
Abstract
Purpose:
To determine the feasibility and safety of a new domestic single-port surgical robot in urologic partial nephrectomy and radical prostatectomy, as measured by the primary metric outcome (surgical success rate). In addition, this study measured important perioperative surgical outcomes, such as operative time, blood loss, postoperative length of stay, docking time, and thermal ischemia time, and reported pathologic data using the surgical robot.
Materials and Methods:
This prospective, single-center, single-group clinical study was conducted between August 2023 and October 2023. One surgeon used a new domestic single-port surgical robot (EDGE SP1000) to perform six urologic procedures, including three partial nephrectomies and three extraperitoneal radical prostatectomies. Perioperative data were prospectively recorded, early oncologic outcomes were assessed based on the surgical margin status, and equipment ergonomic comfort was assessed using the National Aeronautics and Space Administration Task Load Index (NASA-TLX).
Results:
All six procedures were effectively completed without conversion to open surgery, laparoscopy, or use of multiport robots. The average total operation time was 207.92 ± 32.42 minutes, estimated blood loss was 100 mL (10–900 mL), and postoperative hospital stay was 8.67 ± 1.33 days. The average docking time was 16.25 ± 5.68 minutes, and warm ischemia time was 17.00 ± 2.65 minutes. None of the patients required perioperative blood transfusion. All pathologic examination margins were negative. No serious perioperative complications occurred (Clavien–Dindo grade 3). The surgeon reported that the device was comfortable to use, with a NASA-TLX score of 35.67 ± 4.23.
Conclusions:
It is safe and feasible to perform urologic procedure using the EDGE single-port endoscopic surgical robot (EDGE SP1000) control system.
Introduction
With the development of minimally invasive surgery, the need to achieve less trauma and better perioperative results, and the advantages of single-port technology and multiarm robotic surgery, robotic single-port surgery has emerged. 1,2 However, it is associated with some disadvantages, including space congestion, interference between instruments, and difficulty in establishing an operating triangle. 3 Therefore, the Intuitive Surgical Company redesigned the architecture of the surgical robot and launched the da Vinci SP single-port system, which has achieved positive results in the fields of urology, obstetrics, gynecology, and general surgery. 4,5
In China, surgical robots have shown a rapid development trend since 2019. 6 Domestic single-port systems such as the Shurui single-port robot, EDGE SP1000, and Tumai SA1000 are being rapidly developed and clinically tested. 6 In 2020, the Shurui single-port robot underwent clinical trials in radical prostatectomy and partial nephrectomy, 7,8 and its safety and effectiveness have been verified. The newly developed SP robotic surgical system (EDGE SP1000, Shenzhen Jingfeng Medical Technology Co., Ltd., Shenzhen, China) features an integrated single-arm, single-port design, making it more compact. Its “sleeve concealment” technology enhances the robot’s ability to handle lesions near the abdominal wall. It has one mechanical arm, capable of providing three flexible instruments and a 3D high-resolution camera for operations and visibility in narrow working spaces. The feasibility and safety of the system have been demonstrated in urologic and gynecologic procedures using porcine models. 9,10 From 2020 to the present, the EDGE SP1000 has been tested in model pigs and humans at the Department of Obstetrics and Gynecology and the Colorectal Department in Zhongnan Hospital of Wuhan University; the safety and feasibility of the robotic system were initially evaluated. The scope of its applications has gradually expanded to the field of urology.
The present study aimed to evaluate the feasibility and safety of the EDGE SP1000 surgical system in partial nephrectomies and radical prostatectomies and present our institution’s initial experience with the robotic system in these two procedures.
Materials and Methods
Our prospective, single-center, single-group clinical research protocol was approved by the Medical Ethics Committee of Zhongnan Hospital of Wuhan University (approval no. 2023016). Informed consent was obtained from all the patients. All enrolled patients had definite indications for urologic surgery and no contraindications for laparoscopic surgery.
Six urologic inpatients were treated between August 2023 and October 2023. All procedures were performed by the same urologist with experience in over 500 multiarmed robotic procedures. In addition, the surgeon underwent training in the EDGE SP1000 dry laboratory, wet laboratory, and animal testing processes before the commencement of the clinical procedures.
