
Abstract
Introduction and Objective:
The laser direct alignment radiation reduction technique (DARRT) presents a novel approach integrating pulsed low-dose fluoroscopy, ultrasound, direct endoscopic visualization, and laser targeting to minimize fluoroscopy exposure during percutaneous nephrolithotomy (PCNL). This study aims to evaluate the safety and efficacy of laser DARRT in comparison with traditional fluoroscopic PCNL access.
Methods:
A retrospective analysis was conducted on patients who underwent PCNL. Patients with pre-existing nephrostomy tubes for access and those who underwent solely ultrasound-guided access were excluded from the study. The primary outcomes of the study were comparing fluoroscopy time used for renal access and total fluoroscopy time between the two groups. Secondary outcomes included relative stone-free rates (SFR) defined as ≤4 mm fragments on postoperative computed tomography scan and complication rates. Continuous variables were compared using an independent-sample t test, whereas categorical variables were compared using the chi-square test, with significance set at p < 0.05.
Results:
A total of 292 patients were eligible for the study. The laser DARRT reduced both access fluoroscopy time (10.8 vs 551.7 seconds; p < 0.001) and total fluoroscopy time (21.8 vs 597.7 seconds; p < 0.001). The relative SFR was significantly higher in the laser DARRT group compared with the conventional group (84.1% vs 64.1%; p < 0.001). There was no significant difference in complication rates between the two groups (p > 0.05).
Conclusions:
The laser DARRT led to a >95% reduction in access and total fluoroscopy times. By combining the advantages of fluoroscopy, ultrasound, endoscopic vision, and laser guidance, this technique represents a promising option for improving outcomes and minimizing radiation-related risk.
Introduction
Percutaneous nephrolithotomy (PCNL) is the standard of care for managing large and complex renal stones. 1 Optimal renal access is a key part of successful percutaneous stone removal. The goal is to enter the collecting system safely at a calyx that provides the best pathway to the stone. The most commonly employed methods for percutaneous renal access rely on fluoroscopic guidance. 2 Although various imaging modalities have been explored over the years to enhance percutaneous renal access, fluoroscopy maintains widespread utilization because of its versatility, ease of use, and integration in most training programs.
One concern with using fluoroscopy is high patient and staff radiation exposure. 3 The long-term risks and adverse effects of radiation exposure are well established, with up to 2% of cancers diagnosed in the United States being attributed to medical imaging. 4 Stone patients often receive computed tomography (CT) imaging for diagnosis, planning, and follow-up in addition to intraoperative fluoroscopy. Furthermore, stone patients are at risk for recurrence requiring additional imaging, placing them at even higher risk. 5
Current recommendations emphasize the “As Low As Reasonably Achievable” protocol. To mitigate radiation exposure during percutaneous renal access, we have developed a novel technique called the laser direct alignment radiation reduction technique (DARRT). 6 Following the initial description of the technique and bench-top study, we have integrated it into our surgical practice at our institution. The purpose of this study was to compare the laser DARRT with conventional fluoroscopy-guided renal access in patients undergoing PCNL.
Methods
After approval by the Loma Linda University Institutional Review Board (IRB #5220355), PCNL surgeries performed at a single academic institution between January 2017 and March 2023 were retrospectively reviewed. All procedures were performed by one of five surgeons with or without the involvement of an interventional radiologist for renal access. The study population consisted of patients with renal access established using either fluoroscopy or the laser DARRT. Three surgeons routinely used the laser DARRT for the majority of their cases during the period of the study, whereas two routinely used fluoroscopic guided renal access. Patients were included if renal access was performed prior to or during the PCNL procedure. Patients with purely ultrasound-guided access, previously established access used for second looks, or access established at an outside institution were excluded. Demographic and perioperative data were collected and compared between the groups. Stone volume (mm3) was measured using Enterprise Imaging (Agfa Healthcare, Mortsel, Belgium).
Our study focused on two primary outcomes, namely the fluoroscopy time required for initial renal access and the total fluoroscopy time. Access fluoroscopy time was defined as the period from the first fluoroscopy pedal depression until tract dilation. Total fluoroscopy time included the fluoroscopy time for access and the time spent on additional steps such as tract dilation, stone removal, and tube placement at the conclusion of the procedure.
