
Abstract
Background:
Complete removal of urinary stones remains a challenge, as residual fragments can contribute to recurrence and postoperative urinary tract infections. This study presents an initial laboratory investigation into the development of an alginate gel composite designed to bind calcium-based stone remnants and exhibit antibacterial properties.
Methods:
To evaluate gel formation, calcium oxalate powder reagent and sodium alginate (SA) powder reagent were mixed in a Becker glass and stirred on a hot plate. Stones from 17 patients who underwent stone surgery were crushed, and gel formation was confirmed using the same experimental conditions with SA powder reagent. A gel composite material containing silver nitrate and vancomycin was prepared, and antibacterial activity against Staphylococcus aureus and Escherichia coli was tested over a 5-minute period. A mixture of 0.5 g alginic acid and 0.05 g calcium oxalate monohydrate powder reagent with 50 mL distilled water formed a gel after 30 minutes.
Results:
Sandy stones composed of calcium oxalate formed a better gel composite when mixed with SA than those composed of uric acid. In the antibacterial test of the alginate gel composite containing silver nitrate and vancomycin against S. aureus and E. coli, the number of live bacteria in the control and alginate gel composite was 3.5 × 103 and <10, respectively.
Conclusion:
This study represents a preliminary laboratory investigation into the development of an alginate gel composite for potential use in urinary stone management. Further preclinical studies are necessary to evaluate its efficacy and safety before clinical translation.
Introduction
Urinary stone disease is one of the most common benign diseases in urology. It is among the most important diseases affecting morbidity, with a prevalence rate of 7%–15% in North America, 5%–9% in Europe, and 1%–5% in Asia, with the trend increasing every year. 1 –3
More than 80% of stones are calcium-based, such as calcium oxalate or calcium phosphate, whereas other stones include uric acid, struvite, and cysteine. 4 Most urinary stones that cannot be removed using conservative treatment or extracorporeal shockwave lithotripsy can be surgically removed. 5,6 Surgical methods include percutaneous nephrolithotomy or rigid and flexible ureteroscopy/retrograde intrarenal surgery (RIRS), depending on the size and location of the stones. 7 –10 The stones were fragmented using a laser and removed by holding them in a stone basket. 11 However, it is difficult to completely remove finely broken sandy stones. 12,13 In addition, urinary tract infections due to bacterial spread during the process of dusting stones can become fatal complications after surgery. 14,15 The recurrence of stones due to residual stones is common, resulting in increased retreatment costs. 16 –18 Accordingly, there is an urgent need to develop a treatment method that can completely remove residual kidney and ureter stones and prevent postoperative urinary tract infections with low development and treatment costs.
The most important goal of stone surgery is complete stone removal while minimizing recurrence. Various novel approaches and techniques have been studied to enhance the removal of residual stones. The most common and widely used method is mechanical extraction via stone baskets; however, this approach has limitations in removing smaller fragments. 19,20 Suction-based techniques utilizing ureteral access sheaths have also been explored, although challenges such as pressure management remain. 21 –23 In addition, emerging research has investigated the feasibility of magnetic extraction using iron oxide particles. 24 –28 These previous studies highlight the ongoing need for innovative approaches to optimize stone clearance and improve patient outcomes.
Alginic acid (sodium alginate [SA], Na·(C6H8O6)n) is a naturally abundant polysaccharide fiber component that accounts for 20%–30% of brown algae, such as seaweed and kelp, and has various clinical applications but no application in the urologic field. 29 –33 In materials containing calcium ions (Ca2+) with low solubility, alginic acid combines with calcium ions to form a gel-like precipitate that is insoluble in water. 29,32,33 Therefore, a gel composite combining alginic acid and calcium-based sandy stone remnants after lasing may facilitate complete removal with a stone basket. In addition, to prevent urinary tract infections caused by bacterial spread due to stone fragmentation and the dusting process, it is crucial to create an alginate gel composite with antibacterial properties.
In this study, we developed and applied an alginate gel composite with antibacterial properties that could bind to sandy stone remnants to completely remove fine stones and prevent postoperative tract infections.
