
Abstract
Objective:
Ureteroscopic lithotripsy (URSL) is the main method for treating ureteral calculi. The scholars used ureteroscopes with dual channels and access sheath to reduce the local temperature and flushing fluid pressure. This study compares the efficacy and safety of ureteral catheter-assisted URSL (UCA-URSL) and traditional URSL in treating ureteral calculi.
Patients and Methods:
A cross-regional retrospective case–control study in China, including 217 intention-to-treat patients from the First Affiliated Hospital of Kunming Medical University and Tongji Hospital Affiliated to Tongji Medical College of Huazhong University of Science and Technology, from August 2023 to July 2024. The primary outcome was the temperature of the lithotripsy point. The secondary outcomes included stone-free rate (SFR), operation time, hospital stay, and postoperative complications.
Results:
Compared with the traditional URSL group, the catheter-assisted URSL group had a significantly lower lithotripsy point temperature (max, 37.9 ± 2.60°C vs 49.98 ± 5.04°C, p < 0.0001; mean, 32.3 ± 3.25°C vs 38.56 ± 2.70°C, p < 0.0001). In addition, the UCA-URSL group showed higher absolute SFR (immediately, 89.81% vs 53.21%, p < 0.0001; 3 months, 99.07% vs 72.48%, p < 0.0001), and reduced operation time (22.74 ± 7.08 minutes vs 26.40 ± 6.72 minutes, p = 0.0001), postoperative fever rate (1.85% vs 15.60%, p = 0.0003), and ureteral stricture rate (0% vs 3.67%, p = 0.04).
Conclusions:
In treating ureteral calculi, UCA lithotripsy shows better safety than traditional URSL. Catheter-assisted URSL can be used to improve traditional URSL.
Introduction
Urolithiasis is one of the most prevalent urinary diseases worldwide, with an incidence of 1%−5% in Asia and 7%−13% in North America. 1 According to the European Association of Urology (EAU) guidelines, both ureteroscopic lithotripsy (URSL) and extracorporeal shockwave lithotripsy (SWL) can be used as the first choice for the treatment of ureteral stones 2 because of their high stone-free rate (SFR). However, to achieve the goal of complete stone clearance, SWL requires multiple repeated treatments and a longer follow-up period, thereby increasing the total duration of treatment. URSL is more reliable in obtaining early SFR but also has the potential risk of causing serious complications. Compared with SWL, some studies have shown that URSL has better overall clinical outcomes than SWL. 3 The holmium:yttrium aluminum garnet (Ho:YAG) laser is the most effective laser lithotripsy system. It is currently the best choice for URSL 2,4 because it is effective for all types of stones. The Ho:YAG laser lithotripsy mechanism depends on its photothermal effect, which causes the rupture of stones through the vacuolization and expansion of water molecules inside the stones. 5 However, laser excitation causes a significant increase in its surrounding temperature, which may lead to tissue solidification, carbonization, and denaturation. 6 In extreme cases, local thermal energy at the lithotripsy point can lead to irreversible damage to the ureteral tissue, resulting in ureteral stenosis. 7 Once ureteral stricture occurs, except for the surgical effect of ureteroplasty being recognized, the efficacy of other treatment methods is still uncertain. It is necessary to take effective measures to optimize the key steps of URSL to reduce the incidence of postoperative ureteral stricture.
Traditional URSL has limited efficacy in achieving an SFR and sometimes requires multiple operations or conversion to flexible URSL. In addition, when handling large stones, it is difficult to control the intrarenal pressure in the traditional operation, and serious complications may occur, which poses a major challenge to traditional URSL. In the previous study of the in vitro model, our team found that the new water circulation system assisted by a catheter can reduce the thermal effect of URSL, renal pelvic pressure, and stone displacement rate, at the same time, the system can also improve the clarity of lithotripsy field. 8 Continuing our previous study, we conducted a clinical study to compare the efficacy and safety of UCA-URSL and conventional URSL in treating ureteral calculi.
Methods
Trial design and participants
This was a retrospective case–control study conducted in the Urology Department of two hospitals, with approximately more than 400 URSL procedures performed annually at each participating center. Patients who were diagnosed with ureteral calculi and had undergone semirigid URSL in the Department of Urology of the First Affiliated Hospital of Kunming Medical University and Tongji Hospital of Tongji Medical College of Huazhong University of Science and Technology from August 2023 to July 2024 were selected. The inclusion and exclusion criteria are shown in Table 1. The operation was completed by skilled urologists. A total of 217 patients were included. The subjects were divided into a UCA-URSL group and a traditional URSL group according to whether they used catheter assistance during surgery. A total of 163 cases (83 cases in the UCA-URSL group, 80 cases in the traditional URSL group) from the First Affiliated Hospital of Kunming Medical University and 54 cases (25 cases in the UCA-URSL group, 29 cases in the traditional URSL group) from the Tongji Hospital of Tongji Medical College of Huazhong University of Science and Technology were included. The preoperative data, the temperature of the lithotripsy area during the operation, surgical field clarity, the success rate of one-stage operation, operation time, hospitalization time, SFR (immediately and 3 months), and postoperative complications (Clavien–Dindo) were compared between the two groups.