The secondary outcomes included the absolute stone-free rate (SFR), defined as the absence of any residual fragments, and the relative SFR, defined as the presence of fragments ≤4 mm in size on a low-dose CT scan on postoperative day 1. Other recorded parameters included procedure time, estimated blood loss (EBL), blood transfusions, complications, hospital stay, secondary procedures, and stone analysis.
Laser DARRT technique
Our PCNL technique and the laser DARRT have been previously described. 3,6 Patients were positioned prone with split legs, followed by ureteroscopic real-time mapping to identify the optimal entry calyx based on angle, width, and length. Ultrasonography complemented the evaluation of renal anatomy and confirmation of the target calyx while ensuring the avoidance of pleura and abdominal viscera and allowed the determination of tract length for needle selection. During end expiration, the ureteroscope tip was positioned gently, touching the center of the papilla in the target calyx. The C-arm was set to low dose at 1 pulse per second (pps). Using limited fluoroscopic activation, the tip of a Kelly clamp was aligned with the ureteroscope tip (and subsequently the papilla of the target calyx). A laser-aiming beam emanating from the image intensifier was then positioned on the Kelly clamp tip (Fig. 1). The tip of an 18-gauge pyramidal needle and hub was then placed in line with the laser-aiming beam and inserted incrementally during the breath hold with a