Materials and Methods
Study design
This study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review board of
Preparation of alginate gel composite using powders
Using SA powder reagent and distilled water, we prepared solutions of 0.5, 1, 1.5, and 4 g SA with 50 mL of distilled water. These mixtures were stirred for 30 minutes on a 36.5°C hot plate using a stirring bar. Similarly, solutions containing 0.05, 0.1, and 0.2 g calcium oxalate monohydrate powder reagent with 50 mL distilled water were prepared and stirred for 30 minutes under the same conditions. The two prepared materials were then combined and stirred on a 36.5°C hot plate in a fume hood for 30 minutes to 12 hours to confirm the formation of a hard gel composite with various concentrations. Furthermore, we prepared 0.1 g β-TCP by mixing β-TCP powder reagent with 50 mL distilled water and then mixed it with various concentrations of SA to confirm gel composite formation in a similar manner. In addition, 0.05 g of uric acid was prepared using uric acid powder reagent and 50 mL of distilled water. This was then mixed with various concentrations of SA, and gel composite formation was confirmed in the same manner.
Preparation of alginate gel composite using stones of patients
Stone fragments formed from 100% calcium oxalate stones were washed with distilled water for 30 minutes and then dried in a dryer at 37°C for 24 hours. Subsequently, they were finely ground to form sandy stones. To confirm the formation of the alginate gel composite, we mixed 4 g of SA powder reagent with 50 mL distilled water and 0.5 g of 100% calcium oxalate sandy stones from the patient. The mixture was then placed on a 36.5°C hot plate in a fume hood and stirred for 30 minutes using a stirring bar. Gel formation was confirmed. The same process was performed for 100% uric acid stone fragments obtained from all patients.
Preparation of alginate gel composite containing antibacterial property
To manufacture an alginate gel composite with antibacterial properties, three samples of alginate gel composite were prepared using the same method: calcium oxalate sandy stones from the patient, SA powder reagent, silver nitrate powder reagent, and vancomycin. The control group was a sample without the alginate gel composite with silver nitrate. Sample #1 was prepared by mixing 0.5 g of SA, 0.5 g of patient-derived sandy stones, and 0.5 g of silver nitrate with 50 mL of distilled water on a hot plate at 36.5°C for 30 minutes, forming an alginate gel composite. Similarly, Sample #2 used the same quantities of SA and sandy stones but increased the silver nitrate to 1.0 g. Sample #3 was also an alginate gel composite, created with 0.5 g of SA, 0.5 g of sandy stones, 1.0 g of silver nitrate, and 0.1 g of vancomycin (product No. SBR00001, purity ≥95%; Sigma-Aldrich) under identical conditions.
Antibacterial in vitro test
For the in vitro antibacterial test against the manufactured alginate gel composite with calcium oxalate sandy stones of a patient containing silver nitrate, two strains of gram-positive Staphylococcus aureus (ATCC 6538) and gram-negative Escherichia coli (ATCC 8739) were used.
34
–36
The two bacterial strains were transferred to a solid medium and cultured at 37.0°C for 24 hours. Activated bacteria were inoculated into a liquid medium and incubated overnight at 37.0°C. The concentrations of the bacterial solutions for S. aureus (ATCC 6538) and E. coli (ATCC 8739) were 3.5 × 103 colony forming units (CFU)/mL and 4.2 × 103 CFU/mL, respectively. The reaction time between the bacteria and samples was 5 minutes. The bacterial reduction rate (RRB, %) was calculated using the following formula
36
:
Results
Figure 1 illustrates the gel morphology resulting from various ratios of alginic acid to calcium oxalate monohydrate. Figure 1D demonstrates that mixing 1.5 g of alginic acid with 0.2 g of calcium oxalate under similar conditions for 4 hours resulted in a small amount of gel-like precipitate. These observations indicate that lower concentrations of the reagents increase the gel formation time, whereas higher concentrations and shorter heating durations promote gel formation.