The Inclusion and Exclusion Criteria
Procedures and quality control
The patients were numbered according to the admission sequence number, and then they were divided into the UCA-URSL group and the traditional URSL group by random number table method. All patients underwent a 2-mm slice-thickness noncontrast CT scan before the operation. The same software was used to measure stone size and density in both centers. Patients with negative urine routine tests and cultures were given standard perioperative antibiotic prophylaxis 30 minutes before surgery. Patients with positive urine cultures before surgery were treated with appropriate antibiotics according to the results of drug sensitivity. All procedures were performed by one designated experienced surgeon (≥100 cases per year in traditional URSL). Before all procedures, the thermocouple (T-couple, 0.05 mm, KAIPUSEN) was passed through the inside of the ureteral catheter (F4, 45 cm in length) to be flushed with the front of the ureteral catheter (Fig. 1). The thermocouple was connected to the thermometer (KAIPUSEN), and the temperature data were set to be collected every 3 seconds. The operation was performed in the lithotomy position under general anesthesia. Before ureteroscopic implantation, a 10–12F catheter was placed into the bladder for drainage. After the stone was located by the ureteroscope, the laser fiber (200 μm, Raykeen) and the ureteral catheter were sent through the ureteroscope to reach the ureteral lens end with the thermocouple. The end of the ureteral catheter in the UCA-URSL group was left open, and the end of the ureteral catheter in the traditional URSL group was closed (sealed with sterile tape). All patients were treated with room temperature 0.9% sodium chloride solution during the operation and the flushing flow rate was 100 mL/min. Lithotripsy was performed under an 8/9.8F (single channel) ureteroscope with a holmium laser (1 J/20 Hz) (Supplementary Videos S1 and S2). The ureteral catheter is not always unobstructed during the operation, and its obstruction is often because of the blockage of stone particles/powder. The patency of the ureteral catheter was comprehensively judged by observing the continuity of the outflow of the catheter and the change of the clarity of the surgical field. When the catheter is blocked, we choose to replace it with a new catheter. After the stone was crushed, the ureter was checked for damage, and the residual stone was evaluated for returning to the kidney. The equipment was withdrawn after the satisfactory intraoperative effect, and the Double-J stent (D-J, F6, Cook) was placed under the guidance of the guidewire. An abdominal noncontrast CT scan (with 2 mm cuts) examination was performed within 24–48 hours after operation to evaluate the immediate SFR. Blood routine and urine routine were used to monitor the infection within 2–6 hours after the operation. Patients were discharged the following postoperative day if they had no apparent discomfort. F6 D-J stent was implanted for 2–4 weeks. All patients underwent noncontrast CT scan (with 2 mm cuts) reexamination at 3 months of follow-up. General information, treatment-related information, and follow-up information were collected.
