
Abstract
Introduction:
Focal therapy (FT) is an emerging option for intermediate-risk prostate cancer (IR-PCa). Transperineal MRI fusion laser ablation of PCa (TPFLA) is a novel FT technique with limited data reported. We conducted a phase I clinical trial evaluating the safety, feasibility, and 1-year oncologic results for patients with IR-PCa treated with TPFLA in an office setting.
Materials and Methods:
NCT05241236 aimed to evaluate TPFLA for the International Society of Urological Pathology-grade 2 (ISUP-2) tumors. All procedures were performed in the office using MR/US fusion imaging. The diode interstitial laser system fibers were applied through the perineum using local anesthesia. The primary outcome was safety and tolerability. Pain scores were recorded using analog scales. Thirty-day adverse events and 1-year prostate biopsy oncologic outcomes were noted. Functional outcomes at 3 months and 1 year were compared with baseline as well.
Results:
Thirty patients accrued had TPFLA safely in the office with no complications. TPFLA median pain score was 1. At 30 days, one man required a transurethral resection of the prostate (TURP). There were no imaging demonstrable cancers at 3 months and a significant improvement in urinary function (p = 0.001) was noted and sustained for the year. No patient experienced urinary incontinence. No changes in sexual function were observed (p = 0.7). At 1 year, 25/30 (83%) had no clinically significant cancer. However, 14 had PCa, in 5 (17%) solely in treated areas, all ISUP-1. Seven had PCa outside the treated areas. Two had infield and outfield recurrences, both were ISUP 2. At study closure, 16 patients were free from PCa, 3 were on active surveillance, 9 were treated focally with cryoablation, and 2 were converted to radical surgical procedure.
Conclusions:
TPFLA appears to be a safe and an effective focal therapy for IR-PCa, offering a potential alternative to more radical treatments with a minimal periprocedural impact. Longer follow-up and larger studies are needed to confirm these results.
Introduction
Since the U.S. Preventive Services Task Force recommendation was changed to a “C,” prostate cancer (PCa) cases in the United States have risen to 65%, with 299,000 new diagnoses in 2024. 1 Globally, cases are expected to increase from 1.4 million in 2020 to 2.9 million by 2040. 2 Localized PCa makes up 70%–80% of new cases, with a 97% 5-year survival rate. 3 Current guidelines suggest the following three approaches for this stage: active surveillance (AS), radical prostatectomy (RP), and raditaion therapy (RT). 4 The survival benefits of RP and RT are unclear from existing trials, and they have harmful impacts on quality of life (QoL). 4,5
Focal therapy (FT), introduced by Onik 6 as a PCa alternative option, has significantly evolved with improvement in prostate multiparametric MRI (pMRI). 7 Intermediate-risk PCa (IR-PCa) patients are ideal for evaluating a tailored targeted approach as they represent the most prevalent group, lack of robust data for AS-managed cohorts, face incremental conversion to aggressive approaches, and see a plausible survival benefit from radical treatments limited to younger men. Clinical guidelines are catching on to the benefits of a more measured management approach to PCa; the latest EAU recommendations now suggest focal high-intensity focus ultrasound or cryotherapy for IR-PCa only within clinical trials or prospective registries. 8
Transrectal laser ablation in-bore (performed by radiologists in MRI units) emerged as an ultra-minimally invasive (uMIST) low-risk approach to destroy localized PCa tumors proven radiologically and pathologically. 9,10 However, this approach has pitfalls, including operator dependency, lengthy general anesthesia, and procedure times ∼3 hours. 9,10 Transperineal laser ablation (TPLA) for PCa was introduced by Linder et al. 11 in a proof-of-principle study in four patients followed by RP. The results were promising, with a distinct ablation zone seen on gross examination, corresponding microscopically to homogeneous areas of coagulation necrosis surrounded by a small hemorrhagic rim. Cytokeratin 8 staining confirmed the absence of viable glandular tissue within the necrotic zones. 11 They later reported a 66% success rate in 12 low-risk patients treated with transperineal indigo laser under general anesthesia. 12
We began NCT02381990 in 2013 to evaluate the outcomes of transperineal targeted fusion cryoablation for PCa. In such, we developed office-based systems and methods to perform these procedures under local anesthesia. 13 This approach was effectively utilized in a phase I benign prostatic hyperplasia (BPH) trial. 14 Other investigators have also effectively “taken the laser out of the box,” with positive results regardless of anesthesia type or clinical setting. 15 –18 Thus, TPFLA has become an uMIST option with no adverse effects on urinary and sexual functions, and promising oncologic efficacy. Recently, a Delphi consensus suggested TPFLA as a potential effective option for IR-PCa, particularly for patients aiming to avoid urinary incontinence and sexual dysfunction. 19
In this study, we report the short-term outcomes of our phase I clinical trial, which evaluated the tolerability and safety of TPFLA in the office setting under local anesthesia for patients with IR-PCa.
