
Abstract
Objective:
To test whether the contemporary robot-assisted nephroureterectomy (RNU) is associated with more favorable in-hospital outcomes than historical RNU, relative to the same endpoints in open NU (ONU).
Methods:
Within the National Inpatient Sample (2008–2019), we identified RNU and ONU patients. Multivariable logistic and Poisson regression models were fitted.
Results:
Of 8032 NU patients, historical (2008–2013) vs contemporary (2014–2019) proportions were 776 (41%) vs 1104 (59%) for RNU and 3719 (60%) vs 2433 (40%) for ONU. The rates of RNU have increased over time (2008–2019; Δ absolute: +18%; p < 0.001). Contemporary RNU patients exhibited significantly better in-hospital outcomes in 6 of 12 comparisons vs historical that ranged from −54% for genitourinary complications to −12% for median length of stay (LOS). Contemporary ONU patients also exhibited significantly better in-hospital outcomes in 11 of 12 comparisons vs historical that ranged from −67% for blood transfusions to −26% for gastrointestinal complications. When historical RNU was compared with historical ONU, RNU in-hospital outcomes were better in 7 of 12 comparisons that ranged from −61% for median LOS to −16% for postoperative complications. Conversely, when contemporary RNU was compared with contemporary ONU, RNU in-hospital outcomes were only better in 2 of 12 comparisons: −25% cardiac complications and −13% for median LOS.
Conclusion:
The magnitude of in-hospital outcomes categories improvement between historical vs contemporary was two-fold more pronounced in ONU (11 improved categories) than in RNU (6 improved categories). Few outcome benefits remained (two categories only) when contemporary RNU was compared with contemporary ONU.
Introduction
Nephroureterectomy (NU) is a guideline-recommended standard treatment for nonmetastatic upper urinary tract cancer (UUTC). 1,2 Of NUs, an increasingly large proportion is performed with robot assistance. 3 –5 Based on the “practice makes perfect” hypothesis, 6 we postulated that contemporary outcomes after robot-assisted NU (RNU) have improved compared with their historical RNU counterparts. To the best of our knowledge, no previous study addressed the comparison between historical vs contemporary in-hospital outcomes after RNU. We addressed this knowledge gap. We also hypothesized that differences in in-hospital outcomes between RNU and open NU (ONU) recorded in historical patients may have been eliminated in contemporary patients. To test these hypotheses, we relied on the most contemporary National Inpatient Sample (NIS; 2008–2019) database.
Methods
Data source
To test for in-hospital outcomes after NU, we relied on discharge data from the NIS (2008–2019). All diagnoses and procedures were coded using the International Classification of Disease (ICD) 9th revision Clinical Modification (ICD-9-CM), ICD 10th revision Clinical Modification (ICD-10-CM), as well as ICD 10th revision Procedure Coding System (ICD-10-PCS).
Study population
We focused on patients aged ≥18 years with a primary diagnosis of nonmetastatic UUTC (ICD-9-CM codes 188.6–188.9, 189.1, and 189.2, and ICD-10-CM code C65.0-C65.2, C66.0-C66.2, and C66.9). Only patients treated with RNU or ONU were included. 7
Definition of variables for analyses
Study endpoints consisted of in-hospital outcomes, defined as overall, intraoperative, and cumulative postoperative complications as well as specific complication categories (gastrointestinal, pulmonary, cardiac, and genitourinary complications), perioperative bleeding, blood transfusions, median length of stay (LOS), in-hospital mortality, and critical care therapy (CCT) use. 8 –12 Covariates consisted of patient and hospital characteristics. Patient characteristics were age at admission (years and continuously coded), sex (female vs male), and Charlson Comorbidity Index (0 vs 1–2 vs ≥3). Hospital characteristics were teaching hospital status (teaching vs nonteaching) and hospital bed size (large [≥400 beds] vs medium [200–399 beds] vs small [<200 beds]).