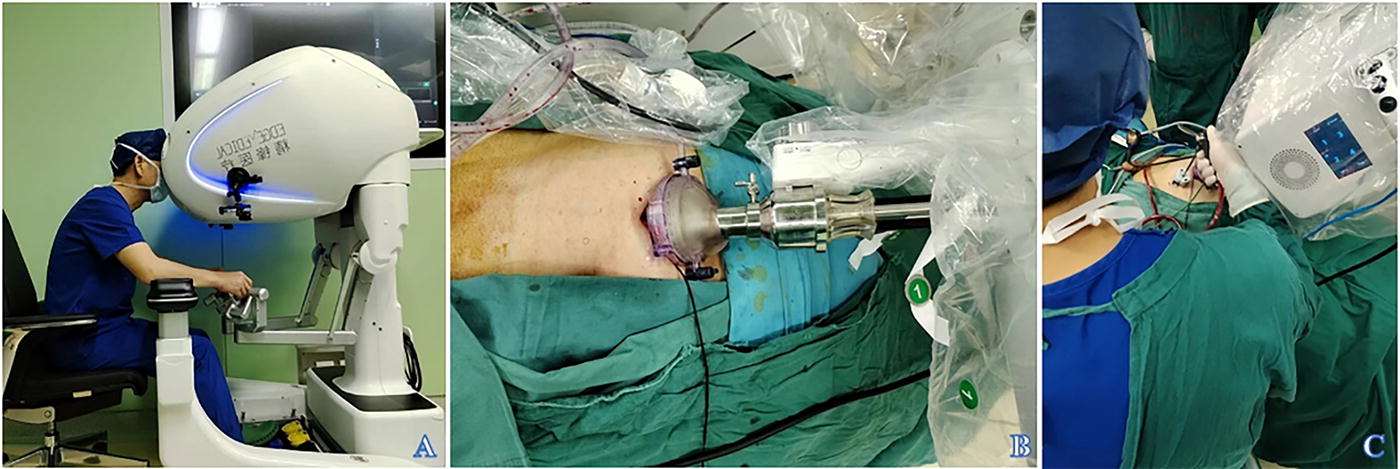
Perioperative clinical data were prospectively collected and analyzed using descriptive statistics. Preoperative data included age, body mass index, preoperative diagnosis, biochemical tests, and biopsy Gleason score, whereas intraoperative data included docking time, operative time, estimated intraoperative blood loss, and intraoperative complications. Postoperative data included drain duration, postoperative complications, positive surgical margins, pathologic findings, postoperative biochemical test results, and length of postoperative hospital stay. Based on the Clavien–Dindo grading criteria, surgical complications were deemed serious if a grade of 3 or higher was recorded. Operator satisfaction with the use of instruments was measured using the National Aeronautics and Space Administration Task Load Index (NASA-TLX), following the calculation method proposed by Fan et al. 11 As shown in Figure 1, the EDGE SP1000 consists of the following three parts: surgeon’s console, patient’s surgical platform, and a three-dimensional high-definition imaging system.

The EDGE single-port endoscopic surgical robot (SP1000).
Six urologic surgical treatments were performed in this study as follows: three partial nephrectomies and three radical prostatectomies. All partial nephrectomies were performed using the retroperitoneal approach, whereas radical prostatectomies were performed using the extraperitoneal approach. The operator was seated in front of the surgeon’s console (Fig. 2), while the assistant stood beside the patient’s surgical platform.
To perform a partial nephrectomy, the patient was placed in the lateral position, a 2-cm transverse incision was made in the midaxillary line, four fingers above the iliac crest, and a single-port robotic trocar was inserted. A 12-mm trocar was inserted in the flat first incision in the anterior axillary line as an auxiliary hole, the retroperitoneal fat was separated ventrally, and the lateral vertebral fascia was opened to expose the lumbar psoas major muscle. The lumbar psoas major muscle was then separated downward to the level of the anterior superior iliac spine. The wound was sutured using barbed sutures. After mobilization of the renal artery, pararenal fat was opened to fully expose the tumor. The renal artery was clamped with bulldog clamps. The tumor was resected, and the excised kidney was sutured with continuous running sutures. Bulldog clamps were removed after proper hemostasis. The specimen was removed, the drain was inserted, and the incision was closed layer-by-layer (Fig. 3).