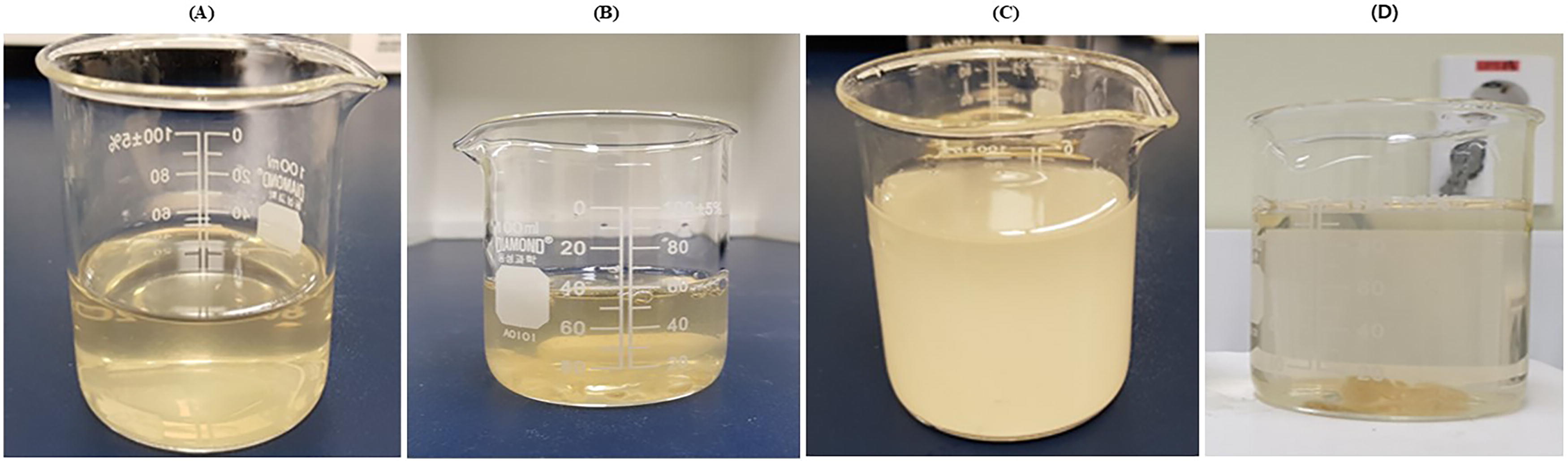
Gel formulated using different ratios (including water) of materials, including alginic acid and calcium oxalate monohydrate powder reagents.
Figure 2 illustrates the optimal gel formation using alginic acid and calcium oxalate monohydrate. Figure 2A shows that mixing 4 g of alginic acid with 0.2 g of calcium oxalate monohydrate in 50 mL of distilled water at 36.5°C for 30 minutes with stirring resulted in a yellow jelly-like alginate gel composite. The composite was formulated by mixing: (1) 0.15 g calcium oxalate monohydrate and 0.25 g SA in 50 mL distilled water at 36.5°C for 12 hours; (2) 0.1 g β-TCP and 0.25 g SA in 50 mL distilled water at 36.5°C for 12 hours; or (3) 0.05 g uric acid and 0.25 g SA in 50 mL distilled water at 36.5°C for 12 hours. Lower reagent concentrations increased the gel formation times.
Gel formed using an optimal proportion of alginic acid and calcium oxalate monohydrate powder reagent.
To create an alginate gel composite using patient stones, we reviewed the clinical information of 17 registered patients (Table 1). The surgical methods used were percutaneous or RIRS, depending on the stone size and location. The most common stone component was calcium oxalate monohydrate, followed by uric acid, struvite, and carbonate apatite.
