
Abstract
Background:
Iatrogenic lesions of the distal ureter represent a frequent and feared complication of abdominal surgery that is traditionally managed by ureteral reimplantation. The aim of this systematic review (SR) is to summarize the published literature on the role of minimally invasive ureteroureterostomy (UU) in the surgical treatment of non-neoplastic distal ureteral lesions.
Methods:
We performed a comprehensive literature search on PubMed, Embase, and Cochrane CENTRAL including published peer-reviewed studies according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The intra-, peri-, and postoperative outcomes as well as the safety profile and the success rates of minimally invasive UU are presented.
Results:
Seven retrospective studies with 116 patients were included in this SR. If the basic principles of the ureteral reconstructive procedure are followed, both laparoscopic and robotic UU are feasible, safe, and with a success rate ranging between 81.8% and 100%, depending on the definition of success. A single comparative study documented a significant difference in operative time and length of hospitalization in favor of robotic UU. The success of both laparoscopic and robotic UU has been mainly evaluated in the short and intermediate follow-up.
Conclusion:
Minimally invasive UU may represent a viable treatment option for the treatment of non-neoplastic distal ureter pathology such as iatrogenic injuries or radiotherapy-induced stenosis. Larger, prospective studies adopting a standard definition of the postoperative success are required to affirm UU as a first-line option in the management of benign distal ureteral lesions.
Introduction
Iatrogenic lesions of the ureter are a frequent complication of abdominal surgery with an incidence ranging between 0.5% and 1% of all surgical procedures. 1 Gynaecologic, colorectal, urologic, spinal, and vascular surgical procedures are the most frequent iatrogenic causes. 2,3 These injuries can result in partial or total ureteral damage and/or subsequent stenosis. The pelvic tract of the ureter is the most frequently involved (91% of cases). 4
Although temporary nephrostomy tubes or ureteral catheters are frequently adopted for the initial management, surgical repair is often required. The surgical strategy is decided based on the location, length and etiopathology of the ureteral stenosis, and for distal ureteral lesions is mainly represented by the ureteroneocystostomy (UCN) with or without bladder psoas hitch. 5 –7 Ureteroureterostomy (UU) is another surgical option that is mainly adopted for the surgical repair of lesions of the upper and mid ureter. Concerning the management of lesions of the distal ureter, however, UU has been historically considered challenging to perform in the deep, narrow, and dark working space of the pelvis. In open surgery, UU is associated with high failure rates due to the fragile plexiform vessels that supply the distal ureter. Furthermore, achieving a wide tension-free anastomosis in the deep pelvis is particularly challenging. 7
These issues have been partially overcome by traditional laparoscopy that started to provide enhanced visibility through magnification of the image and improved illumination that allowed for a better definition of pelvic anatomical landmarks. 7,8 The subsequent advent of robotics further improved the ability of the surgeon to operate in narrow working spaces using EndoWrist instruments and filtering the physiological hand tremor. 9,10
Based on this technological progress, UU is actually being reconsidered by several authors as a first-line surgical option for lesions of the distal ureter located at >2 cm from the bladder. Compared with UCN, UU provides the considerable advantage to preserve the integrity of the bladder and the natural antireflux mechanism of the intramural ureter. 11,12
The aim of this systematic review (SR) is to summarize the published literature on the role of minimally invasive UU in the surgical treatment of distal ureteral lesions and to report and analyze its intra-, peri- and postoperative outcomes.
Materials and Methods
The present SR was performed and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement. 13 Considering the data scarcity and heterogeneity of the included studies, the current article was naturally directed toward an SR without meta-analysis.
Search strategy
We performed a comprehensive literature search on PubMed, Embase, and Cochrane CENTRAL including published peer-reviewed studies. The keyword search was performed using both Medical Subject Headings terms and free text. The research strategy protocol is depicted in Supplementary Data S1.
Inclusion and exclusion criteria
Two authors (E.R. and A.D.A.) independently screened all titles, abstracts, and full-text records against the eligibility criteria by collating them in an Excel sheet. In case of any disagreement, a third author (R.M.) solved the divergence. No automation tools were used.