Statistical analyses
First, patient and hospital characteristics as well as in-hospital outcomes rates were tabulated. Second, multivariable logistic and Poisson regression models predicting in-hospital outcomes were fitted after adjustment for clustering at the hospital level, using generalized estimation equation methodology. 13 –15 Overall, four comparisons were made. In the first part of the analyses, contemporary RNU was compared with historical RNU (first comparison), and subsequently contemporary ONU was compared with historical ONU (second comparison). In the second part of the analyses, historical RNU was compared with historical ONU (third comparison), and subsequently, contemporary RNU was compared with contemporary ONU (fourth comparison). Due to the NIS data reporting agreement, counts and associated proportions were reported as <11 for sample sizes <11. 16 All tests were two-sided, with a significance level set at p < 0.05. R software environment was used for statistical computing and graphics (R version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
Descriptive characteristics of the study population
Within the NIS, we identified 8032 nonmetastatic UUT patients who underwent NU between 2008 and 2019 (Table 1). Of RNU patients, 41% (n = 776) were historical and 59% (n = 1104) were contemporary (Δ absolute: +18%; relative ratio: 1.43, p < 0.001; Supplementary Fig. S1). Of ONU patients, 60% (n = 3719) were historical and 40% (n = 2433) were contemporary (Δ absolute: −20%; relative ratio: 0.66, p < 0.001; Fig. 1). Among 1880 RNU patients, contemporary RNU patients were younger (70 vs 71 years, p = 0.01). Contemporary RNU patients were more frequently treated at teaching hospitals (82.0 vs 70.0%, p < 0.001) and at medium bed size hospitals (27.0 vs 17.0%, p < 0.001) but a lower proportion (59.0 vs 68.0%, p < 0.001) was treated at large bed size hospitals. No statistically or clinically meaningful differences were recorded for the remaining characteristics.
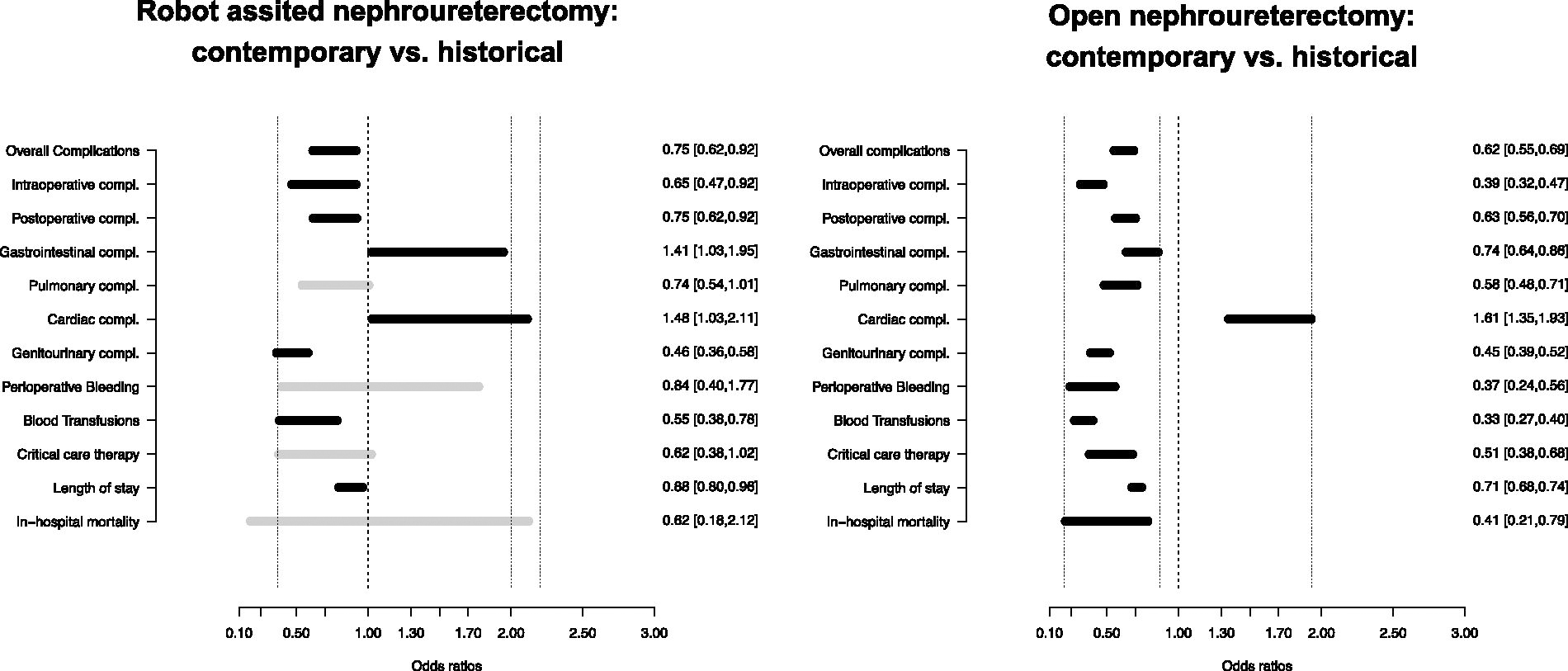
Forrest plot depicting multivariable-adjusted comparison of in-hospital outcomes in 1880 robot-assisted vs 6152 open nephroureterectomy according to study years (2008–2013 vs 2014–2019).