Clinical Information of the Patients Enrolled in This Study
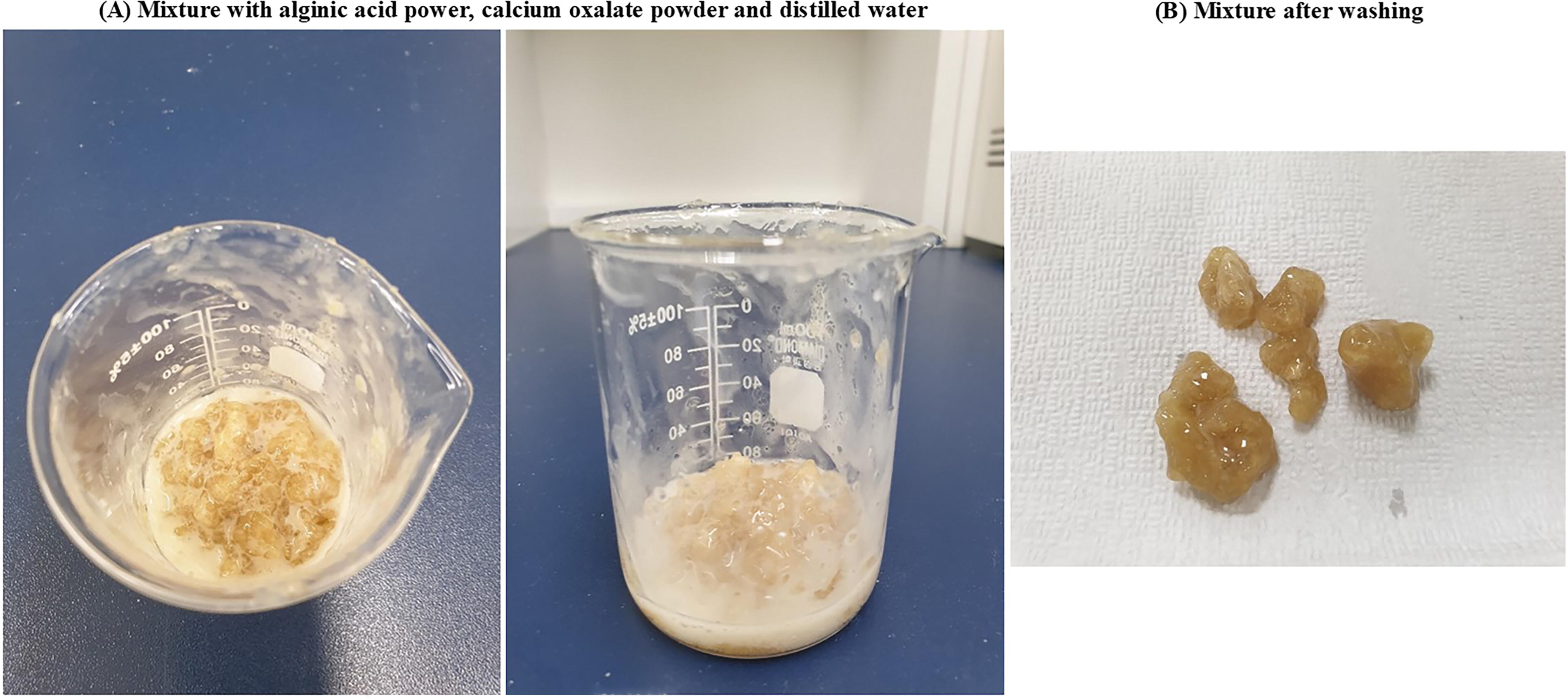
Figure 3 illustrates gel formation from mixtures of alginic acid powder and patient stones. Figure 3A presents gross images of stones composed of 100% calcium oxalate (brown and hard) and 100% uric acid (yellow and relatively softer). Figure 3B shows the sandy stone remnants obtained after grinding the stones for 5 minutes. Figure 3C shows the alginate gel composite prepared by mixing each 0.5 g sandy stone and 4 g SA powder reagent with 50 mL distilled water heated on a 36.5°C hot plate for 30 minutes. Calcium oxalate stones form a more viscous gel composite than uric acid stones. In addition, in the case of struvite and apatite stones, the alginate gel composite was effectively formed, similar to calcium oxalate and uric acid stones.

Gel was prepared using a mixture of alginic acid and stones from patients.
Figure 4 shows the gross images after antibacterial testing of the alginate gel composite with calcium oxalate sandy stones containing silver nitrate and vancomycin using S. aureus and E. coli for 5 minutes. Compared with the control (no alginate gel composite with silver nitrate), the two strains of bacteria were almost eliminated in samples #1, #2, and #3, suggesting strong antibacterial activity.
