22,24,38,53,56,57,75 –77,82,96 36.7% used a combination of nephrostomy, JJ stent, and UC 23,25,29 –32,50 –52,55,91 and 16.7% did not use nephrostomy. 54,78,80,92,93 Four studies reported some patients used T 31,54,79,92 and one did not describe the postoperative drainage. 81
In the SMP and ultramini-PCNL group, the use of combinations increased to 53.8% 26,33,59,60,64,83,94 and nephrostomy use alone decreased to 7.7% (66). The use of JJ stents or tubeless methods grew to 38.5%. 58,62,63,65,95 In the microperc group, no researchers used nephrostomies, and only one study reported the use of T methods. 34
The reduction in nephrostomy use did not correlate with an increased rate of complications. However, different techniques tended to shorten hospital stays as the tract caliber decreased (3.5, 3.2, 3, and 2.2 days for standard PCNL, mini-PCNL, SMP/ultramini-PCNL, and microperc, respectively). On the contrary, the operative time was higher in mini-PCNL (127 minutes) and SMP/ultramini-PCNL (115 minutes) than in standard PCNL (75 minutes).
In 2022, Gauhar et al. conducted a systematic review of RCTs to evaluate whether the T approach (ureteral stent/catheter without nephrostomy) is superior. 105 The review included 1839 patients across 26 studies: 907 patients underwent T PCNL, and 932 underwent standard PCNL with nephrostomy. The study found that the T approach was associated with shorter operative times, shorter hospital stays, and a lower rate of postoperative urinary fistulas. In addition, a meta-analysis of three studies comparing JJ catheters with standard nephrostomy in 147 pediatric patients found no significant difference in SFRs, hospital stays, or complication rates such as transfusions, infections, or urine leakage, supporting the safety and viability of T PCNL in children. 106
SFRs and residual fragments
Our analysis revealed mean SFRs of 85.1% (range 67.7%–100%) for standard PCNL, 89% (range 78%–97.2%) for mini-PCNL, 88.5% (76.9%–100%) for ultramini-PCNL and SMP, and 86.19% (80%–95.7%) for microperc. However, all of them had different definitions of SFR and different follow-up modalities. Variations in SFR definitions and follow-up modalities among studies complicate the comparison of PCNL efficacy. About 53.8% of studies defined SFR as the absence of lithiasis larger than 2, 3, or 4 mm, 11,14,17,19,21,25,26,28,32,35,38,44 –47,49 –51 ,53,55,57,59,60,62 –64,68,70 –72,77 –79,82 –84,87,89,90,92 –95 whereas 35% defined it as a complete absence of lithiasis on follow-up imaging, 10,12,13,16,20,22,23,29,30,34,48,52,54,56,58,61,65 –67,69,73 –76,80,81,86,88 with most using KUB and US. Nine studies did not even define SFR. 9,15,18,24,31,33,85,91,96
In adults, small fragments are often deemed clinically insignificant, but in children, any residual fragments are considered undesirable. However, many of the studies included in this review defined SFR as fragments smaller than 4 mm.
Complications
The most frequently reported complications were fever (6.3%), blood transfusion (2.9%), urinary tract infection (UTI) (1.7%), and hematuria (1.6%). By PCNL type, micro-PCNL had the highest rate of renal colic (7.7%), whereas fever was most common in SMP/ultramini-PCNL (6.6%), standard-PCNL (6.8%), and mini-PCNL (7.1%) (see Supplementary Tables S2, S3, S4, S5). Four intestinal injuries, 20,45,78,86 two arteriovenous malformations requiring embolization, 46,72 and one death because of sepsis were reported. 12
Standard-PCNL had the highest overall complication rate (22.2%), followed by miniPCNL (20.6%), microperc (17.3%), and SMP/ultramini-PCNL (11.9%). Notably, the proportion of Clavien–Dindo grade III or higher complications was similar in microperc (15.8%) and mini-PCNL (14.1%), whereas standard PCNL had a lower rate (10.6%). The SMP/ultramini-PCNL group had the lowest complication rate (8.1%). Comparisons between different PCNL types showed only one study with significant differences between mini-PCNL and SMP (25.3% vs 7.5%), with fever being the only complication reported in both groups. 17
In general, the most common complications of PCNL in children reported in the literature are hemorrhage, postoperative fever/UTI, and urinary leakage, which align with our findings. A Turkish multi-institutional study involving 1205 pediatric PCNL procedures reported complications in 27.7% of cases (10.1% required transfusion). Risk factors for increased complication rates included partial staghorn stones, sheath sizes greater than 20Fr, midcaliceal punctures, and longer operative times. These risk factors remained statistically significant in subanalyses. 107
Recent studies report postoperative infectious complications such as fever and UTI in less than 15%, with noninfectious causes also considered. Kaygisiz et al. reported a 3.5% UTI rate postoperatively, with risk factors including younger age, right-sided PCNL, staghorn stones, sheath sizes <20Fr, longer operative times, and blood transfusions. 108
Metabolic studies
Both EAU and AUA guidelines recommend a complete metabolic study of all children with lithiasis episodes. 5,6 However, only 32 of the 80 included studies in our analysis reported crystallographic or metabolic analysis 9,12,20,22,24 ,30 –33,46,48 –50,53,54,58,59,64,67,69,70,72,74 –76,78,80,86 –88,93,95 and at least half of these did not include all their patients. Notably, some studies mentioned presurgical metabolic analysis, although it is typically recommended after treatment in addition to stone analysis. Calcium oxalate and stones of infectious origin (calcium phosphate, struvite, ammonium, etc.) were the most frequently reported compositions in this review.