few activations of fluoroscopy to ensure the trajectory was on target (Fig. 2). Using ureteroscopic visualization, papillary puncture was confirmed with minor corrections performed as needed. Following this, a 0.038-inch hybrid guidewire was passed through the needle, grasped ureteroscopically, and pulled into the ureter. Using a 4-Fr Glidecath (Terumo Medical Corporation, Shibuya City, Tokyo, Japan), access into the bladder or through-and-through access was established. The Glidecath was then used to convert the hybrid wire into an Amplatz Extra-Stiff guidewire (Cook Medical, Bloomington, IN). Using a dual-lumen catheter, the hybrid wire was reinserted as a safety.
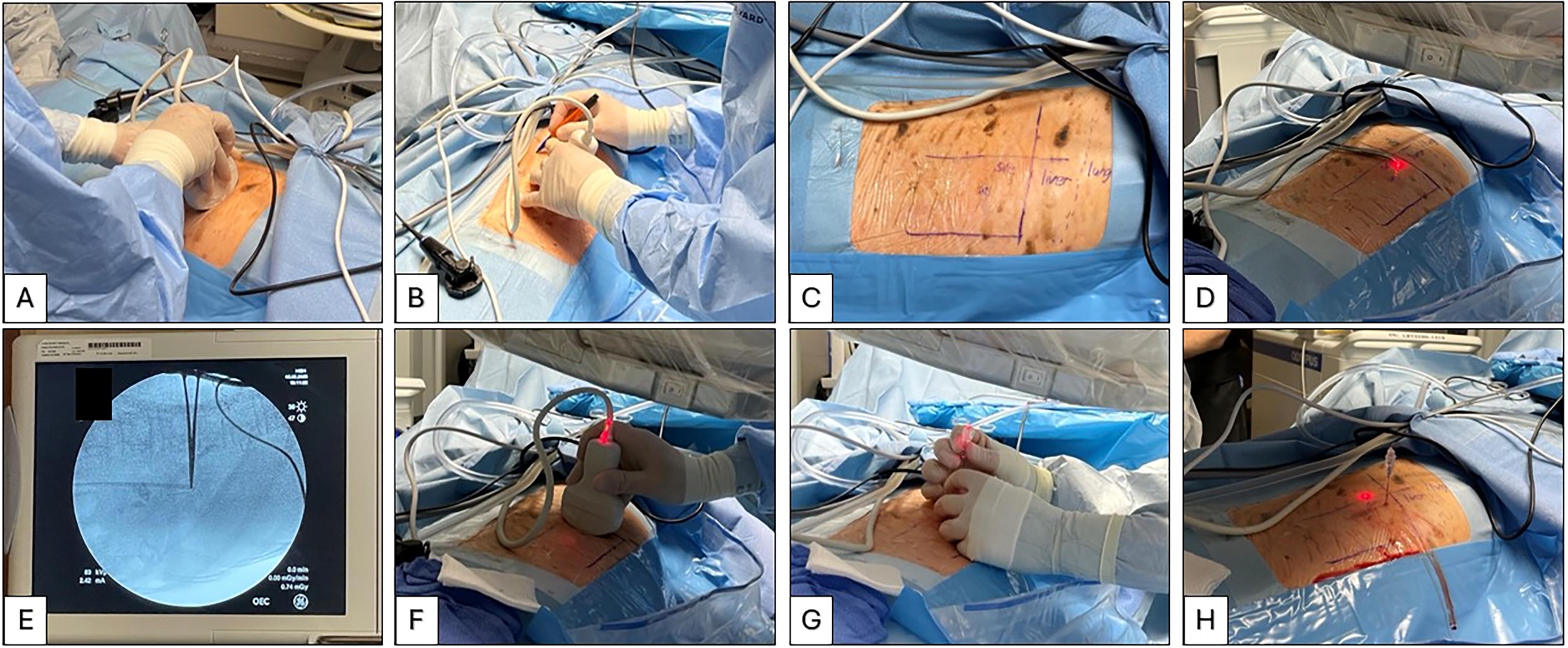
Demonstration of the steps employed for needle insertion in the laser direct alignment radiation reduction technique. (
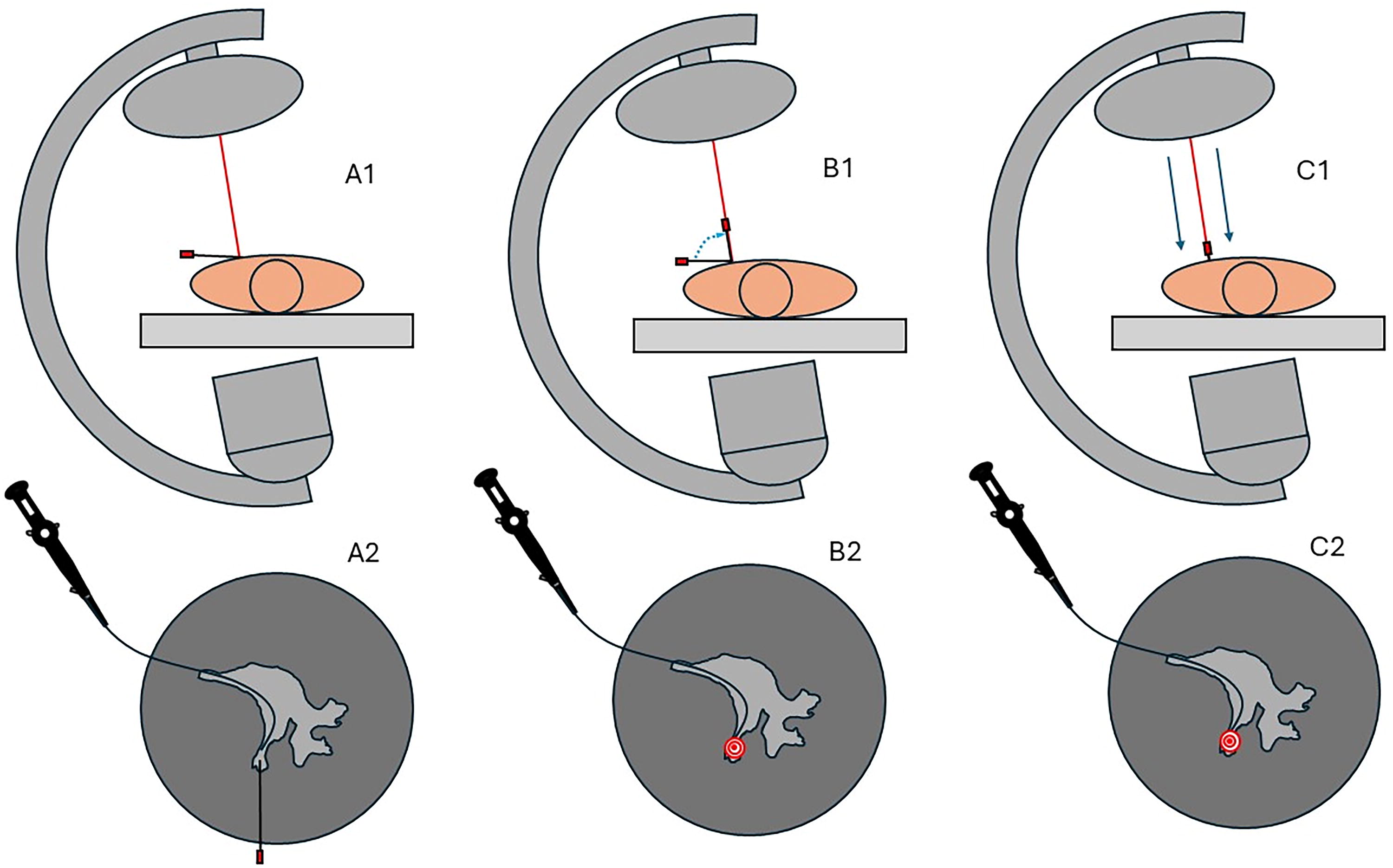
Needle alignment using the laser direct alignment radiation reduction technique. In step 1 (Figs A1 and A2), the needle is placed horizontally on the patient’s back, and its tip is aligned with the tip of the ureteroscope under fluoroscopic guidance (A2). In step 2 (Figs B1 and B2), once the tip alignment with the ureteroscope is confirmed, the needle hub is elevated to be in line with the laser beam, which appears as a “bull’s eye” on fluoroscopy (B2). In step 3 (Figs C1 and C2), while maintaining the “bull’s eye” alignment, the needle is advanced into the collecting system under direct ureteroscopic visualization.