Descriptive Characteristics of 8032 Nonmetastatic Upper Urinary Tract Cancer Patients Undergoing Radical Nephroureterectomy According to Surgical Approach (Robot-Assisted Vs Open) Within the Nationwide Inpatient Sample from 2008 to 2019
Wilcoxon rank sum test; Pearson’s chi-square test; Fisher’s exact test.
IQR = interquartile range.
Among 6152 ONU patients, contemporary ONU patients were older (73 vs 72 years, p = 0.02). Contemporary ONU patients were more frequently treated at teaching hospitals (79.0 vs 56.0%, p < 0.001) and at medium bed size hospitals (26.0 vs 21.0%, p < 0.001), but a lower proportion (60.0 vs 68.0%, p < 0.001) was treated at large bed size hospitals. No statistically or clinically meaningful differences were recorded for the remaining characteristics.
First comparison: Contemporary vs historical RNU
Contemporary RNU patients exhibited significantly better in-hospital outcomes in 6 of 12 examined categories (Supplementary Fig. S2), namely overall (46.0 vs 51.0%), intraoperative (6.9 vs 9.9%) and cumulative postoperative complications (43.0 vs 46.0%), genitourinary complications (17.0 vs 29.0%), blood transfusions (5.8 vs 10.0%), and median LOS (2 vs 3 days; all p ≤ 0.02; Table 2). Conversely, contemporary RNU patients exhibited significantly worse in-hospital outcomes in 2 of 12 examined categories, namely gastrointestinal (12.0 vs 8.9%) and cardiac complications (9.1 vs 6.6%; all p ≤ 0.04). After multivariable adjustment (Supplementary Table S1, Fig. 1), contemporary RNU independently predicted better in-hospital outcomes in 6 of 12 examined categories, namely overall complications (odds ratio [OR]: 0.75), intraoperative complications (OR: 0.65), postoperative complications (OR: 0.75), genitourinary complications (OR: 0.46), blood transfusions (OR: 0.55), and median LOS (OR: 0.88; all p ≤ 0.01). Conversely, contemporary RNU independently predicted worse outcomes in 2 of 12 examined categories, namely gastrointestinal complications (OR: 1.41) and cardiac complications (OR: 1.48; all p = 0.02).
Rates of In-Hospital Outcomes in 1880 Robot-Assisted Vs 6152 Open Nephroureterectomy According to Study Years (2008–2013 Vs 2014–2019)
Wilcoxon rank sum test; Pearson’s chi-square test; Fisher’s exact test.