For this SR, we included randomised trials, cohort studies, and case-control studies. Case reports or studies including <3 patients, surveys, expert opinions, editorials, and abstracts, as well as guidelines, review articles, and meta-analyses, were excluded. Moreover, studies referring to a pediatric cohort as well as studies based on animal or cadaveric models were also excluded. We included all articles concerning mini-invasive (laparoscopic or robotic) distal ureteral repair for iatrogenic lesions that occurred after surgery (pelvic surgery or endourology) and after radiotherapy. Patients with stenosis due to endometriosis were considered for inclusion, whereas patients affected by distal ureteral stenosis because of cancer, kidney transplantation, or infectious disease were excluded. Finally, studies that included distal ureteral repair or stenosis treated with ureteroneocystostomy without providing a comparison with UU were not included.
Data collection process and data items
Eligible outcomes were broadly categorised as follows: 1) study characteristics; 2) baseline characteristics; 3a) type of surgery and peri- and 3b) postoperative outcomes, and 4) follow-up evaluations.
Concerning the study characteristics, information about the authors, years of publication, and the institution where the study has been conducted as well as the design of the study and the Institutional Review Board Approval (IRB) were collected.
Baseline parameters included the number and the age of participants (years, mean ± SD, range, and median), side of ureteral injuries, ureteral stenosis length (mm, mean ± SD, range, and median) and cause of the iatrogenic lesions/stenosis (previous pelvic, endoscopic surgery, or radiotherapy treatment). Numbers and rates of previous endoscopic treatment to treat the stenosis and previous positioning of the nephrostomy tube or stenting JJ were also reported.
Concerning surgical aspects, the following items were extracted: number of patients, type of surgery (principal intervention and adjunctive procedures, type of surgical suture, and use of wrapping omental flap), operative time (minutes, mean ± SD/range, median), blood loss (mL, mean ± SD/range, median), ureteral stenting or nephrostomy positioned at the end of the procedure, conversion rates and hospitalization stay (days, mean ± SD/range, median) as well as surgical complications according to the Clavien–Dindo classification. 14
For follow-up evaluations, months of follow-up (mean ± SD/median and range), success rate, and its definition were reported.
Reporting bias assessment
The risk of bias of each included study was assessed by two review authors working independently using the ROBINS-1 15 scale for cohort studies (Supplementary Data S2).
Statistical analysis
Considering the absence of meta-analysis, only descriptive statistics were used to present the outcomes of this review both in the results section and in the tables.
Results
Study inclusion
A total of 122 publications were initially identified through database searching. Figure 1 provides a diagram of the flow of information through the different phases of this SR according to the PRISMA criteria. 13 At the end of the screening, seven studies were included in this SR. All the included studies were retrospective. IRB approval was obtained in 57.1% of cases 9,12,16,17 (Table 1).