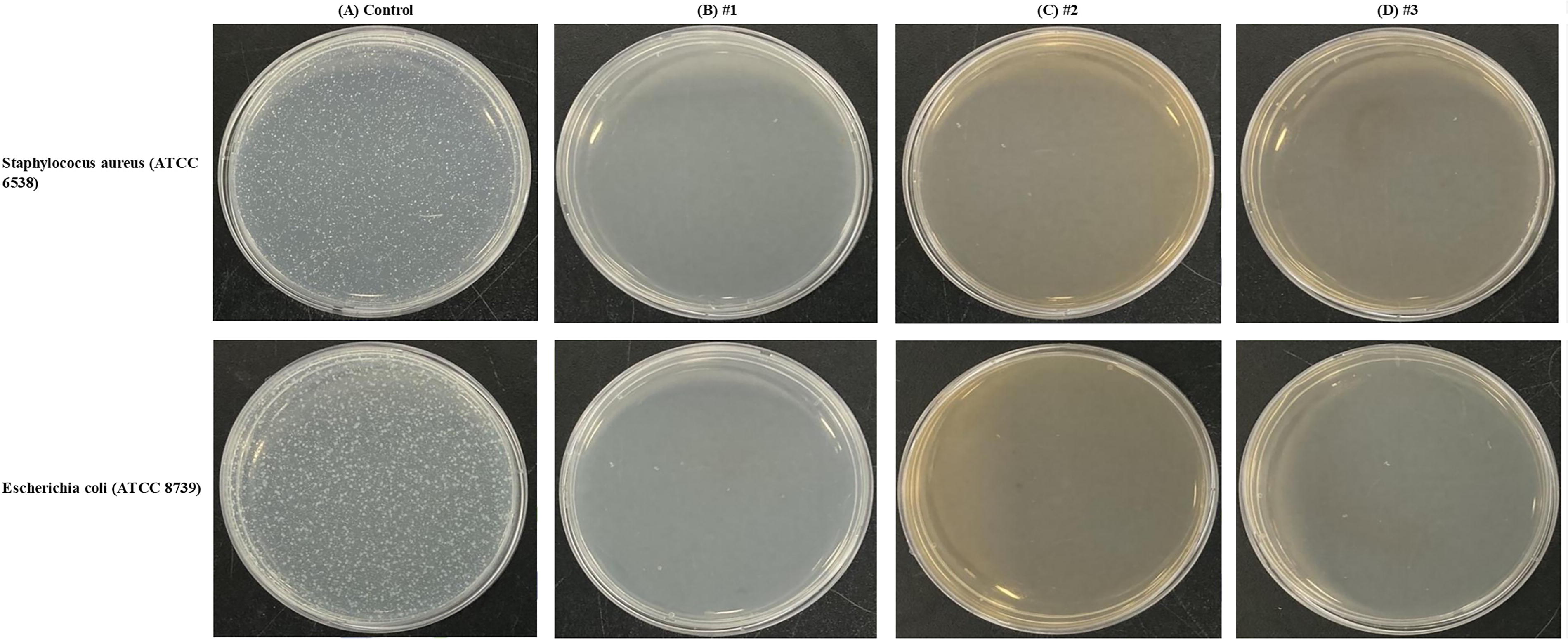
Antibacterial testing of alginate gel composite with calcium oxalate sandy stones from a patient containing silver nitrate against Staphylococcus aureus and Escherichia coli for 5 minutes.
Table 2 shows the quantitative analysis of the antibacterial test of the alginate gel composite with calcium oxalate sandy stones containing silver nitrate and vancomycin using S. aureus and E. coli for 5 minutes. Compared with the control, there were <10 live bacteria in all three samples, indicating strong antibacterial activity.