Balloon dilation and sheath placement were performed under direct ureteroscopic visualization. Stone treatment and removal were executed conventionally, with the ureteroscope parked at the ureteropelvic junction to prevent distal stone migration. Renal mapping, conducted both retrograde and through the nephrostomy tract, ensured thorough assessment of all calyces for complete stone removal.
At the conclusion of the procedure, a double pigtail stent was routinely placed antegrade and observed ureteroscopically to confirm proper positioning. In addition, a council tip catheter was inserted as a nephrostomy and irrigated with saline to verify adequate drainage. A single tap of full-dose fluoroscopy was used to ensure that there were no radiographically visible stones. Confirmation of nephrostomy and double pigtail stent placement was obtained through low-dose fluoroscopy.
Conventional fluoroscopy-guided PCNL
In the conventional fluoroscopic approach, needle insertion was performed using a bulls-eye technique either in the operating room at the start of the procedure or in the interventional radiology (IR) suite prior to the surgery. Fluoroscopy with automatic exposure control and continuous mode was used to insert the needle and guidewire into the bladder. If access was obtained in IR, a reentry catheter was positioned in the bladder, and the patient was transferred to the operating room. In all patients, tract dilation and sheath insertion were performed in the operating room under fluoroscopic guidance with the patient in the prone position. Renal mapping, stent insertion, and nephrostomy tube placement were also performed under fluoroscopic guidance.
Statistical analysis
Baseline variables and outcomes were compared using independent samples t tests for continuous variables and Chi-squared tests for categorical variables (p < 0.05 considered significant). A generalized linear model with a Gamma distribution and a log link function was used to analyze the relationship between fluoroscopy time for access and other predictors such as overall operative time, total fluoroscopy time, access type (fluoroscopy vs DARRT), age at surgery, body mass index (BMI), surgeon, and the interaction between access type and surgeon. The Gamma distribution was chosen because the dependent variable (fluoroscopy time for access) is a continuous, positively skewed variable. Statistical analyses were conducted using R v4.4.1.
Results
Baseline characteristics
A total of 292 patients were included in this study, with 183 (62.7%) in the laser DARRT group and 109 (37.3%) in the fluoroscopy group. There was no significant difference in the mean age, BMI, American Society of Anesthesiologists score, Charlson Comorbidity Index score, or the gender distribution between the two groups (p > 0.05 for all; Table 1).
Baseline Characteristics and Stone Parameters
Continuous variables are expressed as median (IQR), and categorical variables are expressed as n (%).
ASA = American Society of Anesthesiologists; BMI = body mass index; CCI = Charlson Comorbidity Index; DARRT = direct alignment radiation reduction technique; HU = Hounsfield units; IQR = interquartile range.
Regarding preoperative stone parameters, there was no significant difference in laterality, presence of hydronephrosis, stone density, and stone volume between the two groups (p > 0.05 for all; Table 1). However, the laser DARRT group had a significantly higher proportion of staghorn calculi compared with the fluoroscopy group (84.2% vs 67%; p = 0.001).