Materials and Methods
NCT05698576 and NCT05241236 (ClinicalTrials.gov) represent a clinical phase I trial and a registry, respectively, designed to systematically evaluate short-, intermediate-, and long-term outcomes of PCa patients managed with TPFLA. NCT5698576, approved as CR00585489 by Advarra IRB (Columbia, MD) on March 22, 2022, is a prospective, single-center, nonrandomized, phase I trial. It rigorously evaluates the safety, feasibility, and 1-year outcomes of men treated with TPFLA. The trial was offered to newly diagnosed patients ISUP grade 2, diagnosed through transperineal MRI/US fusion-targeted plus systematic prostate biopsy. Thirty patients met the inclusion and exclusion criteria, as detailed in Table 1. They were enrolled in the trial conducted at the offices of Urology Specialist Group in Hialeah, FL, sponsored by the Urological Research Network (Miami Lakes, FL). The protocol called for an immediate post-TPFLA pMRI, followed by a pMRI at 1, 3, and 12 months. All follow-up pMRIs were conducted at Lakes Radiology (Miami Lakes, FL).
Inclusion and Exclusion Criteria of NCT05698576 Trial
ECOG = Eastern Cooperative Oncology Group, pMRI = prostate multiparametric magnetic resonance imaging.
Preoperative data
Upon enrollment, we collected data on age, clinical T (cT) stage, pMRI, Prostate Imaging-Reporting and Data System scores, lesion and prostate volume, prostate-specific antigen (PSA) levels, estimated PSA density (PSAD), and the indication for biopsy—history of PCa on AS and an elevated PSA, abnormal digital rectal examination, or both. We included biopsy data, such as the following: number of cores, number and percentage of positive cores, Gleason score, ISUP grade, millimeters of PCa found, and maximum percentage of PCa in a single core.
TPFLA procedure
The MRI and the pathological results were reviewed by an experienced radiologist and the treating urologist. As shown in Figure 1, a tailored treatment was created using the Focalyx Fusion medical device (FFMD) (Focalyx Technologies, Miami, FL), which generated a 3D mesh harboring the intended partial gland ablation zones. The ablation zones on 24/30 patients were based on the results of a TPFBx performed in the clinic and incorporated information from positive cores and its negative boundaries. For the remaining six men, the ablation zones were estimated using the correlation of MRI and biopsy findings. The FFMD enhances visualization of the ablation area and key anatomical landmarks, such as the neurovascular bundles, bladder neck, and membranous urethra. The ablation approach was tailor-made for the TRANBERG® laser (Clinical Laserthermia, Lund, Sweden), a 1064 nm diode interstitial laser with nondiffuser fibers that delivers energy flows backward from the tip of the fiber in an ellipsoid manner. We used 15 mm energy laser tip fibers and allowed for pushback if required, to cover the intended length. The FFMD provided the intended area of ablation and the number of laser applications to accomplish the goal (Fig. 1). Upon arrival, patients signed procedure consent, received antibiotics, and opted for self-administered nitrous gas anesthesia, chosen by 26 of the 30 participants. Patients were positioned in a lithotomy position, and a catheter was placed. The procedure was conducted under local anesthesia following fundamental steps described by Bianco et al. 13,20 A superficial perineal block was performed using 15–20 mL of 1% or 2% diluted lidocaine; the ultrasonography biplanar probe was placed transrectally, secured to a digital stepper with a grid; and a 21G spinal needle advanced under ultrasonography guidance to infiltrate a “deep” anesthetic block. We then focused on the laser fiber, inserting it into a sheath to expose and secure the energy tip with a small notch. The fiber was removed from the sheath, placed in a sterile safe location, whereas a sharp obturator is advanced through the sheath and placed in the sterile cart. Next, the transrectal probe was centered with the prostate visualized in both transverse and sagittal views using the FFMD. The prostate was scanned in either plane, and both views were processed and presented by the FFMD. The treating urologist marked the apex, base, and boundaries of the prostate in either plane of the acquired images. The FFMD then performed the coregistration and identified potential adjustments. Finally, the system entered “live mode,” delivering real-time fusion showing the intended treatment area and coordinates for the grid. The team and patients were instructed to apply protective eyewear. In sagittal view, the laser sheath with the obturator was advanced through the grid into the perineum, using the coordinate information. The obturator was removed leaving the sheath tip at the most distal point of the sagittal target. The fiber was then advanced to the most proximal target point. With the fiber in position, thermosensors were placed at 5 mm and 10 mm distances. We began the initial application of laser energy at 8 watts delivering 1800 joules. This ablation process took 3–4 minutes and generated bubbles, captured on imaging using the Doppler function under the FFMD perspective. The TRANBERG generator recorded the temperatures from the thermosensors. Upon completing an application, a cloud image could be seen in the FFMD. The urologists followed the plan, adjusting based on the FFMD image feedback (added applications or rolled back). Upon completing the TPFLA, all equipment was removed, the perineum cleaned, and a small dressing was applied. The patient moved to a recovery room and was discharged 20 minutes later with prescriptions for nonsteroidal anti-inflammatory drugs, antibiotics, and mirabegron. Upon discharge, the patient was transported to the radiology facility about three miles away from for a pMRI.