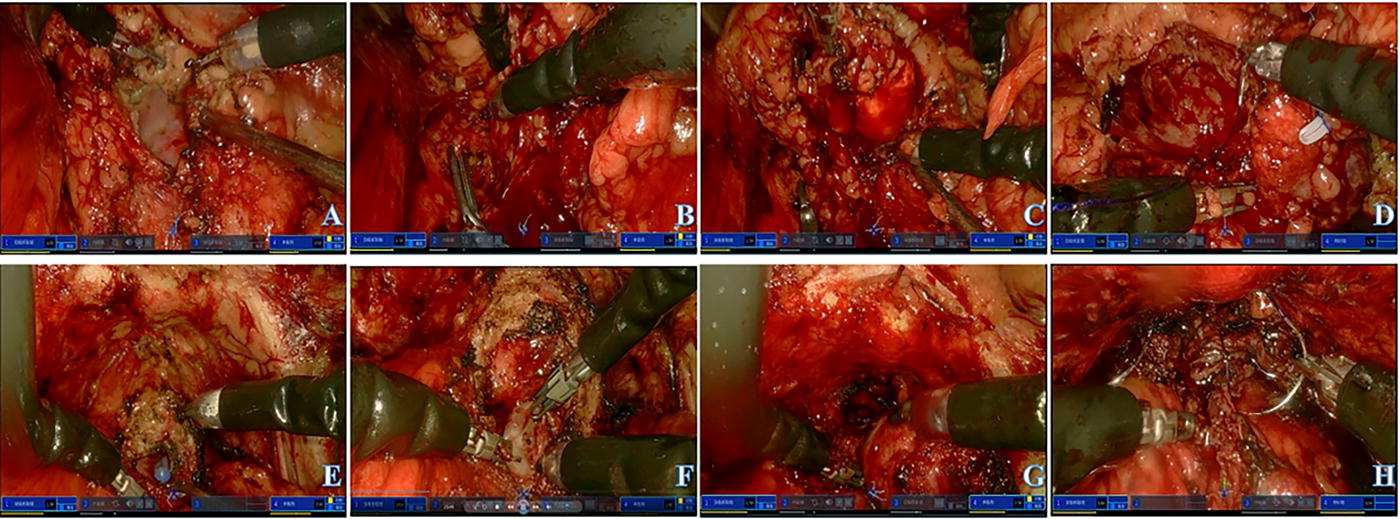
Intraoperative steps:
During radical prostatectomy, the patient was placed in the supine head-down and feet-high position, a 3-cm longitudinal incision was made on the midline of the lower edge of the umbilicus, and a 12-mm auxiliary hole trocar was placed next to the left rectus abdominis. Fat and loose tissues were removed from the bladder neck, prostate surface, and pelvic floor fascia, and the ventral and both sides of the prostate were separated. The vesico-prostatic junction was identified by pulling the urinary catheter and divided, after which vesicourethral anastomosis was performed. The prostate was dissected along the gap between the anterior and posterior layers of Denonvilliers’ fascia, the bilateral seminal vesicles were exposed and freed, and the vas deferens was isolated. The gap between the pelvic fascia and the prostate capsule was gradually dissociated to the tip of the prostate, and the urethra was cut off. After the urethral balloon was exposed and the prostate was completely freed, urethrovesical anastomosis was performed, and the entire thickness was intermittently sutured with 2–0 absorbable sutures. With no active bleeding in the surgical area, an extraperitoneal drain was inserted, and the incision was closed layer-by-layer (Fig. 3).
Results
Based on the inclusion and exclusion criteria, three partial nephrectomies and three radical prostatectomies were performed using the EDGE SP1000 system from August to October 2023. There was no conversion to traditional laparoscopic, multiarm robot-assisted or open surgery. None of the patients with prostate cancer (PCa) underwent pelvic lymph node dissection. No serious complications occurred during or after the procedures. Perioperative results are shown in Table 1.
Demographic Data, Clinical Characteristics, and Perioperative and Pathologic Data of Included Participants
RA radical prostatectomy = robot-assisted prostatectomy via extraperitoneal approach; RA partial nephrectomy = robot-assisted partial nephrectomy via retroperitoneal approach; PCa = prostate cancer; BMI = body mass index; SCr = serum creatinine; Hb = hemoglobin; OT = operating time; EBL = estimated blood loss; WIT = warm ischemia time; GS = Gleason score; RK = right kidney; LK = left kidney; ccRCC = clear cell renal cell carcinoma; PSA = prostate-specific antigen.