Long-term follow-up
Long-term follow-up in children is challenging because of the high rates of loss to follow-up. Nonetheless, it is essential to assess the impact of treatments on growth and renal function. There is no consensus on the duration, content, or timing of follow-up examinations, such as DMSA scans. In our analysis, the average follow-up duration was 7.4 months (ranging from 2 days to 12 years). Only 11 studies had a follow-up period longer than a year. 14,18,30,38,44,54,59,61,69,74,86 This lack of adherence to guidelines is concerning, given the high recurrence rates in children, yet many were discharged in less than 3 months. One of the longest follow-up studies, conducted by Patil et al. 30 followed 24 children under one year of age for an average of 12 years. All children showed normal renal growth and function for their age and body size. Of the 24 infants, only three had initial DMSA scan scars, but there was no progression of these scars during follow-up, and their overall renal function remained normal. Although these results may reduce the immediate need to assess renal function deterioration because of prior PCNL, they still highlight the importance of long-term follow-up. We need to consider how best to monitor these patients and for how long.
Future trends
PCNL miniaturization has demonstrated its versatility while maintaining excellent SFRs with low complications. This review herein supports this outcome. Accessories such as percutaneous sheaths with suction are tools that must prove its value even in the pediatric population. However, the SMP has so far shown encouraging results with its intrinsic negative pressure.
One of the most difficult steps of PCNL is without a doubt, the puncture. Some articles have been published on the use of 3D printing to enable surgeons to adequately plan the percutaneous access. 109 This could be a useful tool in the pediatric population, given the more frequent possibility of finding aberrant anatomies or having less space to perform the puncture and dilatation of the tract. Although there are no studies in children that have used this technology.
At the moment, one of the phases that needs improvement is the standardization of reporting. The International Alliance of Urolithiasis (IAU) made a checklist to standardize the results of the PCNL. 110 Among its recommendations is the reporting of the following: name of procedure, size of sheath, position of PCNL, modality of imaging used to perform access, operating time, drainage tube, radiation time, energy source for lithotripsy, length of stay, blood loss and blood transfusion, imaging modality and timing postoperatively, complications according to the Clavien–Dindo classification, urine leakage, analgesic requirement, and definition of success. Besides these, we would suggest to include also the preoperative diagnostic imaging as well as the antibiotic coverage and the radiation dose received by the patient. Most importantly, we need to reach consensus as pediatric urologists on what we consider as stone free and how and when it should be measured.
As limitations of this systematic review, only studies published in indexed journals were included, which may have introduced publication bias by excluding gray literature and potentially relevant unpublished studies. In addition, only English- and Spanish-language articles were considered, which may have led to the omission of important data from other linguistic sources, potentially affecting the generalizability of our findings. Another limitation was the lack of specific data on special subpopulations within the pediatric cohort, such as patients with genitourinary malformations or neurologic conditions, which could significantly impact the success and complication rates. Furthermore, because of substantial heterogeneity in the definition of success and the classification of complications across studies, a meta-analysis could not be performed, limiting the ability to provide a quantitative synthesis of the evidence. However, a rigorous quality assessment of the included studies was conducted to ensure methodologic reliability.
Conclusion
In conclusion, our systematic review, including 80 studies with 7174 pediatric patients undergoing PCNL, supports that PCNL in children is safe and feasible, regardless of the age at which it is performed. Its efficacy does not diminish despite a decrease in the caliber of the percutaneous working channel and will likely continue to improve as the experience of pediatric urologists increases and the development of new technologies continues. Improvement of uniform registration of the pre-, peri-, and postoperative steps is needed. In addition, a precise definition of SFRs and standardized measurement methods are urgently needed.
Footnotes
Take Home Message
PCNL in children is effective and safe, maintaining efficacy with a smaller percutaneous tract and fewer serious complications. However, outcome reports lack standardization, and the literature often lacks essential data to assess its impact on pediatric patients.
Authors’ Contributions
Y.Q.M.: Study design, data extraction, synthesis of extracted data, and article revision. M.İ.D.: Article review, data extraction, and article revision. R.J.M.L.: Article review, data extraction, and article revision. B.B.M.: Article review, data extraction, and article revision. N.B.: Article review, data extraction, and article revision. E.B.: Article revision. S.S.: Article revision. L.A.‘t.H.: Article review, data extraction, and article revision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.