Step by step visual description of the TPFLA procedure. TPFLA = Transperineal MRI Fusion Laser Ablation of PCa.
During the procedure, we recorded the following: (1) in and out room times; (2) number of lesions treated; (3) total ablation time (in minutes); (4) percentage of treated volume relative to prostate volume; and (5) total energy delivered (in joules) and the J/min ratio. In addition, pain levels were assessed using a visual analog scale (0 = “no pain” to 10 = “severe pain”) before, during, and after the procedure.
Follow-up
The follow-up protocol included a Foley removal visit (5–7 days) and a 30-day pMRI and office visit to assess ablation areas and adverse events (AEs) using the Clavien–Dindo system. PSA measurements, pMRI, and urinary and sexual quality-of-life (QoL) questionnaire (QoL-Q) were conducted at 3 months and 1 year. In addition, we did PSA testing and QoL-Q at 6 months. The protocol included a transperineal fusion biopsy at the 1-year mark, using pMRI, which completed the study protocol. Treatments for patients with positive biopsy at 1 year were also documented.
Outcome measures
The primary outcomes were safety and tolerability, as previously mentioned in the article of our TPFLA technique performed in office. Secondary outcomes included the following: (1) incidence and management of AEs at 30 days; (2) absence of any type of PCa in the treated areas; (3) absence of clinically significant PCa within 5 mm of the treated areas; (4) any and clinically significant PCa detection in nontreated areas; (5) changes in functional sexual outcomes using the Sexual Health Inventory for Men (SHIM) scores and ejaculation survey; (6) changes in urinary outcomes using the International Prostate Symptom Score (IPSS), and questions 1, 5, and 12 from the EPIC questionnaires, and (7) management for either infield (tumors present within 5 mm of a treated area) and outfield recurrences.
Statistical analysis
A descriptive statistical analysis was performed. Parametric numerical variables were presented as mean ± standard deviation (SD), whereas nonparametric variables were reported as median and interquartile range (IQR). Categorical variables were expressed as numbers and percentages (n [%]). No imputations were made for missing values. Statistical analysis was conducted using SPSS Statistics version 25.0 (IBM Corp., Armonk, New York).
Results
This report describes the findings of NCT05698576 where 30 patients with IR-PCa met the I/E criteria between April 2022 and August 2023. The accrual process had two breaks (July–November 2022 and February–May 2023) related to supply chain fiber disruptions. The procedures were completed and tolerated by all patients. The median procedure time was 31 minutes (range 22–43), and ≥1 lesion was treated in 14 men, no intraoperative complications were observed, and all completed the postprocedure pMRI. There was great correlation between the execution of treatment plans and the immediate pMRI showing the hypoperfused areas, Figure 2. Over time both the prostate and the hypoperfused areas shrunk, Figure 2. Preoperative and periprocedural data are summarized in Table 2. The median prostate volume was 45 cc and ranged from 20 to 90 cc. Five patients on AS decided to participate, all had PCa progression from ISUP-1 to ISUP-2. The median PSA was 5.8 ng/mL. A median of 16 biopsy cores was taken preoperatively, with a median of 3 positive cores. The mean prostate-treated volume was 8.6 cc (±2.93) that translated into a median of 21% of the prostate treated. Pain scores were favorable as 19 (63%) reported scores of 0 or 1, 8 (27%) reported scores between 2 and 3, and the reminder 10% score was 4 or worse. Prostate swelling was noticeable, a mean and median of 49% and 55%, respectively, were seen in the pMRI done after the procedure.