Second comparison: Contemporary vs historical ONU
Contemporary ONU patients exhibited significantly better in-hospital outcomes in 11 of 12 examined categories, namely overall (48.0 vs 59.0%), intraoperative (6.2 vs 15.0%), cumulative postoperative complications (45.0 vs 52.0%), gastrointestinal complications (14.0 vs 18.0%), pulmonary complications (7.4 vs 12.0%), genitourinary complications (14.0 vs 27.0%), perioperative bleeding (1.2 vs 3.1%), blood transfusions (7.5 vs 20.0%), CCT (2.9 vs 5.6%), median LOS (3 vs 5 days), and in-hospital mortality (0.5 vs 1.2%; all p ≤ 0.001; Table 2). Conversely, contemporary ONU patients independently predicted only one worse in-hospital outcome, namely cardiac complications (13.0 vs 8.2%, p < 0.001). After multivariable adjustment (Supplementary Table S1, Fig. 1), contemporary ONU independently predicted better in-hospital outcomes in 11 of 12 examined categories, namely overall complications (OR: 0.62), intraoperative complications (OR: 0.39), cumulative postoperative complications (OR: 0.63), gastrointestinal complications (OR: 0.74), pulmonary complications (OR: 0.58), genitourinary complications (OR: 0.45), perioperative bleeding (OR: 0.37), blood transfusions (OR: 0.33), CCT use (OR: 0.51), median LOS (OR: 0.71), and in-hospital mortality (OR: 0.41; all p ≤ 0.001). Conversely, contemporary RNU independently predicted worse in-hospital outcomes only in one examined category, namely, cardiac complications (OR: 1.61, p < 0.001).
Third comparison: Historical RNU vs historical ONU
Historical RNU patients exhibited significantly better in-hospital outcomes in 7 of 12 examined categories, namely overall (51.0 vs 59.0%), intraoperative (9.9 vs 15.0%) and cumulative postoperative complications (46.0 vs 52.0%), gastrointestinal complications (8.9 vs 18.0%), pulmonary complications (9.5 vs 12.0%), perioperative bleeding (1.5 vs 3.1%), blood transfusions (10.0 vs 20.0%), and