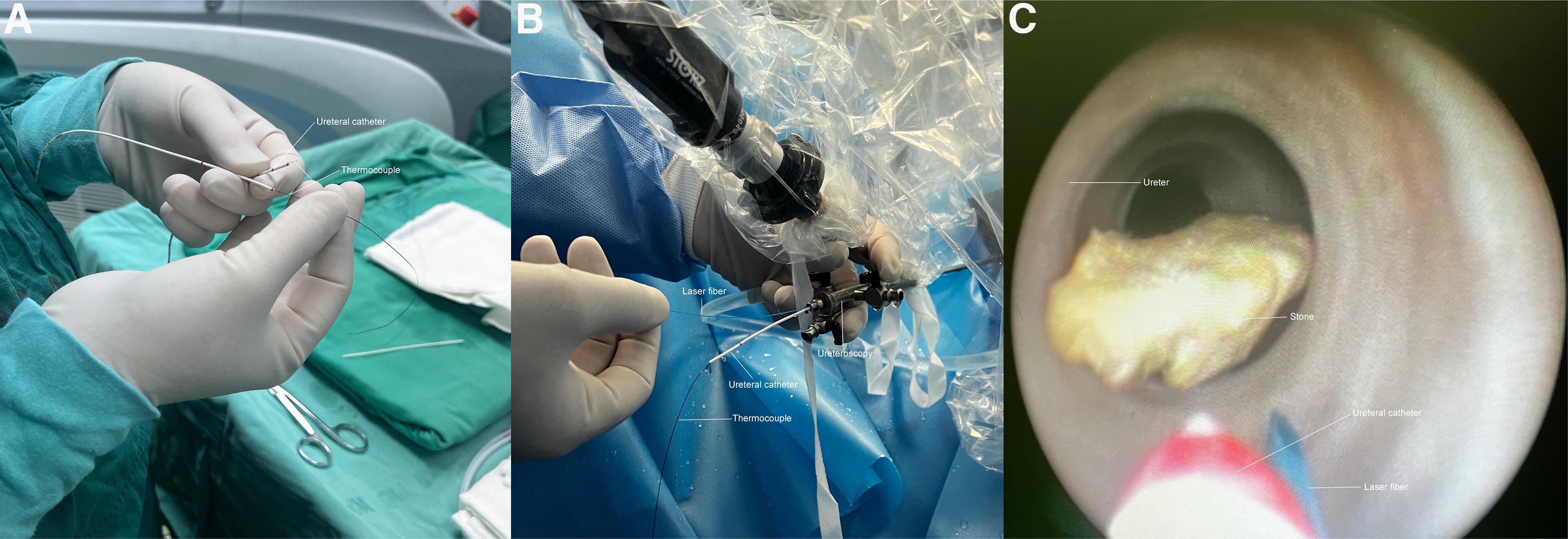
Surgical procedure of UCA-URSL.
Outcomes
The primary endpoint of the study was the intraoperative lithotripsy point temperature, the secondary indicators included SFR (immediately and 3 months), and stone-free data will be classified into three grades by noncontrast 2-mm slice-thickness CT scan: Grade A (absolute stone-free, no stones), Grade B (relative stone-free, ≤2 mm fragments), and Grade C (relative stone-free, 2.1–4 mm fragments), operation time, hospital stay, auxiliary surgery, and postoperative complications. Patient characteristics and clinical outcomes were recorded on case report forms. Stone size was defined as the maximum diameter of a single stone and the sum of the maximum diameters of multiple stones. The operative time was the time from the endoscope insertion into the urethra to the completion of stent placement. Fever was defined as a persistent body temperature >38.5°C, and septic shock was diagnosed based on clinical criteria of persistent hypotension requiring vasopressor therapy to maintain mean arterial pressure ≥65 mm Hg and serum lactate level ≥2 mmol/L despite adequate fluid resuscitation.
Statistical analysis
SPSS 20.0 was used for statistical analysis. Measurement data were expressed as mean ± standard deviation, and continuous variables with normal distribution were expressed as mean (standard deviation). An independent t-test was used for comparison between groups. Categorical variables were expressed as rates and percentages and analyzed using Fisher’s exact test or chi-square test. A p-value of less than 0.05 was considered statistically significant.
Results
Patient recruitment and baseline characteristics
Among the 230 eligible patients, 6 patients in the UCA-URSL group and 7 patients in the traditional URSL group were treated with a 6/7.5F semirigid ureteroscope (4F catheter could not be inserted) instead of an 8/9.8F ureteroscope because of the thinner ureters. After subtracting the 13 patients excluded for not using the 4F catheter, all patients were included in the analysis. A total of 108 patients in the UCA-URSL group and 109 patients in the traditional URSL group were included in the study. Table 2 summarizes the demographic data (gender, age, body mass index [BMI]), stone location, size, and stone density. Overall, there were no significant differences in demographics, stone location and characteristics, or preoperative infection rates among the enrolled patients (Table 2).
Procedure-Related Characteristics
BMI = body mass index; CI = confidence interval; HU = Hounsfield unit, a unit of CT value that is used to quantify the radiation density of different tissues; UCA-URSL = ureteral catheter-assisted URSL; URSL = ureteroscopic lithotripsy.