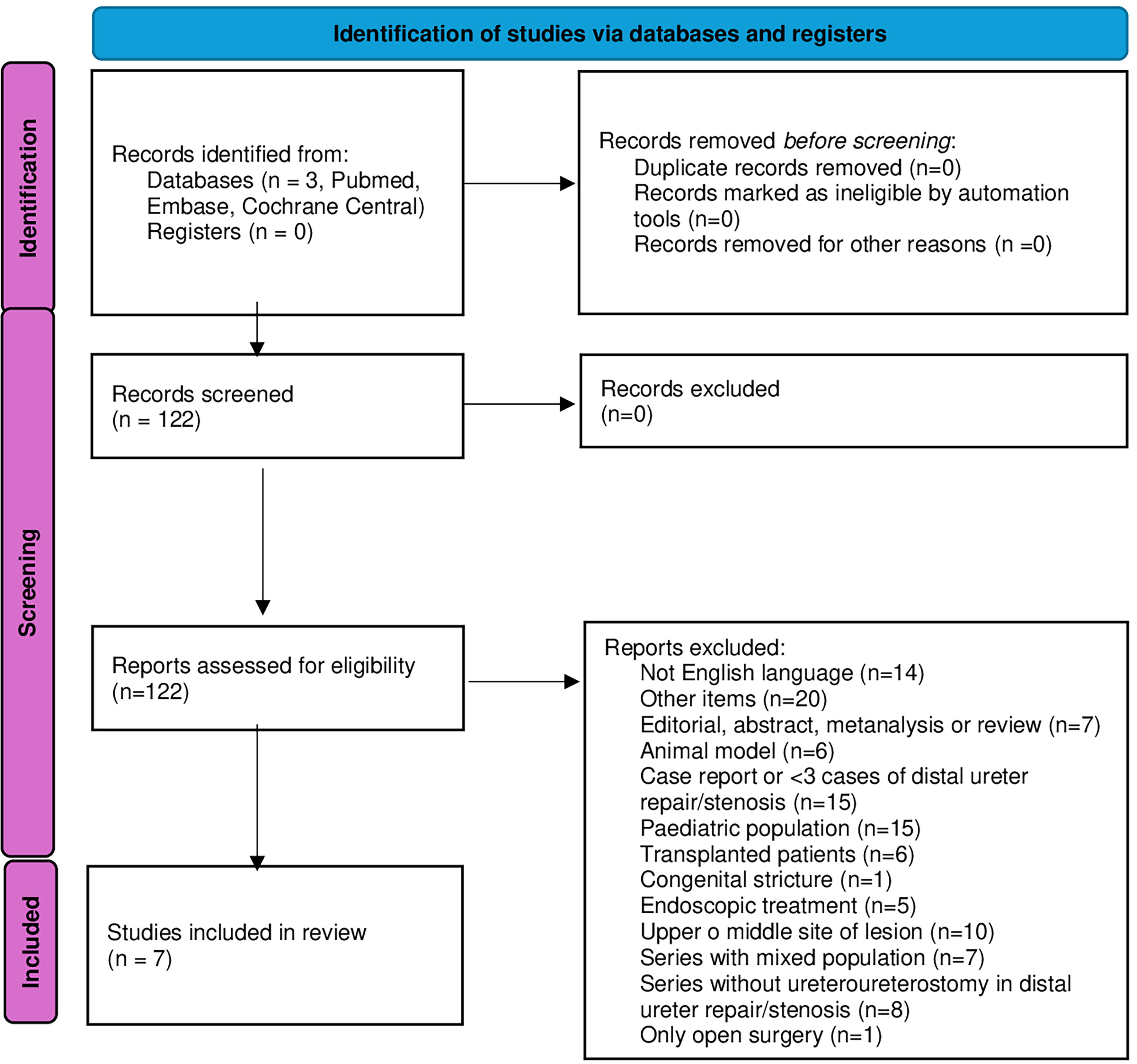
PRISMA flow chart for included study.
Studies and Patients Characteristics
Baseline characteristics
One hundred and twenty-five patients were included in the SR. Five studies (71.4%) 9,12,16,17,19 indicated the ureteral side injury or repair, and the right side was most frequently affected by this condition (27 vs 22 patients). The length of the defect was specified in three studies, 9,10,12 ranging from 1 to 4.5 cm. 10
As expected, gynecologic, urologic, and colorectal surgery were the most frequently reported causes of distal ureteral injuries/stenosis. 9,10,12,16,17,19 Only one study reported stenosis due to radiotherapy, 10 whereas another study did not indicate the cause of the distal ureteral lesion. 18 In total, 36.8% of the included patients were subjected to a previous unsuccessful treatment (endoscopic or other ureteral reconstruction). 9,10 Three studies reported the previous positioning of the nephrostomy tube 9 or double J stent. 12,16
The aforementioned data are presented in Table 2.
Baseline Characteristics
UL = ureteral lesion.