median LOS (3 vs 5 days; all p ≤ 0.04; Table 3). After multivariable adjustment (Supplementary Table S2, Fig. 2), historical RNU independently predicted better in-hospital outcomes in 7 of 12 examined categories, namely overall (OR: 0.78), intraoperative (OR: 0.66) and cumulative postoperative complications (OR: 0.84), gastrointestinal complications (OR: 0.48), perioperative bleeding (OR: 0.50), blood transfusions (OR: 0.49), and median LOS (OR: 0.39; all p ≤ 0.03).
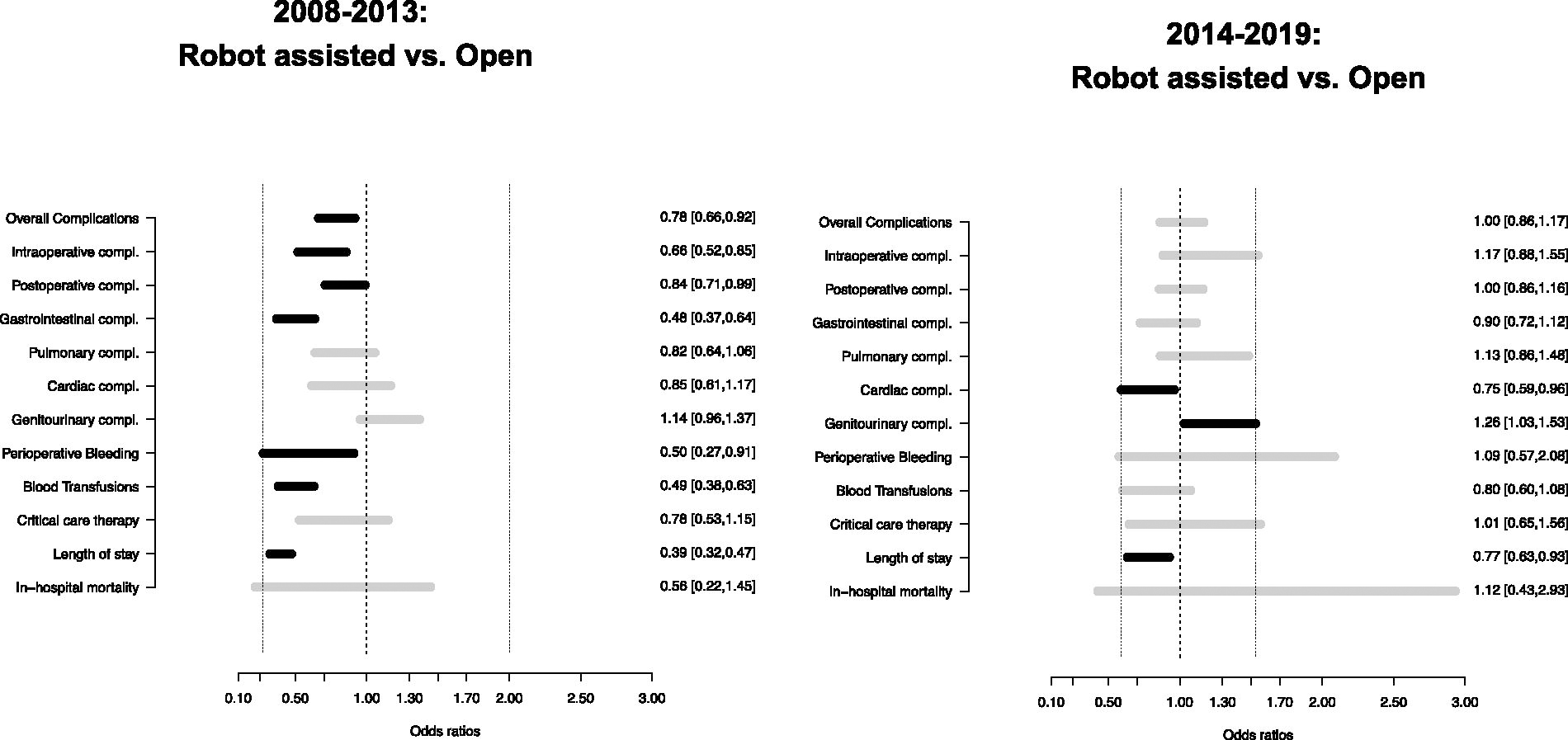
Forrest plot depicting multivariable-adjusted comparison of in-hospital outcomes in 4495 historical (2008–2013) vs 3537 contemporary (2014–2019) upper urinary tract carcinoma patients who underwent nephroureterectomy according to surgical approach (robot-assisted vs open).
Rates of In-Hospital Outcomes in 4495 Historical (2008–2013) Vs 3537 Contemporary (2014–2019) Upper Urinary Tract Carcinoma Patients Who Underwent Nephroureterectomy According to Surgical Approach (Robot-Assisted Vs Open)
Wilcoxon rank sum test; Pearson’s chi-square test; Fisher’s exact test.
Fourth comparison: Contemporary RNU vs contemporary ONU
Contemporary RNU patients exhibited significantly better in-hospital outcomes in 2 of 12 examined categories, namely cardiac complications (9.1 vs 13.0%, p < 0.001) and median LOS (2 vs 3 days, p < 0.001; Table 3). Conversely, contemporary RNU patients exhibited worse in-hospital outcomes in only 1 of 12 examined categories, namely genitourinary complications (17.0 vs 14.0%, p = 0.02). After multivariable adjustment (Supplementary Table S2, Fig. 2), contemporary RNU independently predicted better in-hospital outcomes in 2 of 12 examined categories, namely cardiac complications (OR: 0.75) and median LOS (OR: 0.77; all p ≤ 0.01). Conversely, contemporary RNU independently predicted worse in-hospital outcomes only in one examined category, namely genitourinary complications (OR: 1.26, p = 0.02).