Postoperative outcomes
The laser DARRT had lower total fluoroscopy time compared with the fluoroscopy group (13.1 vs 330 seconds; p < 0.001), a reduction of 96.6% (Fig. 3A). The fluoroscopy time for renal access was 98.5% less for the laser DARRT group compared with the fluoroscopy group (6.2 vs 405 seconds; p < 0.001; Fig. 3B). There was no significant difference in total procedure time, length of stay, EBL, and complication rates between the two groups (p > 0.05 for all; Table 2). Both absolute and relative SFRs were significantly higher for the laser DARRT group compared with the fluoroscopy group (73.1% vs 39.8% and 84.1% vs 64.1%, respectively; p < 0.001 for both; Fig. 4). There was a higher proportion of second look PCNL (12.8% vs 7.1%) or ureteroscopy (6.4% vs 2.7%) procedures for the fluoroscopy group, but statistical significance was not reached (Table 2). Postoperative stone analyses were similar between the two groups (Table 2).
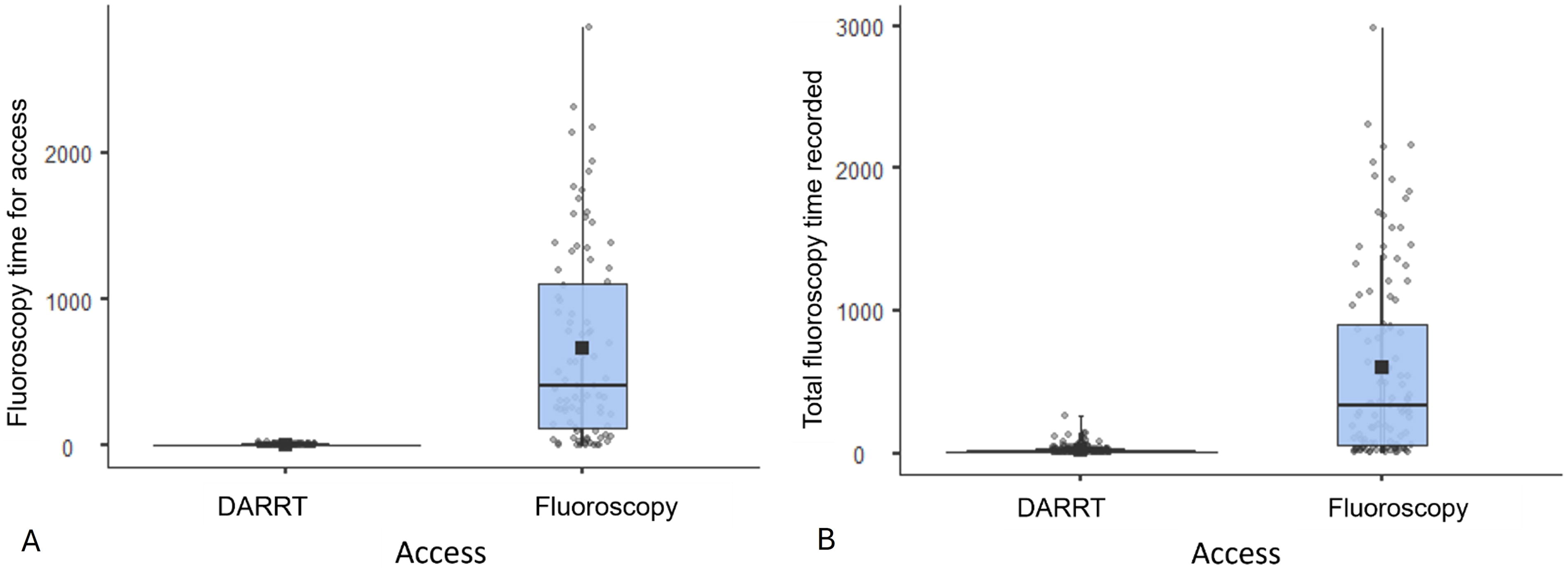
Fluoroscopy time for access

Absolute and relative stone-free rates for laser DARRT compared with fluoroscopy. DARRT = direct alignment radiation reduction technique.
Postoperative Outcomes
Continuous variables are expressed as median (IQR), and categorical variables are expressed as n (%). SFR was calculated only from patients who had postoperative CT scans performed (n = 182 in the laser DARRT group and n = 103 in the fluoroscopy group).
DARRT = direct alignment radiation reduction technique; IQR = interquartile range; PCNL = percutaneous nephrolithotomy; SFR = stone-free rate.