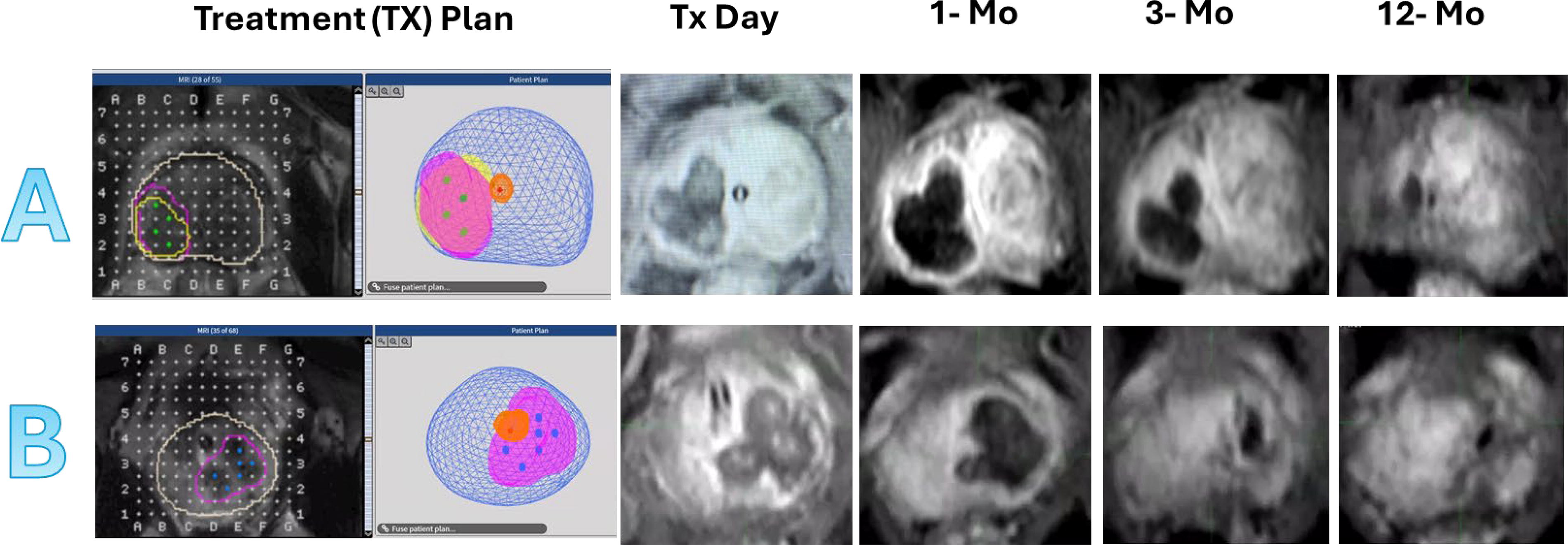
This presents serial prostate multiparametric MRIs (pMRIs) on two exemplary patients
Preoperative and Operative Data of Patients Enrolled (n = 30)
AS = active surveillance; cT = clinical T stage; IPSS = International Prostate Symptom Score; IQR = interquartile range; PCa = prostate cancer; PI-RADS = Prostate Imaging-Reporting and Data System; PSA = prostate-specific antigen; QoL = quality of life; SD = standard deviation; SHIM = Sexual Health Inventory for Men.
At the 30-day visit, 24 patients had sexual intercourse and all reported hematospermia that had subsided in 16 of them. Four (13%) patients experienced urinary retention, two patients were catheter free 14 days postprocedure, another 23 days later and one still had retention at a month an elective transurethral resection of the prostate (TURP) was performed. There were no hospital admissions.