The UCA-URSL group had a lower lithotomy point temperature than the traditional URSL group (maximum temperature, 37.9 ± 2.60°C vs 49.98 ± 5.04°C, 95% confidence interval [CI] 10.84 to 13.30, p < 0.0001; mean temperature, 32.3 ± 3.25°C vs 38.56 ± 2.70°C, 95% CI 5.337 to 7.177, p < 0.0001) (Table 3). Compared with the traditional URSL group, the UCA-URSL group had a higher absolute SFR (Grade A: immediately, 89.81% vs 53.21%, p < 0.0001; 3 months, 99.07% vs 72.48%, p < 0.0001). The proportion of patients with Grade B (≤2.0 mm fragments) and Grade C residual stones (2.1–4.0 mm fragments) in the UCA-URSL group was significantly lower than that in the traditional URSL group, and the probability comparison was Grade B (immediately, 10.19% vs 27.52%, p = 0.0011; 3 months, 0.93% vs 15.60%, p < 0.0001) and Grade C (immediately, 0% vs 19.27%, p < 0.0001; 3 months, 0% vs 11.93%, p < 0.0001) (Table 3). Three patients in the traditional URSL group underwent flexible ureteroscopy because of large (>5 mm) stone escape (two cases in the first stage and one case in the second stage). The probability of surgical procedure replacement (patients undergoing flexible ureteral lithotripsy) in the traditional URSL group was higher than that in the UCA-URSL group (2.75% vs 0%, p = 0.08), although the statistical difference was not shown (Table 3). The UCA-URSL group had a certain advantage in the operation time (22.74 ± 7.08 minutes vs 26.40 ± 6.72 minutes; 95% CI 1.808 to 5.518; p = 0.0001). There was no significant difference in the length of hospital stay between the two groups (4.52 ± 2.41 days vs 4.47 ± 2.18 days; 95% CI −0.6583 to 0.5754; p = 0.89) (Table 3).
Intraoperative and Follow-Up Data
CI = confidence interval; SFR = stone-free rate; UCA-URSL = ureteral catheter-assisted URSL; URSL = ureteroscopic lithotripsy.
Safety
Using the Clavien–Dindo classification system, compared with the traditional URSL group, the UCA-URSL group had a lower incidence of overall surgical complications, a lower incidence of postoperative fever (>38.5°C) than the traditional URSL group (1.85% vs 15.60%, 95% CI 0.0230 to 0.4288, p = 0.0003), and a lower incidence of ureteral stenosis than the traditional URSL group (0% vs 3.67%, 95% CI 0.000 to 1.009, p = 0.04). There were no Clavien–Dindo grade III or IV complications during the operation, including ureteral injury requiring surgical intervention and septic shock.
Discussion
Our modification of traditional URSL was inspired by flexible URSL. The use of a ureteral access sheath reduces the local temperature of flexible URSL and further reduces the risk of postoperative fever and sepsis in patients. 9 UCA-URSL achieves the separation and synchronization of fluid in and out during lithotripsy. Literature reports that the incidence of complications during Ho:YAG laser lithotripsy is less than 3%, 10 and the incidence of ureteral stricture after URSL is 0.7% (0.30%–23.81%). 11 The mechanism of ureteral stricture after ureteral calculi is still unclear, and its related risk factors have not been fully elucidated. There is evidence that temperatures above 43°C are associated with the development of exponential tissue damage, which is also closely related to the duration of exposure. 12 The temperature rises rapidly after a 1-second Ho: YAG laser excitation, 13 whereas the temperature of the liquid can be increased to 43°C after a 10-second Ho: YAG laser excitation. 12 Thermal energy usually extends beyond the immediate laser absorption region 6 and can denature the urothelium, which becomes more problematic once the ureters are repaired to form scars and strictures. Intraoperative temperature monitoring is an important part of this study. In this study, the overall intraoperative temperature in the UCA-URSL group was in the safe range, whereas in the traditional URSL group, we monitored the occurrence of higher temperatures, although the incidence of postoperative ureteral stricture was higher in the traditional URSL group than in the UCA-URSL group (0% vs 3.67%, p = 0.04). However, it cannot be assumed that the ureteral stricture is due solely to the thermal effect of laser lithotripsy. In the traditional URSL group, patients with dangerously high temperatures do not necessarily have a ureteral stricture, and we speculate that it should also be related to the duration of high temperatures and the differences in the self-healing ability of individual tissues.
Other complications of URSL include infection and bleeding. High-pressure liquid renal reflux and reabsorption of infected urine may play a role, and the total fluid absorption rate of retrograde intrarenal surgery would be higher than that of percutaneous nephrolithotomy. Subcapsular hematoma and renal rupture have also been reported after holmium laser lithotripsy because of excessive perfusion pressure or pathological kidneys. Postoperative infection is one of the most common complications of URSL, and the incidence varies greatly among different studies. 14 In our study, the use of UCA-URSL significantly reduced the rate of postoperative fever, suggesting a potential advantage of this procedure in preventing infectious complications. Fever occurred in 15.6% of patients after traditional URSL, which is higher than the data reported in other literature. Although the patients included were relatively simple patients with ureteral calculi, the number of patients included in this study was still small, and the positive rate of preoperative urine culture was not low, which may cause the patients in the traditional URSL group to show a high postoperative infection rate in this study.