Univariate and multivariate analysis
In our univariate log-likelihood analysis, total fluoroscopy time and access type (fluoroscopy vs DARRT) were significant predictors of access fluoroscopy time (Table 3). The multivariate model confirmed that total fluoroscopy time and access type (fluoroscopy vs DARRT) remained significant predictors of access fluoroscopy time, even after adjusting for potential confounders such as overall operative time, age, BMI, and surgeon. The DARRT technique was associated with a 92.9% reduction in access fluoroscopy time (rate ratio 0.071, p < 0.001; Table 4), demonstrating its substantial impact on reducing radiation exposure during the procedure.
Univariate Log-Likelihood Ratio Analysis
BMI = body mass index; DARRT = direct alignment radiation reduction technique.
Multivariate Parameter Estimates and Rate Ratios Analysis
BMI = body mass index; CT = confidence interval; DARRT = direct alignment radiation reduction technique; RR = rate ratio.
Discussion
In this study, we present the first clinical description of the laser DAART renal access technique during PCNL. This method is a hybrid approach, which incorporates four distinct modalities including ultrasound, direct endoscopic visualization, low-dose pulsed fluoroscopy, and laser guidance. Our study demonstrates that the laser DARRT is safe and effective, with mean renal access fluoroscopy time reduced by 98% and total fluoroscopy time by 96.4% when compared with conventional fluoroscopic guided access as a single modality. In addition, the implementation of the laser DARRT led to higher SFRs compared with fluoroscopy-guided procedures with relative and absolute SFRs of 84% and 73%, respectively.
The laser DARRT was first described as a concept using a benchtop model in 2016. 6 Subsequently, the safety and efficacy in a clinical setting could not be fully demonstrated. The laser employed in this technique is a clinically safe, low-power laser pointer that comes standard on many C-arms or as an aftermarket modification. The laser DARRT modifies the conventional bulls-eye technique and dramatically reduces fluoroscopy during needle insertion. Upon needle alignment with limited fluoroscopy activations, the laser guidance system can maintain the needle trajectory during insertion. In addition, laser guidance permits tactile feedback as the needle passes through the renal capsule and into the collecting system without radiation exposure.
In addition, the laser DARRT facilitates the use of low-dose, pulsed fluoroscopy. In the conventional bulls-eye technique, continuous fluoroscopy is routinely required to maintain needle alignment. Because of its low density, it can be difficult to distinguish the needle hub from the tip. Subsequently, conventional automatic exposure control fluoroscopy is routinely employed. In contrast, the laser DARRT permits determination of the needle orientation in reference to the laser at the lowest dose fluoroscopy settings. In our operating room, we routinely employ the image intensifier C-arm set to low dose and 1 pps settings. By employing low-dose pulsed fluoroscopy at 1 pps, radiation exposure can be reduced by >64%. 7
Reducing radiation exposure is crucial because of its potential risks, including DNA damage and cancer development. One study on vascular and IR surgeons performing endovascular repair revealed elevated DNA damage and repair markers following a single procedure. 8 Surgeons routinely employing fluoroscopy face higher risks of breast and brain cancer. 9 Ionizing radiation induces oxidative stress, inflammation, and endothelial dysfunction, potentially leading to cardiovascular disease (CVD). 10 In addition, astronauts with no medical comorbidities exposed to cosmic radiation in deep space have increased CVD mortality compared with those completing low Earth orbit missions. 11 The average radiation dose during PCNL is 8.66 mSv with a mean fluoroscopy time of 10 minutes. 13,14 Recently, the U.S. Food and Drug Administration issued a whitepaper calling for a reduction in radiation exposure from CT and fluoroscopy. 12 Transitioning from pure fluoroscopy to the laser DARRT presents a viable approach to mitigate these health care risks.
The third component of this hybrid technique is endoscopic combined intrarenal surgery (ECIRS) to facilitate needle insertion, tract dilation, and sheath insertion under direct visualization. Improved perioperative outcomes have been reported with the use of ECIRS, which was originally introduced at Loma Linda University. 15 Subsequent reports extended technique application to anatomically complex cases, improving outcomes. 16 –19 Isac and colleagues demonstrated ECIRS reduced access attempts, bleeding rate, and fluoroscopy time by 80%. 17 In our experience, ECIRS allows selection of the optimal calyx for access and confirmation of papillary puncture. If the puncture is not papillary, corrections can be performed under direct vision without fluoroscopy. In addition, establishing bladder or through-and-through access is facilitated by retrograde basketing of the antegrade guidewire. Furthermore, by adding retrograde renal mapping, calyces that might normally be impossible to visualize through antegrade access may be easily visualized, resulting in higher SFRs.