Table 3 shows the 12 months outcomes. We observed a median PSA and PSAD drop of 50% and 46%, respectively (p < 0.01 when compared with baseline levels). pMRI showed neither discrete lesion nor enhancement in 18 (60%, p < 0.001). The reminder 12 had discrete lesions PI-RADS 3 and 4 in 8 and 4 patients, respectively. All underwent a transperineal MRI/US fusion-targeted plus systematic biopsy. No patient required an early biopsy owing to elevated PSA levels or suspicious findings on postprocedure pMRI. There were five patients with purely infield PCa all graded ISUP-1. Two patients had infield and outfield tumors, both were ISUP-2 PCa. Pure outfield detection rate was seen in seven (23%): three were ISUP-2 and four were ISUP-1. Hence, five (17%) had clinically significant PCa a year after TPFLA (Fig. 3). Six of the 18 negative pMRI patients had a positive biopsy, 3 had purely infield ISUP-1 and -3 had outfield tumors, with 2 being ISUP-2. The median PSA for positive vs negative biopsies was 2.95 ng/mL vs 2.7 ng/mL (p = 0.6).
Oncologic and Functional Outcomes: 30 Patients
Two patients had infield and outfield lesions.
Two patients had both Infield and Outfield recurrences.
ISUP-2 = International Society of Urological Pathology-grade 2; TPFLA = transperineal MRI fusion laser ablation of PCa.
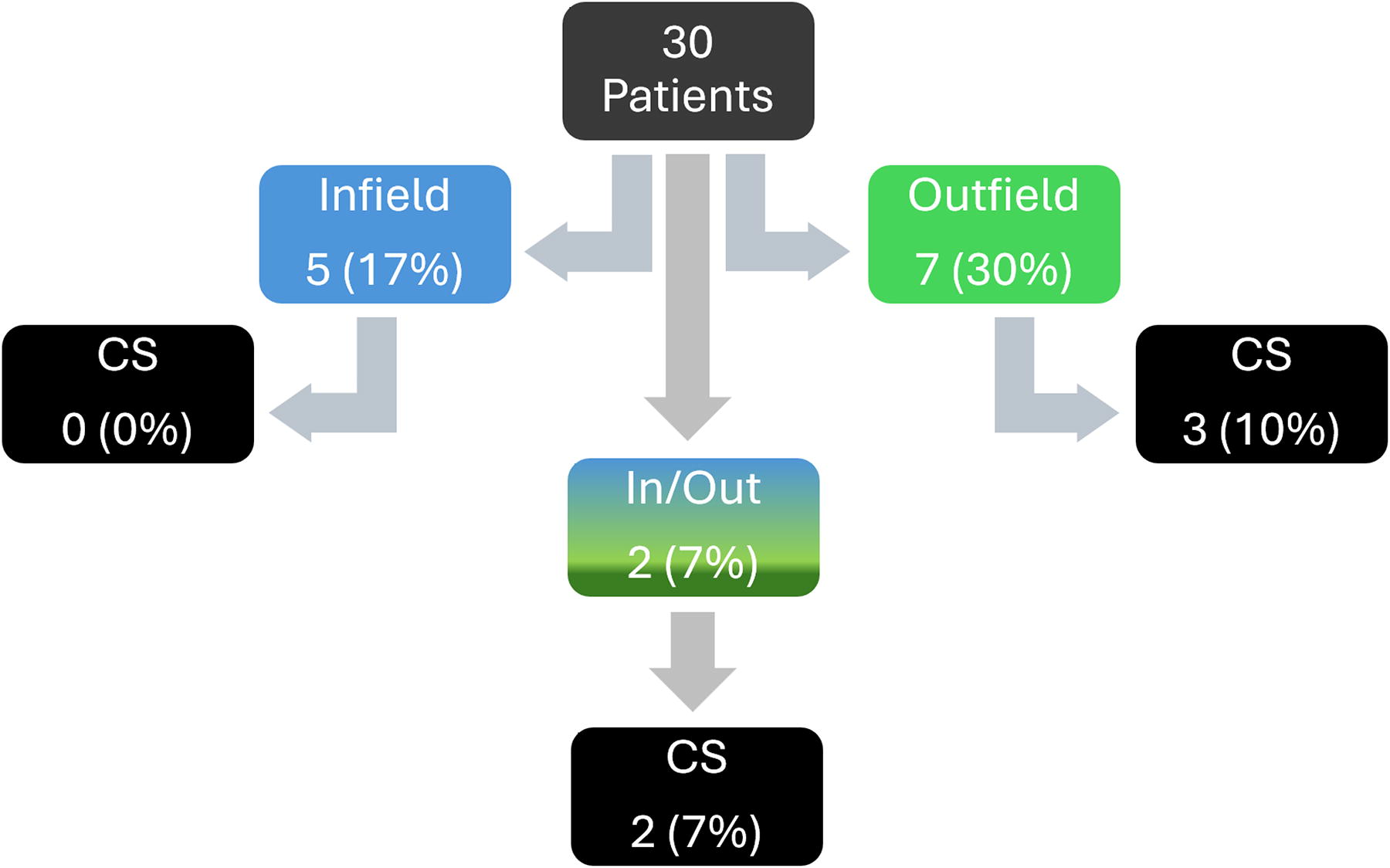
Flowchart that shows 1-year fusion biopsy results for the 30 participants.