The average total operation time (OT) was 207.92 ± 32.42 minutes, the average time for prostatectomy was 232.50 ± 10.10 minutes, the average time for partial nephrectomy was 183.33 ± 13.02 minutes, and the average docking time was 16.25 ± 5.68 minutes. An additional auxiliary hole was created during surgery. The visual pain score 24 hours after surgery was 2.50 ± 0.72, and the patient routinely used propacetamol hydrochloride for analgesia postoperatively.
Patient 1 was diagnosed with a left renal hamartoma in the rupture and bleeding absorption phases before the procedure. Intraoperative blood loss was 900 mL; intraoperative vital signs were stable, and postoperative routine blood tests showed hemoglobin (Hb) 10.1 g/dL.
Surgeon satisfaction with instrument operation during the study period was assessed using the NASA-TLX scale. The total score, psychologic demand, physical demand, time demand, performance, effort, and frustration scores were 35.67 ± 4.23, 3.00 ± 0.89, 2.67 ± 0.82, 3.33 ± 1.03, 20.33 ± 0.52, 4.00 ± 1.41, and 2.33 ± 0.52, respectively (Table 2).
The National Aeronautics and Space Administration Task Load Index Score
NASA-TLX = the National Aeronautics and Space Administration Task Load Index.
All patients returned to the hospital for review 4 weeks after discharge as planned and underwent relevant laboratory tests (blood routine, blood biochemistry, urine routine) and vital sign measurements, which showed no obvious abnormalities. There were no emergency admissions within 1 month after the operation. In addition, none of the patients was readmitted. Patient and Observer Scar Assessment Scale (POSAS) subjective assessment results of bidirectional scars showed a Patient Scar Assessment Scale score of 28.50 ± 5.41 and an Observer Scar Assessment Scale score of 20.67 ± 1.60. One patient newly developed gastroenteritis, which was mild and resolved without the need for medical intervention. The remaining patients experienced no additional discomfort, and no new adverse events occurred.
Discussion
The single-port surgical robot is the latest advancement in surgical robot technology aimed at reducing invasiveness in surgical procedures. 12 To further reduce surgical invasiveness, a new robotic platform was specifically designed for single-port surgery. This study preliminarily evaluated the application of the EDGE SP1000 system in urologic surgery, showing that it is safe and feasible for partial nephrectomy via a retroperitoneal approach and radical prostatectomy via an extraperitoneal approach.
There were no changes in the surgical methods in the six cases, and no serious surgical complications occurred during the perioperative period. None of the patients required emergency admission or readmission within 1 month of postoperative follow-up. Only one patient developed new gastroenteritis, which was unrelated to the device used in this study and was not a complication or adverse event related to the procedure. The remaining patients did not experience any other discomfort or adverse events. Thus, the safety of the device was verified to a degree.
This was the first clinical trial of the EDGE SP1000 system in human surgery at the Department of Urology. The average OT was comparable with the results of Kaouk et al.’s first use of the da Vinci SP surgical control system in 2018. 13 The average blood loss of the patients in the present study was 100 mL (range 10–900 mL), and no blood transfusion was required. We did not specifically exclude patients with special circumstances; therefore, Patient 1 had a hamartoma accompanied by rupture and bleeding, and the patient’s intraoperative bleeding volume was as high as 900 mL. Routine blood tests were reviewed after the operation, showing Hb 10.1 g/dL; blood loss was within the acceptable range. In partial nephrectomy, every minute is important. 14 Three patients with partial nephrectomy had a thermal ischemia time of 16 (15, 20) minutes, which was controlled within 20 minutes. The application of the SP1000 system reduces the thermal ischemic time, potentially lowering kidney damage caused by reperfusion injury due to warm ischemia.
Kaouk et al. emphasized that there is a learning curve for single-port robotic surgery 13 and a certain amount of time is needed for interteam cooperation. In the present study, the average docking time was 16.25 ± 5.68 minutes, similar to that of Chen et al., who used the EDGE SP1000 for an obstetrics and gynecology procedure, where the average docking time was <21.3 ± 3.4 minutes. 15 With better teamwork and control of the equipment, docking time can improve gradually.