Intra, peri-, and postoperative outcomes
Table 3 summarizes all the surgical aspects of minimally invasive UU. The robotic approach was more commonly used compared with laparoscopic reconstruction (50 vs 31 patients). A single study compared the two techniques; a significant difference in favor of robotics was observed concerning operative time (mean ± SD, 126.3 ± 32.2 vs 176.6 ± 47.4) and length of hospitalization (mean ± SD, 4 ± 1.1 vs 5 ± 1.5). 18 Two studies reported the use of adjunctive techniques during robotic ureteroureterostomy (RUU) such as intravenous or intraureteral indocyanine green (ICG) injections administration. 9,10 In some studies, ureteroneocystostomy was used to repair distal ureteral defects and was compared to UU. 10,16
Surgical Aspects
UU operative time ranged from 126.3 18 minutes to 190 12 minutes in the robotic series and from 90 to 260 minutes in the laparoscopic technique. 18 The estimated blood loss (mL) was very low and ranged from 50 10 mL to 100 9 mL; two studies did not report these data. 17,18 All patients positioned a double J stent at the end of the procedure. No patients needed to convert to open surgery. The length of hospitalization was 1–11 days. 9,16
Finally, the complications of minimally invasive UU were rare and all of Grade IIIB, as reported in Table 4. Han et al. reported a higher number of complications (4 cases, 36.4%). 17
Clavien–Dindo Classification for the Postoperative Complications
In this series, the complications were reported mixed with upper and middle ureteral injuries/stenosis cases.
Follow-up Data
Follow-up data
Data on the length of follow-up was reported in all studies reaching a maximum of 59 months 17 for laparoscopic ureteroureterostomy (LUU) and up to 54.6 months for RUU. 9 An overall high success rate (>80%) of UU was reported, although the exact definition of success after UU was described in only four studies as reported in Table 5. 9,10,17,19
Discussion
To our knowledge, this is the first SR on the results of minimally invasive UU in the treatment of non-neoplastic distal ureter lesions such as iatrogenic injuries or radiotherapy-induced stenosis. 20 The surgical rules for ureteral reconstruction should be followed in UU as recommended by the international urologic guidelines. 21 The ureter must be mobilized carefully, preserving the adventitia/periureteral fat and paying attention not to damage its blood supply; also, any necrotic tissue should be resected. 22 The ureteral ends must be spatulated and the anastomosis can be performed end-to-end or side-to-side avoiding any tension, kinking, torsion, or angulation of the ureter. 7 At the end of anastomosis, an omental flap or adipose tissue may be applied to facilitate the healing process 23 and to avoid the contact of the sutured ureter with neighboring vascular or digestive structures. An internal stent and an external passive drain should be used. Concerning the stent placement, several techniques can be adopted (cystoscopic preoperative retrograde stenting, cystoscopic postoperative retrograde stenting, ureteroscopic postoperative placement, antegrade laparoscopic placement, laparoscopic antegrade placement on guidewire inserted though slit of the stent, placement on double guidewire inserted through the stent side holes); the main drawbacks of these techniques have been described in. 24 Our recently described “seagull” technique allows for a quick and safe placement of a double J stent in cases of distal ureteral lesion; it confers no risk of enlarging or tearing the ureterotomy while there is no need for patient repositioning, extra cystoscopic or ureteroscopic procedures, modified guidewires, or closed-tip stents. 24
Although LUU and RUU have emerged as viable treatment options, the literature is still limited with only two studies reporting long-term outcomes. 9 In 1992, Nezhat first reported the LUU management of an obstructed ureter, showing that LUU had a shorter hospitalization time, faster recovery, and similar outcome compared with the open approach. 25 The introduction of robotic platforms makes laparoscopic surgery easier even in the pediatric population. 26
Few studies focused on the comparison between robotic and laparoscopic approaches to UU. A comparative study confirmed significantly lower operative time and length of hospitalization for the robotic approach. 18 In a series, Schiavina et al. reported that the robotic approach may present less estimated blood loss and hospitalization time compared with the laparoscopic approach; no differences were observed in terms of perioperative outcomes, incidence of complications, or recurrence in both minimally invasive techniques. 8 In our review, the blood loss resulted in a very low range of 50–100 mL. 9,10 The length of hospitalization was 1–11 days. 9,16 Concerning the length of the stenosis, Lee et al. suggest UU for the repair of short (≤2 cm) distal strictures associated with minimal periureteral fibrosis and adequate ureteral length to obtain a tension-free anastomosis. 10 However, in this review, data regarding the length of the defect were scarcely reported and ranged from 1cm to 4.5 cm. 10
Traditionally, urologists performed UCN for the definitive surgical management of distal ureteral pathology because, in the past, open UU was associated with technical difficulty and higher failure rates because of frequent compromising of the vascular supply of the two ureteral ends. 26 The robotic approach permits the use of near-infrared fluorescence (NIRF) imaging, ICG, and Firefly™ for the identification and dissection of the stricture, potentially allowing to spare the ureteral vascularization. In particular, intraureteral ICG visualized under NIRF is useful when the identification of the ureteral dissection plane is difficult because of fibrosis, 27 whereas intravenous ICG under NIRF facilitates the preservation of the ureteral blood supply. 10,27 This aspect is very important in cases of prior failed surgery that often requires an extensive ureterolysis, which may increase the risk of ureteral devascularization and postischemic stricture recurrence.