In our analysis of functional urinary outcomes, no patient reported leakage or pad usage before TPFLA. This was sustained at 3-month and 1-year follow-ups. IPSSs did change significantly during the study as the baseline, 3-month, and 1-year median (IQR) scores were 6 (5–10), 4 (2–6), and 4 (2–6), respectively. The statistical difference was evident at 3 months (p = 0.001, Fig. 4). At baseline, 21 men were satisfied or better with their pattern of urination; however, by 3 months and 1 year, the number rose to 29 (Fisher’s exact, p = 0.005). Analysis of sexual function outcomes revealed no significant changes on SHIM scores (Fig. 4). At baseline, 3 months, and 1 year, 30, 26, and 26 men, respectively, reported erections sufficient for intercourse with or without PDE5 inhibitors. Five men used PDE5 inhibitors at baseline, with two more reporting usage 1-year post-TPFLA. At the start of the trial, all but one man reported normal ejaculations. By the end, two more reported absent ejaculation, including the patient who had a TURP. Among the 27 with ejaculation, 11 (41%) referred to a decrease in quantity.
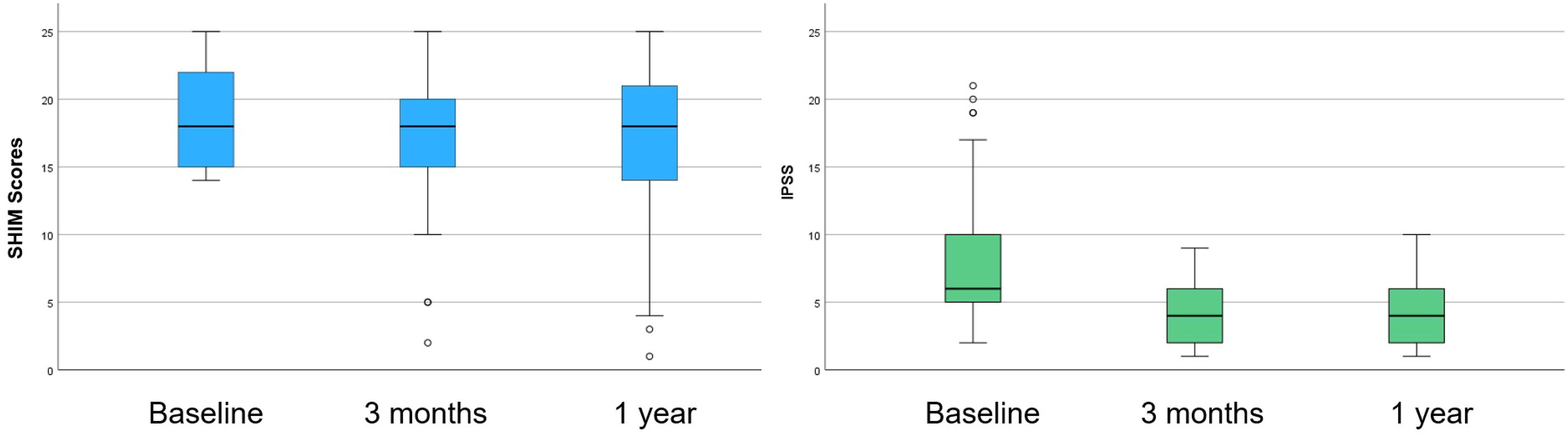
SHIM scores and IPSSs at baseline, 3 months, and 1 year post-TPFLA. IPSS = International Prostate Symptom Score; SHIM = Sexual Health Inventory for Men; SHIMNM = Sexual Health Inventory for Men—without medication; SHIM-MEDS = Sexual Health Inventory for Men—when medication is taken.
With a median follow-up of 14 months (IQR 12.5–17.3), of the 14 biopsy-positive patients, 9 were treated with MR fusion cryotherapy in the office setting, 3 with ISUP-1 were placed on AS, and 2 with ISUP-2 underwent RP.