Discussion
RNU patients exhibited more favorable in-hospital outcomes than ONU patients based on three reports. 3 –5 Of those, one originates from a single institution, 5 one is multi-institutional, 3 and the last is population-based. 4 The single-institution (Zeuschner et al.; n = 131) and the multi-institutional (Grossman et al.) studies are based on relatively small sizes. 3,5 For example, Grossman et al. described 473 (19.4%) RNU patients and 1096 (45.0%) ONU patients who underwent surgery between 1990 and 2020. 3 Conversely, Pearce et al. relied on a simulated patient cohort where the recorded NIS observations were weighted to reflect the U.S. population. 4 In consequence, these counts do not reflect true patient observations and cannot be directly compared with studies with real patient observations, such as the current study. Here, we relied on true NIS patient observations (2008–2019) and performed comparisons between contemporary vs historical RNU, contemporary vs historical ONU. Two additional comparisons were also performed between historical RNU vs ONU and contemporary RNU vs ONU. We made several noteworthy observations.
First, UUTC is rare. 1,3,4 For example, in their multi-institutional study of RNUs (n = 473) vs ONUs (n = 1096), Grossman et al. relied on 21 European, North American, and Asian participating centers, with a study span of 31 years (1990–2020). 3 Only 473 (19.4%) RNU and 1096 (45.0%) ONU patients were included. 3 In consequence, less than one RNU patient (average 0.7) and less than two ONU patients (average 1.7) were included annually at each institution. Clearly, large-scale data repositories, such as NIS, are needed to study NU patients as was done in the current study as well as in Pearce et al.’s study. 4
Second, within the current study, we identified 776 (41.0%) historical and 1104 (59.0%) contemporary RNUs (Δ absolute: +18%; relative ratio: 1.43, p < 0.001). These numbers imply a 1.43-fold increase in RNUs over the study span (2008–2019). Within the same dataset, we also identified 3719 (60.0%) historical and 2433 (40.0%) contemporary ONUs. These numbers indicate a 34% decrease in ONUs over the study span (2008–2019). These observations are consistent with other reports. 4,17
Third, we tabulated patient and hospital characteristics of contemporary vs historical RNU patients. Interestingly, contemporary RNU patients were younger (70 vs 71 years) and more frequently treated at teaching institutions (82 vs 70%), where more favorable outcomes are usually reported. 18,19 Conversely, fewer contemporary RNU patients were treated at large bed size hospitals (59 vs 68%) where favorable outcomes are more frequently expected. 6 In contemporary ONU patients, an even larger proportion of patients were treated at teaching institutions (79 vs 56%). Conversely, fewer contemporary ONU patients were treated at large bed size hospitals (60 vs 68%). Additionally, contemporary ONU patients were older (73 vs 72 years), and less favorable outcomes are expected in older patients. These observations suggest a more pronounced disadvantage in baseline patient characteristics in the contemporary vs historical ONU comparison than in the contemporary vs historical RNU comparison.
Fourth, we addressed differences in in-hospital outcomes and performed four different comparisons. In the first comparison (Table 2), we contrasted contemporary RNU with historical RNU. Contemporary RNU patients exhibited more favorable in-hospital outcomes in 6 of 12 categories (overall, intraoperative and cumulative postoperative complications, genitourinary complications, blood transfusions, and median LOS) even after multivariable adjustment (Supplementary Table S1). In the second comparison (Table 2), we contrasted contemporary ONU with historical ONU. Here, a larger number of differences were recorded. Specifically, contemporary ONU patients exhibited better in-hospital outcomes in 11 of 12 comparisons (overall, intraoperative and cumulative postoperative complications, gastrointestinal complications, pulmonary complications, genitourinary complications, perioperative bleeding, blood transfusions, CCT use, median LOS, and in-hospital mortality) even after multivariable adjustment (Fig. 1). These findings of better outcomes in both contemporary vs historical RNU and contemporary ONU vs historical ONU comparisons have not been previously reported. It may be possible that these improvements are due to either the surgical expertise or the appropriate selection of UUTC patients in which NU is contemplated. However, these hypotheses to be either confirmed or confuted require further prospective studies relying on a wider amount of data.