A couple of activations of fluoroscopy are important to ensure that the angle of renal access selected is optimal to clear the majority of stone burden. In addition, the endoscopic approach ensures that the puncture is papillary, and therefore, it does not bleed and maintains better visualization throughout the procedure for optimal stone clearance and completion of the procedure. Finally, the ureteroscope from below allows surveillance of calyces that are parallel to the calyx of entry that would not be possible to access from the solely antegrade approach. All these factors explain the higher rate of SFR in the laser DARRT group.
The final component of the laser DARRT is the use of ultrasound to evaluate the pleura, abdominal viscera, renal orientation, and tract length for needle selection. Ultrasound has been shown to allow successful renal access with dramatic reductions in radiation exposure. 20,21 Isolated reports have been published using only ultrasound guidance, especially in regions where patients have low or normal BMI. 22 In contrast, patients with high BMI, staghorn calculi, absence of hydronephrosis, history of previous surgery on the same kidney, upper pole access, and anatomical variation make ultrasound-guided PCNL more challenging. 23 Most centers employing ultrasound-guided access still employ modest amounts of fluoroscopy for steps, which are difficult to do under ultrasonography alone, including tract dilation, sheath insertion, and nephrostomy tube placement. For instance, in a prospective randomized trial comparing ultrasonic vs fluoroscopic guided access for PCNL, Basiri and colleagues found a mean fluoroscopy time of 41.5 seconds in the ultrasound group. 24 Other studies have found significant fluoroscopy times in ultrasound-guided PCNL. 21 The mean renal access and total fluoroscopy times in our study were 10.8 and 21.8 seconds, respectively. Desai and colleagues in a prospective randomized study showed that ultrasound-guided renal access took longer, was more difficult to learn, and had a greater failure rate compared with fluoroscopic guided renal access. 25 In contrast, the laser DARRT was easier to learn. 26
One of the most important outcomes of PCNL is achieving a stone-free status. The laser DARRT employs the advantages of laser, fluoroscopy, ECIRS, and ultrasound to provide optimal renal access, facilitate above and below renal mapping, and ensure ureteral clearance to optimize SFRs. This was demonstrated in our study where, despite having more complex stone disease, the laser DARRT patients had approximately 20% higher SFRs. These SFRs are comparable with the published literature 27 and higher than ultrasound and ECIRS combined. 22,28
Our study is limited by its retrospective design. Another limitation is the variability introduced by the involvement of different surgeons and IR in performing the procedures. Nevertheless, subsequent multivariate analyses demonstrated that the laser DARRT remained an independent predictor of shorter fluoroscopy times and higher SFRs. This technique was not tested for supine PCNL, and its utility in this position remains to be defined. In addition, not all C-arms have a laser pointer, although it can be easily added. Finally, ECIRS may not be feasible in all patients including those with ureteral strictures and ileal conduits.
In conclusion, the laser DARRT reduced mean renal access fluoroscopy time by 98% and total fluoroscopy time by 96.4% for PCNL without compromising other surgical outcomes. The laser DARRT is easy to learn and safe and represents a promising approach for improving PCNL outcomes.
Footnotes
Authors’ Contributions
D.D.B.: Conceptualization; A.R., A.F., G.S., M.B., A.S.A., and V.G.: Data curation; A.F., A.S.A., and U.O.: Formal analysis; Z.O., R.L., K.S., D.S.B., and D.D.B.: Investigation; A.S.A. and D.D.B.: Methodology; A.F., M.B., and A.S.A.: Project administration; D.S.B. and D.D.B.: Resources; Z.O., A.S.A., and D.D.B.: Supervision; A.F., M.B., and A.S.A.: Validation; K.S., R.L., G.S., and V.G.: Visualization; Z.O., A.R., A.F., R.L., M.B., A.S.A., K.S., V.G., and D.D.B.: Writing—original draft; Z.O., A.F., and D.D.B.: Writing—review and editing.
Author Disclosure Statement
D.D.B. holds a patent for laser-guided needle targeting.
Funding Information
There was no funding for this study.