In vitro studies have shown that increased fluid perfusion can better control the thermal effect, but also significantly increase the intrarenal pressure. 15,16 Stone migration into the proximal ureter or kidney is a common problem during URSL, and trapping tools are usually used to prevent stone migration, 17 but the use of these devices will inevitably increase the cost of treatment. The use of the stone netting basket was reduced with catheter assistance in this study. In theory, the space for stone fragmentation in the ureteral lumen is limited. During the fragmentation process, unless the stone is in the proximal ureter, the stone fragments do not easily migrate to the kidney, which is also the consideration that patients with moderate-severe hydronephrosis and severe ureteral dilatation were not included in this study. Postoperative CT showed a lower SFR in the ureter and kidney in the traditional URSL group than in the UCA-URSL group, which we speculate is because of the increased pressure of the flush during the traditional procedure. Although there was no subcapsular hematoma and urine extravasation in the two groups, and no pressure monitoring above the stone or in the renal pelvis was performed because of ethical and treatment restrictions, there are reasons to believe that the local pressure of lithotripsy in UCA-URSL is lower but more stable.
No severe ureteral injury (large area of contusion, perforation, laceration, etc.) was found in all cases. Although mild contusion of ureteral mucosa was recorded in some traditional groups, no statistical comparison was made. We found that UCA-URSL had a better surgical field and observed less vibration at the working site of the laser fiber, which may facilitate accurate lithotripsy and may reduce accidental ureteral injuries.
The focus of this study is to try a modified irrigation method to form a local microcirculation of liquid in the lithotripsy area, reduce the local temperature, and reduce the fluid pressure burden of the upper urinary tract. In traditional URSL surgery, the water flow is often unidirectional, and the water outlet valve is intermittently opened. To ensure the safety of surgery, the stone crushing process is often interrupted, which also prolongs the operation time. For young doctors, URSL is challenging because of its fleeting timing of lithotripsy and the need to constantly explore the control of repeated water entry and exit, which requires a certain learning curve to master. In UCA-URSL surgery, the number of repeated openings and closings of the water valve is greatly reduced after adjusting the minimum water intake velocity to meet the visual field, which may be one of the reasons for the shorter operation time in the UCA-URSL group. In addition, surgeons found that UCA-URSL surgery has a better surgical field of view and higher lithotripsy efficiency, which is also the key to shortening the operation time.
Conclusions
The thermal effect of the UCA-URSL was even lower than that of the traditional URSL, which was attributed to the greater return of fluid. Compared with traditional URSL, UCA-URSL showed a better stone-free effect. UCA-URSL can reduce the rate of postoperative infection and ureteral stricture, and show better efficacy and safety. The use of UCA-URSL does not significantly increase the treatment cost but reduces the need to use a stone basket. Therefore, UCA-URSL can be used as a beneficial improvement or as an alternative to traditional URSL.
Limitations
Although the literature reported that immediate postoperative SFR was mostly evaluated by imaging examination within 24 hours after surgery, because of the potential ethical risk issues and treatment habits, patients received noncontrast CT scans within 24–48 hours after surgery to evaluate the SFR, and the same CT scan was performed 3 months after surgery to evaluate the final stone-free condition in this study. Although the engineers found that the holmium laser emitter used in this study attenuated the output energy by approximately 20% compared with the parameters shown on the screen, the power setting of 1 J/20 Hz may still be higher than the typically reported power for ureteral stone lithotripsy and may have resulted in strong local temperature increases. Ureteral mucosal edema is common in patients with calculi, and the mucosal edema has not been clearly described, and the degree of edema of the ureteral mucosa may have an effect on postoperative ureteral stricture. Because of the limitation of the software, the volume of stones and residual stones was not measured and compared. Because of economic constraints, some patients in both groups did not undergo stone composition analysis, so stone composition analysis was not included in this report. In addition, follow-up of only 3 months in some patients may limit the assessment of long-term complications such as ureteral stricture.
Footnotes
Authors’ Contributions
Z.H. and H.B.G.: Contributed equally to this paper; Y.X. and S.G.W.: Joint corresponding authors.
Ethics Approval
The study protocol was approved by the ethics committees of the First Affiliated Hospital of Kunming Medical University and Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology.
Author Disclosure Statement
All authors are responsible for the content of this article. All authors declared no competing interests.
Funding Information
This work was supported by the annual operating funding project of Provincial Scientific Research Platform, Clinical Medical Research Center (No.2022SJKY006).
Supplementary Material
Supplementary Video S1
Supplementary Video S2
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.