To better investigate the above phenomenon, we contrasted historical RNU patients with their historical ONU counterparts. As in previous historical reports addressing in-hospital outcomes, we also recorded more favorable findings after historical RNU than after historical ONU. 3 –5 Specifically, historical RNU (Table 3; 2008–2013) was an independent predictor of more favorable in-hospital outcomes than after historical ONU in 7 of 12 comparisons (overall, intraoperative and cumulative postoperative complications, gastrointestinal complications, perioperative bleeding, blood transfusions, and median LOS).
In the fourth and final comparison (Table 3), we contrasted contemporary RNU vs contemporary ONU. Here, we recorded no differences between these two approaches (Table 3; 2014–2019). Specifically, only 2 of 12 examined in-hospital outcome categories demonstrated statistically significant differences: cardiac complications (13.0 vs 9.1%, OR: 0.75) and LOS (3 vs 2 days; OR: 0.77). However, 10 of 12 examined in-hospital outcomes were not different between contemporary RNU and contemporary ONU. For example, when overall complications (46.0 vs 48.0%), intraoperative complications (6.9 vs 6.2%), and overall postoperative complications (43.0 vs 45.0%, p = 0.7) were considered, contemporary RNU offered no tangible advantage compared with contemporary ONU. Lack of advantage was also recorded for seven of eight specific postoperative complications (gastrointestinal, pulmonary and genitourinary complications, perioperative bleeding, blood transfusions, CCT, and in-hospital mortality). These observations indicate that the same in-hospital outcomes may be expected after contemporary RNU and ONU. In consequence, contemporary ONU should be given the same consideration as contemporary RNU in clinical decision-making.
Taken together, the current study demonstrated important absolute and relative increases (Δ: +18%; 1.43) in the numbers of contemporary vs historical RNU. Concomitant absolute and relative (Δ: −20%, 0.66) decreases in contemporary ONU have also occurred. Current study comparisons between historical RNU vs historical ONU are in agreement with historical reports where historical RNU in-hospital outcomes were more favorable than historical ONU. However, the contemporary RNU and ONU comparison that is reported for the first time in the current study indicates the absence of differences in in-hospital outcomes between the two approaches. In consequence, when in-hospital outcomes represent the endpoint of interest, contemporary RNU does not offer a tangible advantage over contemporary ONU. These observations should ideally be used in preoperative counseling and clinical decision-making to reassure patients in whom NU is contemplated.
Despite the novelty of our observations, the present study has inherent limitations. First, it is retrospective with selection and reporting biases, 20 as in other NIS studies. 4,7,21 –24 Second, RNU patient counts are still relatively limited. 25,26 Third, the pathological stage, the bladder cuff management, and the extent of lymphadenectomy are unavailable. 27,28 Fourth, procedural details (operative time, estimated blood loss, hemostatic agents, and preoperative and postoperative laboratory results) are unavailable. 29 Fifth, surgical and/or institutional expertise cannot be accounted for. Finally, within the NIS, only in-hospital data are available.
Conclusion
The magnitude of in-hospital outcomes categories improvement between historical vs contemporary was two-fold more pronounced in ONU (11 improved categories) than in RNU (6 improved categories). Few outcome benefits remained (two categories only) when contemporary RNU was compared with contemporary ONU.
Footnotes
Authors’ Contributions
F.D.B. and C.C.R.: Conceptualization. F.D.B., N.R.P., and P.I.K.: Methodology. G.C., M.L., and F.F.: Validation. Z.T., Q.C.L., M.C., and F.D.B.: Formal analysis. A.M., F.H.K.C., and O.D.C.: Investigation. N.L.: Resources. J.A.G., G.C., F.D.B., and C.C.R.: Data curation. F.D.B., S.P., A.B., S.S., and F.S.: Writing—original draft preparation. F.S., M.C., M.G., P.I.K., and F.M.: Writing—review and editing. G.C. and S.P.: Visualization. N.L. and S.P.: Supervision. M.C., P.I.K., and N.L.: Project administration. All authors have read and agreed to the published version of the article.
Data Availability Statement
All analyses and their reporting followed the NIS reporting guidelines. The specific datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research received no external funding.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.