Discussion
This phase 1 clinical trial represents the largest structured cohort of patients with single or multifocal ISUP 2 PCa treated systematically with TPFLA in an office setting under local anesthesia. The study accrued 30 men, all of whom safely tolerated the procedure with no abortions. All procedures were completed in less than 45 minutes with a median time of 31 minutes. During this time, a median of 7860 joules of energy were administered requiring a median of 5 applications. Three (10%) patients noted pain scores of 4–6, and four experienced urinary retention, with one (3%) requiring a TURP. From an oncologic perspective, 1 year after the procedure, 7% had clinically significant tumors in the treatment area. These data demonstrate the safety, feasibility, and efficacy of performing TPFLA in a medical office.
The history of TPLA for PCa is brief. The concept was pioneered by Linder et al., 11,12 whose studies with the Indigo® Optima laser showed surgical energy destruction and innovative image fusion for planning. Conducted under general anesthesia with live ultrasonography monitoring, their study showed a 33% infield recurrence in low-risk patients without significant changes in urinary or sexual functions. Natarajan S. et al. used an adapted Visualase system to perform transrectal fusion laser ablation on patients with low risk and IR-PCa in the clinic under mild sedation. 17 These procedures, lasting an hour and a half, were well tolerated, but 70% had infield positivity at 6 months with 40% being of clinical significance. 17 Renewed interest in TPFLA emerged with the recent introduction of TPLA using the Echolaser® system for BPH treatment. 14,21 This development highlighted the potential for applying the same principles to treat localized focal PCa. Similar to us, other investigators have explored various approaches for using TPLA in the management of PCa. We reviewed the current literature on this topic, including five studies plus ours, as presented in Supplementary Table S1. 12,15 –18 These represent five single-center and one multicenter assessment. 12,15 –18 Among these studies, one used the Indigo® Optima laser (800–850 nm diode laser), one used an adapted Visualase® MRI-guided FLA system (980 nm diode laser), three used the SoracteLite™ EchoLaser EVO system (1064 nm diode laser), and ours used the TRANBERG-1064 nm diode nondiffuser laser. Four were conducted in an outpatient setting, one as an inpatient procedure, and ours in an office setting. One consistent observation across these investigations was the absence of major AEs. 12,15 –18 Most observed AEs can relate to other transperineal procedures, such as biopsies where hematospermia, hematuria, and occasional hematomas occur, with urinary retention representing the most common. However, these are short lived and resolved within days. Likewise, there is a consistent lack of harm induced by laser ablation on sexual or urinary functions.
Our study carries the intrinsic limitations of a phase I clinical trial: small sample size and short follow-up, although it yields meaningful oncologic outcomes. The data demonstrate the feasibility of our management approach in the office setting. However, the long-term effects of TPFLA and major questions such as metastasis-free, cancer-specific, and overall survival are beyond this trial. Two men required conversion to radical surgical procedure, a major observation requiring meticulous follow-up in registration and further clinical trials. Our novel fusion, anesthetic techniques and treatment setting demand external validation and currently make it difficult to directly compare TPFLA with other focal therapies. Nonetheless, the data are promising and stimulate further research such as phase II trials with this energy and approach.
Conclusion
We present a novel office-based treatment approach for PCa that requires no sedation or general anesthesia, significantly reducing the procedural impact associated with other PCa treatments. TPFLA was safe, well tolerated, time efficient, and relatively easy to perform, with an acceptable AE profile. TPFLA in the office is a new concept, tailored to destroy the known cancer and preserve the healthy prostate, which translates into improved urinary function without life-altering effects in sexual function. Importantly, a year after TPFLA, cancer was downgraded or eliminated in 83% of our phase I cohort. Performing these procedures in an office setting may lower both treatment-related costs and patient anxiety.
Footnotes
Authors’ Contributions
G.M.: Conceptualization, data curation, formal analysis, original draft writing, and review and editing (equal). A.L.-P.: Data curation—review and editing (equal). G.E.-B.: Data curation—review and editing (equal). A.M.K.: Conceptualization, data curation, and supervision. E.L.G.: Formal analysis, resources, and funding acquisition. F.J.B.: Conceptualization (lead, supporting), supervision, writing—review and editing (equal), and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No specific funding was received for this study from external sources. The Urology Research Foundation supported the NCT05241236 trial (ClinicalTrials.gov).
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.