In the included studies, limited by the small numbers of patients, postoperative complications were scarcely reported. These were more frequently represented by hydronephrosis (4 cases, Grade IIIb) treated with permanent stenting, ballooning followed by stenting, or ureteroneocystostomy. 9,17 A single patient developed a pelvic abscess (IIIb) treated with drainage. 10
In our review, UU appeared feasible and was associated with low rates of complications and good functional outcomes. 8,11 Generally, the definition of success is considered as the absence of obstruction on computed tomography urography or renal ultrasonography and absence of obstructive symptoms (flank pain and recurrent urinary tract infections), while diuretic renal scintigraphy has been rarely adopted to confirm the resolution of ureteral obstruction. 10 In this review, the success rate of minimally invasive UU was very high, ranging from 81.8% to 100%.
Limitations of the included studies and of the SR
Short follow-up duration:
Many of the studies lack long-term follow-up data, which limits the ability to assess the durability of outcomes and potential for late-onset complications after minimally invasive UU. Only two studies in this review provide extended follow-up data,
9,17
which further limits the ability to evaluate the durability of outcomes, and the risk of late-onset complications associated with minimally invasive UU. Retrospective design:
All seven studies included in the review are retrospective in nature, which may introduce biases such as selective reporting and inconsistent data collection, impacting the reliability of findings. Patient population and selection bias:
The patient population analyzed within this review originates from specialized referral centers, potentially introducing selection bias. This limitation may restrict the generalizability of findings to wider patient populations and clinical settings. Sample size:
The overall sample size across the studies remains small, with a combined total of approximately 116 patients. This low number limits the statistical power of the review and reduces the confidence with which conclusions can be drawn.
Summary of the findings and future research
Minimally invasive UU emerges as an effective treatment for non-neoplastic distal ureteral lesions, demonstrating low complication rates and high success when performed in carefully selected patients. There is a rising need for larger, prospective studies evaluating long-term outcomes of UU for distal ureteral lesions; such studies will be essential for better understanding the full potential of this approach and for establishing broader guidelines for its use as an alternative (or even first-line treatment) to ureteral reimplantation.
Conclusions
Minimally invasive UU may represent a viable treatment option for the treatment of non-neoplastic distal ureter pathology. It is feasible, with a low risk of complications and a high success rate in selected patients, although long-term follow-up data are still scarce. Larger, prospective studies adopting a standard definition of the postoperative success are required to affirm UU as a first-line option in the management of benign distal ureteral lesions.
Footnotes
Authors’ Contributions
E.R. data collection and management, data analysis, article writing/editing. R.M. data analysis. L.O. data analysis. T.P. data analysis, critical revision. R.G. data analysis, critical revision. A.D.A. protocol/project development, data collection and management, data analysis, article writing/editing.
Author Disclosure Statement
No conflicts of interest for the authors.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.