Excellent pain control is one of the advantages of single-port robots. A 2020 study comparing the perioperative outcomes of a multiarm robotic system with those of a single-port robot showed that pain control on the first postoperative day of single-port surgery was better than that of the multiport robot-assisted laparoscopic prostatectomy (MP-RALP). 16 In this present clinical trial, postoperative pain was assessed using patients’ subjective visual analog scale, with a score of 2.50 ± 1.76; postoperative analgesia was routinely provided with propacetamol hydrochloride, with no additional need for opioid analgesics. The results showed that the EDGE SP1000 surgical robot system may optimize the postoperative pain control problem. Li et al. suggested an inevitable high degree of heterogeneity in the number of patient hospitalization days. 17 According to the patient’s postoperative hospital stay in our hospital, we judged that the patient’s postoperative length of stay with the EDGE SP1000 system was 8 (6, 10) days, and the postoperative hospital stay was not significantly different from that of similar procedures. The da Vinci SP system was the first single-port robotic system to be applied in clinical practice. 18 The surgical margins in all six cases in the present study were negative; however, subsequent follow-up for oncologic outcomes is ongoing.
The cosmetic outcome of the postoperative wound is another advantage of single-port robots. Kim et al. demonstrated that the da Vinci SP has a high satisfaction rate for cosmetic outcome postoperatively with an incision of approximately 3 cm. 19 One-month follow-up results after treatment with EDGE SP1000 showed that all patients had no readmission; participants’ and reviewers’ viewpoints were integrated by the POSAS bidirectional scar subjective score, which resulted in higher satisfaction with the skin scar. We assessed the subjective comfort of the surgeon by the NASA-TLX scale, and the NASA-TLX score was 35.67 ± 4.23, which demonstrated the excellent ergonomics of human surgery using the EDGE SP1000 system. In addition, the overall comfort level of the surgeons was satisfactory.
Several technical challenges remain in this preliminary clinical study. First, teams in the early stages of the learning curve of the single-port technique are better aided by an extra assistant port. In this study, the tumor was resected using a single-port approach, and the extra assistant port was only intended to assist in the visualization of the operative field and control of substantial hemorrhage to avoid the console surgeon spending additional time controlling the suction device and visualization of the operative field. Second, at the beginning of the PCa procedure, the endoscopic lens was oriented with a 30° mirror downward for better field control, whereas during anastomosis of the bladder and urethra, it was preferable to orient the endoscopic lens upward for better visualization. Finally, it remains emphasized that even experienced multiarm robotic operators need to undergo systematic adaptive training to strengthen the use of clutch pedals and recognition of instrument positions, the instant display of the position of each arm on the screen to minimize collision of instruments. In addition, during the training period of teamwork and docking practice, the operator should take the initiative to form good cooperation between the operator and the assistant, and it is desirable that sufficient control of instruments be achieved outside the operating room.
Overall, the operation space of extraperitoneal and retroperitoneal approaches is narrow, and resection and suturing via these two approaches are more difficult than those via the transperitoneal approach. A single-port surgical robotic system offers unique advantages that overcome the limitations of multiport surgical systems, such as external limited space and instrument collisions. 20 During the rapid extension of multiport surgical robots, single-port robots have become a new direction and competitive platform for the development of minimally invasive surgery. The current trend is to develop new single-port robot platforms to reduce surgical invasiveness. 21
The present study had some limitations. First, only a few cases were included. Second, only one surgeon performed all the procedures at our institution. Comparative studies of single-port vs standard multiarm surgical robotic systems need to be designed and should be considered in the future. Although the postoperative pathologic results were favorable, a long-term follow-up plan and the development of studies with larger sample sizes would be more conducive to validating the new surgical platform. The development of the single-port surgical robot may redefine the standard procedure for narrow-gap procedures due to its unique operational advantages.
Conclusions
The preliminary clinical results of this study demonstrate that the EDGE SP1000 robotic system is feasible and safe for performing partial nephrectomy and radical prostatectomy. More controlled trials with larger sample sizes and long-term follow-up results will be beneficial for validating these conclusions.
Footnotes
Acknowledgments
The authors would like to thank all the patients in this study.
Ethical Approval
This study was approved by the Medical Ethics Committee of Zhongnan Hospital of Wuhan University (ID: 2023016). All participants received detailed information about the study and signed an informed consent form.
Authors’ Contributions
L.Z.: Writing—review and editing, writing—original draft, and visualization. H.Z.: Writing—review and editing, writing—original draft, and visualization. Z.W.: Writing—review and editing. H.Z.: Writing—review and editing. K.Y.: Conceptualization, funding acquisition, and writing—review and editing. X.W.: Conceptualization, funding acquisition, and resources.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.
Funding Information
This work was supported by Wuhan University “351” Talent Program Project Funding.