Quantitative Analysis of the Antibacterial Test of the Alginate Gel Composite with Calcium Oxalate Sandy Stones of Patients Containing Silver Nitrate Using Staphylococcus aureus and Escherichia coli for 5 Minutes
Control: no alginate gel composite with silver nitrate, #1: a mixture of 0.5 g sodium alginate, 0.5 g sandy stones of a patient, and 0.5 g silver nitrate mixed in 50 mL distilled water heated on a 36.5°C hot plate for 30 minutes, #2: a mixture of 0.5 g sodium alginate, 0.5 g sandy stones of a patient, and 1.0 g silver nitrate mixed with 50 mL distilled water heated on a 36.5°C hot plate for 30 minutes, #3: 0.5 g sodium alginate, 0.5 g sandy stones of a patient, 1.0 g silver nitrate, and 0.1 g vancomycin mixed with 50 mL distilled water heated on a 36.5°C hot plate for 30 minutes.
CFU = colony forming unit.
Discussion
The primary objective of stone surgery is to achieve complete stone clearance and reduce recurrence rates. To this end, various techniques have been explored to enhance the removal of residual stone fragments. Mechanical extraction via stone baskets remains the standard method, although it is less effective for fragments smaller than 2 mm. 19,20 Suction-based approaches using traditional or modified ureteral access sheaths have been investigated, but they present challenges related to pressure regulation. 21 –23 More recently, studies on magnetic retrieval using iron oxide microparticles or magnetic probes have demonstrated promising preliminary results. 24 –28 By building on these prior innovations, our study seeks to explore a new approach using an alginate gel composite to facilitate stone entrapment and removal.
This was a preliminary study that developed and applied an alginate gel composite with antibacterial properties to completely remove sandy stone remnants of the kidney or ureter that are difficult to remove surgically and to prevent fatal urinary tract infections that may occur after surgery.
Alginic acid is a fibrous component that constitutes a significant portion of brown algae, such as seaweed and kelp, and naturally becomes mushy and slippery when added to water. 29 –33 Alginic acid is a polysaccharide composed of two uronic acids (mannuronic acid and l-guluronic acid), and its properties can vary depending on the ratio of the two components (Supplementary Fig. S1). Alginic acid with a large ratio of the two components forms an elastic gel, whereas alginic acid with a small ratio forms a hard and brittle gel. 29 –33 Although alginic acid has a hydrophilic hydroxyl group (–OH), it contains a large number of carbon atoms and has a high molecular weight, making it difficult to dissolve in water (Supplementary Fig. S1). However, when alginic acid becomes an anion, its solubility increases because the hydrogen atom of the carboxyl group (–COOH) present in alginic acid breaks down and becomes –COO–, indicating a strong affinity for water (Supplementary Fig. S1). Therefore, all alginic acids present in nature exist in the form of anions. 29 –33 If alginic acid contains sodium ions (Na+) or potassium ions (K+) with high solubility, it dissolves well in water. However, when it contains calcium ions (Ca2+) with low solubility, it combines with calcium ions and does not dissolve in water, forming a gel-like precipitate. 29 –33 Currently, various types of alginate composites are being used to develop substitute materials for bone and cartilage regeneration and are being researched and developed for application in various bone tissue engineering fields. 29,31,32 In particular, studies on bone-repair composite microspheres composed of calcium phosphate/SA/polymer complexes and their drug-releasing properties have recently been reported. 33 In addition, β-TCP powder was prepared and dissolved in an SA solution to create a β-TCP/SA suspension. When this solution was dropped into a calcium chloride solution, calcium was replaced with alginate to form microspheres. In addition, because gentamicin and vancomycin are water-soluble antibiotics, if they are used as solvents to dissolve SA, a complex containing antibiotics can be produced. 33 Therefore, if alginic acid is combined with finely ground calcium-based stones to form a gel, it can be easily removed. Moreover, if antibiotics or metal ions with antibacterial properties are substituted, a gel with antibacterial properties is formed, which effectively prevents urinary tract infections that occur after stone surgery.
Supplementary Figure S2 illustrates the approach to the kidney using a flexible nephroscope, stone fragmentation using a holmium laser, and stone removal using a stone basket. Kidney and ureter stone surgery uses a flexible scope, as shown in Supplementary Figure S2A, and removes them with a stone basket after stone fragmentation and dusting using a holmium laser, as shown in Supplementary Figure S2B. However, complete stone removal is difficult, and residual stones remain, causing future recurrence. 16 In addition, during surgery, stones contaminated by bacteria from a urinary tract infection are broken into small pieces using a holmium laser, which spreads the bacteria. 14,15 Therefore, we investigated a method that can completely remove stone debris and prevent postoperative urinary tract infections. Supplementary Figure S3 shows a conceptual illustration of remnant stone removal by creating a gel composite of sandy stones with alginic acid, which has antibacterial properties. When alginate with silver ions and calcium-based sandy stone remnants combine to form alginate gel composites, they can be removed using stone baskets. This technology offers advantages such as not requiring specialized equipment for development, having low development costs, and shortening surgical time for stone removal. Aiding in the complete removal of residual stones may reduce the need for repeated use of equipment such as endoscopes, thereby decreasing equipment failures and extending maintenance and replacement intervals. This, in turn, could lower costs associated with surgical equipment and consumables. In addition, by minimizing residual stones, this approach may reduce postoperative recurrence, ultimately decreasing both the initial treatment cost of urinary stones and the cost of retreatment.
This study had some limitations. Initially, we used alginic acid, a marine-derived biopolymer that has not been previously used in urologic applications, to develop a novel material. While this study demonstrated the feasibility of using an alginate gel composite for stone entrapment, it did not include a comprehensive analysis of key physicochemical properties, such as size, consistency, and remnant production. These characteristics are essential for optimizing the material for clinical use in endoscopic stone surgery. To address this gap, future studies will focus on synthesizing composites with varied compositions and systematically evaluating their physicochemical behavior in preclinical settings. In this study, we selected E. coli, the most common pathogen in urinary tract infections, and S. aureus, an important pathogen associated with antimicrobial resistance. Although S. aureus is not a typical genitourinary pathogen, it is more frequently isolated in patients with severe urinary tract infections, particularly those with long-term catheterization, urologic abnormalities, or comorbidities. In follow-up studies, we plan to conduct antibacterial tests on additional genitourinary pathogens, including Klebsiella, Proteus, and Pseudomonas aeruginosa. Due to experimental constraints, antibacterial tests could not be conducted on all samples. Therefore, the experiment focused on calcium oxalate stone samples, as they were the most frequently collected. In future research, we plan to extend antibacterial testing to a wider range of stone compositions by applying various bacterial strains. In this study, most of the collected stones were composed primarily of calcium oxalate monohydrate, which does not fully reflect the real-life distribution of urinary stone compositions. This was due to patient consent requirements and the need to obtain sufficient stone material for analysis. Future studies will aim to include a larger and more diverse patient cohort to ensure a representative range of stone compositions, improving the generalizability of the findings. Standardizing the formation of alginate gel composites in a clinical setting remains a key challenge, as factors such as temperature and composition ratios influence gel consistency and usability. To address this, we plan to conduct in vitro and in vivo studies to optimize the formulation by systematically varying these parameters and assessing the physicochemical properties of the resulting composites. In addition, future research should include cytotoxicity and hemolysis assays to evaluate biocompatibility. Feasibility studies and product development efforts will also be necessary to explore potential clinical applications and commercialization pathways.
Conclusions
This study was a preliminary laboratory investigation demonstrating the feasibility of using an alginate gel composite to bind residual urinary stone fragments and exhibit antibacterial properties. Although these findings provide a foundation for future research, a significant gap remains between laboratory studies and clinical applications. Further preclinical studies are required to assess efficacy, safety, and feasibility before potential clinical implementation.
Footnotes
Acknowledgment
The authors acknowledge the research support team at Pusan National University Yangsan Hospital.
Authors’ Contributions
Conceptualization: W.H.S. Methodology: W.H.S., S.S.L., and J.K.N. Investigation: J.K.N. and S.W.P. Resources: W.H.S. and S.S.L. Data curation: W.H.S. Writing—original draft preparation: W.H.S. Writing—review and editing: W.H.S. and S.-W.P. Supervision: S.-W.P. All authors have read and agreed to the published version of the article.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research was supported by a 2024 research grant from Pusan National University Yangsan Hospital.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.